Avicenna J Dent Res. 11(3):108-110.
doi: 10.34172/ajdr.2019.21
Case Report
A Successful Root Canal Therapy of a Maxillary Lateral Incisor With 2 Root Canals: A Case Report
Hamed Karkehabadi 1  , Faraz Moradi 1 , Razieh Salehi 1, * , Leila Ghasemi 1
, Faraz Moradi 1 , Razieh Salehi 1, * , Leila Ghasemi 1
Author information:
1Department of Endodontics, Dentistry School, Hamadan University of Medical Sciences, Hamadan, Iran
Abstract
Background: Complete debridement is the major key to successful non-surgical endodontic treatment in teeth with periapical lesions. The missed canals serve as a harbor for bacteria and the irritant factors that lead to treatment failure. Most anatomical studies found that the maxillary lateral incisor is a single-rooted tooth. Most cases reported about the maxillary lateral incisors with two roots are the result of fusion or gemination and are usually accompanied by an enlarged crown. However, a few studies reported that the crown dimensions were normal. Knowing this unusual anatomy helps clinicians to treat patients more efficiently with less chance of failure.
Case Presentation: This case report describes successful endodontic management of an uncommon variation of the maxillary lateral incisor with two root canals. Based on the clinical and radiographic findings, pulp necrosis and symptomatic apical periodontitis were diagnosed. The tooth received root canal treatment. The patient was followed up for 6 months and clinical and radiographic examinations in the follow-up sessions showed improvement in the periapical condition and the tooth became asymptomatic.
Conclusions: Due to the wide morphological variations in the root and the root canal system of the teeth, clinicians should have knowledge of any anatomical variation to minimize the risk of endodontic treatment failure following inadequate debridement of indistinguishable or inaccessible portions of the root canal system.
Keywords: Two-rooted maxillary lateral incisor, Root canal therapy, Anatomical variation
Copyright and License Information
© 2019 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Citation: Karkehabadi H, Moradi F, Salehi R, Ghasemi L. A Successful Root Canal Therapy of a Maxillary Lateral Incisor With 2 Root Canals: A Case Report. Avicenna J Dent Res. 2019;11(3):108-110. doi: 10.34172/ajdr.2019.21.
Background
Highlights
-
Due to the wide morphological variations in the root and the root canal system of the teeth, clinicians should have knowledge of any anatomical variation to minimize the risk of endodontic treatment failure following inadequate debridement of indistinguishable or inaccessible portions of the root canal system.
One of the most important objectives of the endodontic non-surgical treatment is to remove the infection from the root canal system and prevent re-infection of the root canal system. In fact, endodontic treatment can fail for some reasons, including misdiagnosis, persistence of root canal infection, incomplete debridement and root canal shaping, instrument fractures, and poor restoration. Therefore, it is very important to have knowledge of intradental anatomy in order to achieve a correct endodontic treatment (1). Most anatomical studies found that the maxillary lateral incisor is a single-rooted tooth (2). Although multiple case reports indicated significant variations in the tooth anatomy, most of the cases reported in the literature about the maxillary lateral incisors with two roots are the result of fusion or gemination and are usually accompanied by an enlarged crown. However, a few studies reported that the crown dimensions were normal (3). This study aimed to report a clinical case of endodontic treatment of a lateral maxillary incisor with two roots and two canals.
Case Presentation
An 11-year-old girl with a complaint of tooth sensitivity when chewing referred to Hamedan School of Dentistry for root canal treatment of the left maxillary lateral incisor (Figure 1). Clinical examinations indicated normal dimensions of the lateral incisor crown on both sides. Moreover, there was no evidence of a developmental radicular palatal groove. In addition, the tooth did not respond to vital pulp tests and was sensitive to percussion. Radiographic examination showed caries in the mesial aspect of the crown. Actually, the mentioned tooth had abnormal root morphology with two separate roots (mesial and distal), whereas the contralateral tooth had normal morphology. Furthermore, radiolucency was seen around the mesial root (Figure 2). Based on the clinical and radiographic findings, pulp necrosis and symptomatic apical periodontitis were diagnosed. Following a discussion with the patient and her parents and obtaining informed consent from the patient’s parents, non-surgical root canal treatment was planned. After infiltration anesthesia with 1.8 mL of 0.2% lidocaine with 1:80 000 epinephrine, the tooth was isolated using clamp and rubber dam and access cavity preparation was done using high-speed diamond bur under water spray conditions. Then, the working length was measured by the apex locator (Root ZX, Morita, USA) and was confirmed by radiography. The canals were cleaned and shaped using the crown-down technique with Protaper System (Dentsply, Maillefer, Ballaigues, Switzerland) to size 40 for the distal root and 25 for the mesial root. It is notable that the canals were constantly irrigated with 5.25% sodium hypochlorite solution. Finally, after drying with a paper point, the canals were obturated with gutta-percha (Gapadent, China) and AH26 sealer (Dentsply-Maillifer, Ballaigues, Switzerland) by lateral condensation technique (Figure 3). Then, glass-ionomer cement (GC, Japan) was used as a temporary filling material and after the final radiography, the patient referred to the restorative department for the final restoration. The patient was followed up for 6 months and clinical and radiographic examinations in the follow-up sessions showed improvement in the periapical condition and the tooth became asymptomatic (Figure 4).

Figure 1.
Clinical picture depicting normal anatomic form of right and left maxillary lateral incisors
.
Clinical picture depicting normal anatomic form of right and left maxillary lateral incisors
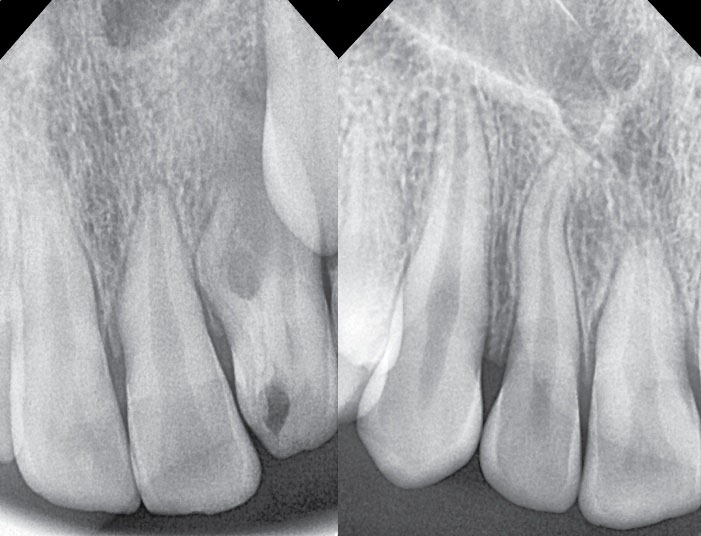
Figure 2.
(a) preoperative radiograph showing an extra root in relation to left maxillary lateral incisor, and (b) contralateral tooth with normal morphology
.
(a) preoperative radiograph showing an extra root in relation to left maxillary lateral incisor, and (b) contralateral tooth with normal morphology
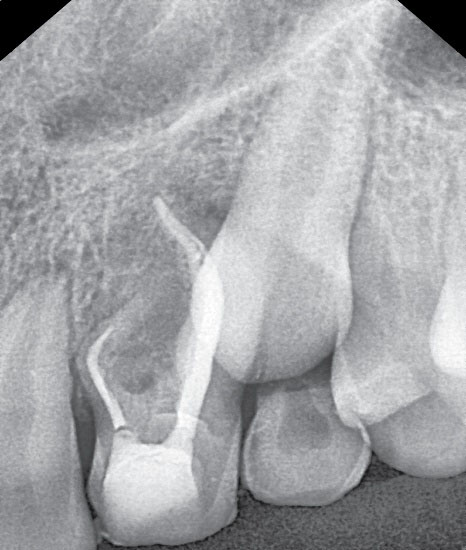
Figure 3.
Final radiograph after root canal therapy
.
Final radiograph after root canal therapy
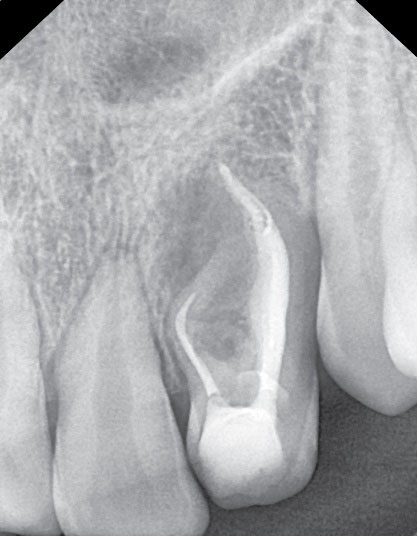
Figure 4.
6 months follow-up radiograph
.
6 months follow-up radiograph
Discussion
The present report indicated a rare maxillary lateral incisor with two canals without crown abnormalities. According to the literature (4), there is no limitation to the morphological variations of the root canal. In order to consider anatomical variations in the number and form of the canal system, this hypothesis is necessary for clinicians. Findings demonstrated that the presence of more than one canal is rare in the central and lateral maxillary incisors. In fact, studies (5) revealed that 100% of these teeth have single canal, though a review of reports (6) indicated that 3% of the maxillary lateral incisors possibly had two canals. In fact, when a maxillary incisor with two roots and two canals are observed, conditions such as fusion (7), gemination, dens in dent, palatogingival or distolingual groove should be considered (8). In the present study, fusion or gemination was less likely to occur because it resulted in a single larger crown or two crowns or roots fused together (7,8), while the tooth crown had normal dimensions in this case and radiography before work showed no evidence of invagination of dentin or enamel; therefore, dens in dent or dens invaginatus was also an improbable factor. In this regard, Sabala et al (9) reported that variations occurred in less than 1% of cases are unilateral in 90% of cases and most cases of the lateral incisor with two roots are also unilateral. Therefore, a possible etiology for unilateral accessory root may be caused by the traumatic injuries to the deciduous tooth, especially intrusive injuries (10). It should be noted that cone beam computed tomography (CBCT) is a diagnostic tool for evaluating teeth with an extra canal or root (11). When two roots or two canals are present superimposing each other buccolingually and are not well detected on conventional radiographs, CBCT can be useful. However, the initial radiography completely showed two roots in the present case report because the roots were mesial and distal. Indeed, surgical loupesand microscopes can be useful when there is difficulty to find canals or when the canals are in the depth of the pulp chamber. In our case, after access cavity preparation, two orifices were present in the mesial and distal roots; therefore it was not necessary to use this tool. However, the clinicians should be aware that even routine cases may sometimes have completely abnormal anatomy. Therefore, the lack of knowledge of anatomical variations can lead to failure in endodontic treatment due to inadequate cleaning, residual debris, and irritants in the missed canal.
Conclusions
Due to the wide morphological variations in the root and the root canal system of the teeth, clinicians should have knowledge of any anatomical variation to minimize the risk of endodontic treatment failure following inadequate debridement of indistinguishable or inaccessible portions of the root canal system. Hence, for managing cases with anatomical variation, modern diagnostic tools, recent endodontic techniques, and advancements in biomaterials to achieve high levels of success in endodontic treatment can be beneficial.
Conflict of Interest Disclosures
The authors declare that they have no conflict of interests.
Ethical Statement
Informed consent was obtained from the patient for being included in this study.
Authors’ Contribution
Study concept and design: HK and FM; Analysis and interpretation of data: FM and RS; Drafting of the manuscript: RS; Critical revision of the manuscript for important intellectual content: FM, RS, and LG; Statistical analysis: LG.
References
- Sponchiado EC Jr, Ismail HA, Braga MR, de Carvalho FK, Simões CA. Maxillary central incisor with two root canals: a case report. J Endod 2006; 32(10):1002-4. doi: 10.1016/j.joen.2006.03.022 [Crossref] [ Google Scholar]
- Yadav S, Shah N. Nonsurgical endodontic management of a two-rooted maxillary lateral incisor. Saudi Endod J 2016; 6(1):40-2. doi: 10.4103/1658-5984.172001 [Crossref] [ Google Scholar]
- Ravindranath M, Neelakantan P, Subba Rao CV. Maxillary lateral incisor with two roots: a case report. Gen Dent 2011; 59(1):68-9. [ Google Scholar]
- Slowey RR. Radiographic aids in the detection of extra root canals. Oral Surg Oral Med Oral Pathol 1974; 37(5):762-72. doi: 10.1016/0030-4220(74)90142-x [Crossref] [ Google Scholar]
- Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 1984; 58(5):589-99. doi: 10.1016/0030-4220(84)90085-9 [Crossref] [ Google Scholar]
- de Deus QD. Endodontia. 5th ed. Rio de Janeiro: MEDSI Editora Médica e Científica Ltda; 1992.
- Patil AA, Patil SA, Dodwad PK. Endodontic management of a supernumerary tooth fused to the maxillary permanent lateral Incisor. Saudi Endod J 2014; 4(1):28-31. doi: 10.4103/1658-5984.127984 [Crossref] [ Google Scholar]
- Hatton JF, Ferrillo PJ Jr. Successful treatment of a two-canaled maxillary lateral incisor. J Endod 1989; 15(5):216-8. doi: 10.1016/s0099-2399(89)80239-0 [Crossref] [ Google Scholar]
- Sabala CL, Benenati FW, Neas BR. Bilateral root or root canal aberrations in a dental school patient population. J Endod 1994; 20(1):38-42. doi: 10.1016/s0099-2399(06)80025-7 [Crossref] [ Google Scholar]
- Maghsoudlou A, Jafarzadeh H, Forghani M. Endodontic treatment of a maxillary central incisor with two roots. J Contemp Dent Pract 2013; 14(2):345-7. doi: 10.5005/jp-journals-10024-1325 [Crossref] [ Google Scholar]
- Kottoor J, Murugesan R, Albuquerque DV. A maxillary lateral incisor with four root canals. Int Endod J 2012; 45(4):393-7. doi: 10.1111/j.1365-2591.2011.01984.x [Crossref] [ Google Scholar]