Avicenna J Dent Res. 17(1):51-61.
doi: 10.34172/ajdr.2189
Review Article
In Vivo Conditions in Bone Tissue Engineering: A Review Article
Mehdi Azizi Writing – original draft, 1, 2 
Mehdi Shahgolzari Validation, 3
Alireza Hoseini Madani Validation, 4
Morteza Alizadeh Writing – review & editing, 1, 2
Fateme Besharati Validation, 5
Maziar Malekzadeh Kebria Supervision, Writing – review & editing, 1, 2, *
Author information:
1Cancer Research Center, Institute of Cancer, Avicenna Health Research Institute, Hamadan University of Medical Sciences, Hamadan, Iran
2Department of Tissue Engineering and Regenerative Medicine, Faculty of Medicine, Hamadan University of Medical Sciences, Hamadan, Iran
3Dental Research Center, Avicenna Institute of Clinical Sciences, Avicenna Health Research Institute, Hamadan University of Medical Sciences Hamadan, Iran
4Department of Chemistry, School of Sciences, Mazandaran University, Babolsar, Iran
5Department of Dentistry, School of Dentistry, Rafsanjan University of Medical Science, Rafsanjan, Iran
Abstract
Background: Bone tissue engineering (BTE) aims to create functional bone substitutes that can repair or regenerate damaged bone tissues. Achieving this goal requires a deep understanding of the in vivo conditions under which natural bone develops, heals, and remodels. These conditions are considered complex and involve mechanical, biochemical, and cellular factors that govern bone formation and regeneration. This article aimed to discuss the key aspects of in vivo conditions essential for successful BTE, including mechanical forces, biochemical signaling, cellular interactions, vascularization, immune responses, and the role of bone remodeling.
Methods: This article aimed to discuss the key aspects of in vivo conditions essential for successful BTE, including mechanical forces, biochemical signaling, cellular interactions, vascularization, immune responses, and the role of bone remodeling.
Results: The obtained data revealed that understanding vascularization and immune responses is crucial for designing engineered bone constructs that can mimic native bone and function effectively in clinical applications.
Conclusion: Ultimately, the continued refinement of in vivo models and a deeper understanding of the tissue microenvironment are essential for the development of BTE therapies that are not only effective but also safe, sustainable, and capable of providing long-term functional outcomes for patients.
Keywords: Bone, Tissue engineering, In Vivo condition, Osteogenesis, Bone remodeling
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Azizi M, Shahgolzari M, Hoseini Madani A, Alizadeh M, Besharati F, Malekzadeh Kebria M. in vivo conditions in bone tissue engineering: a review article. Avicenna J Dent Res. 2025;17(1):51-61. doi:10.34172/ajdr.2189
Background
Bone tissue engineering (BTE) is a multidisciplinary field that focuses on developing biologically and mechanically functional bone substitutes to repair or regenerate damaged bones. Some essential aspects of BTE are understanding and replicating the in vivo conditions within a living organism under which bone formation, healing, and remodeling occur. These conditions are critical for designing effective scaffolds, biomaterials, and cellular therapies to promote bone regeneration. Bone is a highly dynamic and mechanically responsive tissue. In vivo, mechanical forces, such as compression, tension, and shear stress, influence osteogenesis (bone formation) and remodeling (1). A successful BTE approach must provide scaffolds or constructs that can bear mechanical loads similar to native bone, promoting cellular responses such as the differentiation of stem cells into osteoblasts (bone-forming cells). Bone tissue is rich in various biochemical factors that regulate cellular behavior, including growth factors (e.g., bone morphogenetic proteins [BMPs] or vascular endothelial growth factor [VEGF]), hormones (e.g., parathyroid hormone), and extracellular matrix (ECM) proteins (e.g., collagen or osteopontin). In vivo, these factors play a critical role in osteogenesis, angiogenesis (formation of new blood vessels), and the overall remodeling of bone (2). Mimicking these biochemical signals in engineered constructs is essential for successful bone regeneration. The in vivo bone environment supports a dynamic interplay between various cell types, including osteoblasts, osteoclasts (bone-resorbing cells), osteocytes (mature bone cells embedded in the matrix), chondrocytes (cartilage cells), and various stem or progenitor cells. These cells are involved in continuous processes of bone formation, remodeling, and repair (3). BTE aims to recapitulate these cellular interactions within biomimetic scaffolds, often incorporating stem cells, growth factors, or co-cultures to encourage proper bone tissue formation. Bone tissue, especially in interior regions, requires an effective blood supply for nutrient exchange, waste removal, and delivery of oxygen and signaling molecules (4). Without proper vascularization, engineered bone tissues can suffer from necrosis (cell death) and inadequate healing. In vivo, angiogenesis plays a crucial role in ensuring the viability of new bone tissues. Therefore, vascularization strategies, such as the incorporation of pro-angiogenic factors or endothelial cells into tissue-engineered bone constructs, are a critical area of focus in bone regeneration (5). The immune system exerts a key role in the body’s response to injury and tissue engineering implants. In vivo, the immune response to implanted materials or constructs can influence their success. Ideally, biomaterials used in BTE should exhibit biocompatibility, minimizing inflammation and foreign body responses while promoting tissue integration (6). Chronic inflammation or immune rejection can hinder the regeneration process and lead to graft failure. Bone tissue is continuously remodeled throughout life, and successful bone regeneration requires a long-term process of matrix deposition, mineralization, and structural adaptation. In vivo, bone repair follows a well-orchestrated sequence of events, including inflammation, soft callus formation, hard callus formation, and remodeling. The tissue-engineered bone must also undergo these phases to ensure functional integration with the host tissue over time (7).
In vivo conditions in BTE encompass a complex and interconnected array of mechanical, biochemical, cellular, and vascular factors that govern bone formation, healing, and remodeling (8). Understanding and simulating these in vivo conditions are essential for creating engineered bone substitutes that can effectively repair or replace damaged bones in patients. Advances in biomaterials, stem cell therapies, and tissue engineering technologies are progressively enabling more successful translation of in vitro studies to in vivo applications, bringing us closer to reliable and functional bone regeneration therapies (9).
Mechanical Stimuli and Their Role in Bone Regeneration
Mechanical stimuli play a fundamental role in the development, maintenance, and repair of bone tissues in vivo. In BTE, understanding how mechanical forces influence bone regeneration is essential for designing scaffolds, biomaterials, and therapeutic strategies that promote effective healing and integration of engineered bones (10). In this context, mechanical stimuli include the physical forces that act on bone tissue, such as compression, tension, shear stress, and torsion. These forces govern critical cellular and molecular responses that drive bone growth, remodeling, and adaptation to functional demands. Mechanotransduction is the process by which cells convert mechanical stimuli into biochemical signals that regulate cellular functions such as differentiation, proliferation, and matrix production. In vivo, bone cells, particularly osteoblasts (bone-forming cells), osteoclasts (bone-resorbing cells), and osteocytes (mature bone cells embedded in the matrix), are highly responsive to mechanical signals. Osteoblasts respond to mechanical stimuli by enhancing the deposition of new bone matrix. Mechanical loading can stimulate osteoblast differentiation and matrix production, which is critical for bone regeneration. Osteocytes are key mechanosensors embedded within the bone matrix. These cells detect mechanical loads through their dendritic processes that make contact with the surrounding bone matrix (11). In addition, they send signals to osteoblasts and osteoclasts to modulate bone formation and resorption, respectively. Further, osteoclasts respond to mechanical unloading by promoting bone resorption to adapt the bone structure and maintain homeostasis. Mechanotransduction pathways are mediated by various signaling molecules, including Ras homolog family member A, phosphatidylinositol 3-kinases/protein kinase B, and mitogen-activated protein kinase, and involve cytoskeletal rearrangement within the bone cells. Mechanical forces affect the activation of these pathways, ultimately influencing gene expression related to osteogenesis (bone formation) and osteoclastogenesis (bone resorption) (12).
Depending on the type of applied force, mechanical forces influence bone regeneration in several ways. In the context of BTE, scaffolds and biomaterials are frequently designed to mimic or generate these mechanical forces to stimulate bone healing. Compression is one of the most important forces affecting bone growth. It is particularly relevant in weight-bearing bones (e.g., femur or tibia) that experience compressive forces during activities such as walking or running. In vivo, compression stimulates osteoblast activity, promoting new bone formation. It also suppresses osteoclast activity to prevent excessive bone resorption (Figure 1) (13).
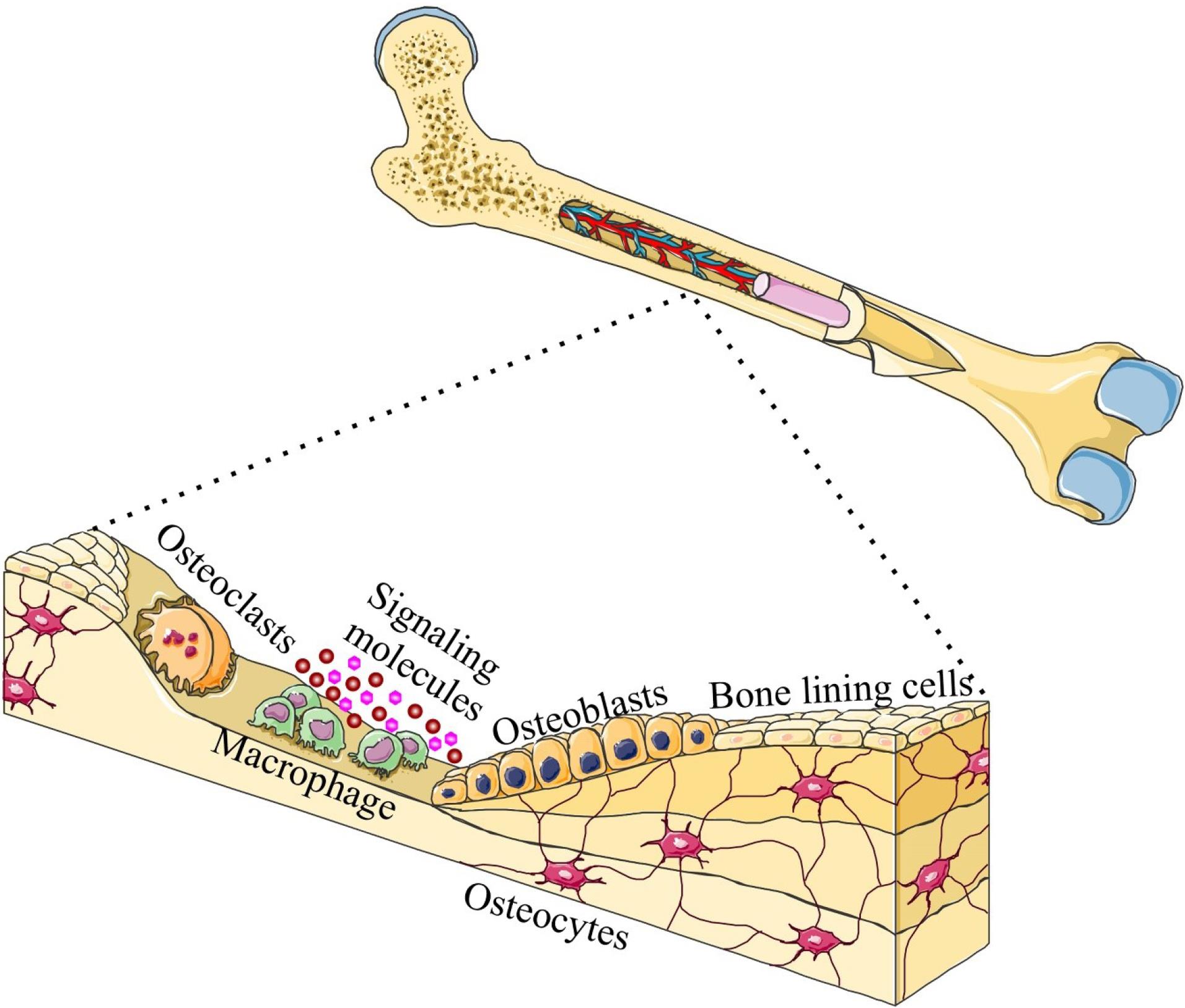
Figure 1.
Bone Repair by Cell Differentiation and Cell Signaling. Note. This process is involved in bone repair by mechanical stimulation
.
Bone Repair by Cell Differentiation and Cell Signaling. Note. This process is involved in bone repair by mechanical stimulation
Scaffolds used in BTE are often designed to mimic the compressive forces that naturally occur in bones. For example, polymeric scaffolds reinforced with materials such as hydroxyapatite (HA) or bioactive glasses are commonly engineered to withstand compressive loads and support osteogenesis (14). Another mechanical condition is tension, which refers to the elongation or stretching of the bone matrix. While bone is not as heavily loaded in tension as in compression, tensile forces can still significantly influence bone remodeling. Tensile forces generally stimulate bone formation in areas that are under tension and are responsible for the development of bone structures such as tendons and ligaments (14,15). These forces are thought to be involved in the alignment and organization of the bone matrix during growth and repair. Scaffolds designed for bone regeneration in tension-bearing areas, such as the tendon-bone interface, must be able to withstand tensile forces while also facilitating the osteogenic differentiation of stem cells. Materials with elastic properties and the ability to deform under load are key for mimicking tension-induced bone formation. Shear stress is generated when there is a force applied parallel to the surface of the bone, which is common in joint areas or areas subjected to complex loads. In addition, in in vivo effect, shear forces are crucial for the remodeling of bones, particularly in the early stages of fracture healing (16). They stimulate bone formation and resorption by affecting the osteoblast-osteoclast balance. Shear stress can also enhance angiogenesis (the formation of blood vessels), which is important for the survival of regenerating bone tissues. Scaffolds engineered in this condition mimic shear stress, which can improve the integration of the bone substitute into the surrounding tissue, especially in joint replacements and fracture healing. This can be achieved through micro-porous scaffolds or biomaterials that provide the appropriate surface topography to facilitate cell attachment and promote shear-induced signaling (17). Torsional forces (twisting forces) are typically encountered in long bones and rotational activities. Torsional forces stimulate bone remodeling and adaptation by enhancing the load-bearing capacity of bone structures. These forces are crucial for maintaining bone strength in areas subjected to rotational stress. BTE approaches often focus on creating scaffolds that can withstand torsional forces, especially in long bone fractures or spinal implants. Scaffolds with torsional stiffness and composite materials can help improve mechanical performance and promote bone integration (18).
Mechanical stimuli play an indispensable role in the process of bone regeneration, influencing cellular behavior, bone formation, and remodeling. In vivo, bone cells dynamically respond to compressive, tensile, shear, and torsional forces, which are critical for maintaining bone integrity and facilitating fracture healing. In BTE, replicating these mechanical environments is essential for designing scaffolds and biomaterials that can successfully support bone regeneration (19). By integrating mechanical loading into engineered bone constructs, researchers can enhance osteogenesis, promote tissue integration, and improve the clinical outcomes of bone repair and replacement therapies. The ongoing development of advanced biomechanical scaffolds that can mimic in vivo mechanical stimuli is a promising direction in BTE, bringing us closer to more effective, durable, and functional bone regenerative therapies (Table 1) (20).
Table 1.
In Vivo Conditions in Bone Tissue Engineering
|
In Vivo
Conditions
|
Description
|
Relevance to Bone Tissue Engineering
|
| Mechanical load/stress |
The presence of dynamic mechanical forces such as compression, tension, and shear. |
Mechanical stimuli are essential for bone development, remodeling, and healing. Scaffolds and engineered tissues must withstand physiological loads (7). |
| Oxygen tension |
Oxygen availability varies in different regions of bone tissue, with hypoxic environments near bone marrow. |
Oxygen plays a key role in cell metabolism, differentiation, and angiogenesis. Scaffolds should support oxygen gradients (21). |
| pH levels |
The bone environment typically has a slightly alkaline pH (7.2-7.4). However, it can drop in disease or injury. |
Scaffold materials should maintain pH stability to avoid disrupting cell function (22). |
| Cellular environment |
It includes osteoblasts, osteoclasts, mesenchymal stem cells, and other bone-resident cells. |
The interaction between scaffolds and resident cells (osteocytes or osteoblasts) is critical for tissue regeneration (9). |
| Growth factors and cytokines |
They include bone morphogenetic proteins, vascular endothelial growth factor, and the like. |
These molecules stimulate cell proliferation, differentiation, and angiogenesis. Scaffolds can be designed to release these factors in a controlled manner (10). |
| Bone matrix composition |
It is primarily made of collagen type I, hydroxyapatite, and other non-collagenous proteins. |
Mimicking the extracellular matrix composition is essential for osteogenic differentiation and mineralization (23). |
| Vascularization |
Development of new blood vessels (angiogenesis) is required for nutrient supply and waste removal. |
Scaffolds should encourage vascular growth to sustain tissue survival and regeneration (11). |
| Inflammation |
Inflammatory responses after bone injury or surgery involve the activation of immune cells. |
Chronic inflammation can impair healing. Biomaterials should ideally modulate the inflammatory response to promote healing without excessive immune activation (12). |
| Bone remodeling |
The ongoing process of bone resorption and deposition is regulated by osteoclasts and osteoblasts. |
Bone tissue engineering must support the continuous remodeling of newly formed bone to integrate with the host tissue (16). |
| Immune response |
The host immune system must not reject engineered tissues, while inflammation must be controlled. |
The biocompatibility of scaffolds and materials is essential to prevent immune rejection or excessive inflammation (18). |
| Temperature |
Normal bone temperature is around 37°C in humans, but it may fluctuate in response to injury or disease. |
Biomaterials and cell-based therapies should maintain functionality under in vivo temperature conditions (19). |
| Nutrient and waste exchange |
Bone tissue relies on efficient nutrient and waste exchange, especially in deeper regions. |
Scaffolds need to allow the diffusion of nutrients and removal of waste products, especially in large tissue-engineered constructs (19,20). |
| Age-related factors |
Aging can affect bone density, mineralization, and the activity of osteoblasts and osteoclasts. |
Age-related conditions (e.g., osteoporosis) should be considered when designing therapies for older populations (24). |
| Infection risk |
Bone tissue is susceptible to infection after surgery or injury, particularly in open fractures. |
Infection resistance or antibacterial properties in scaffolds are crucial for successful bone regeneration (25). |
Biochemical Environment and Molecular Signaling
BTE seeks to develop strategies for regenerating bone tissues to repair skeletal defects or injuries. This complex process requires not only scaffold materials and cell types but also a proper biochemical environment and molecular signaling to effectively promote bone formation in vivo. The biochemical environment and molecular signaling pathways are crucial for successful bone tissue regeneration. They influence stem cell differentiation, ECM mineralization, and engineered tissue integration into the host bone (26). The biochemical environment includes factors such as growth factors, cytokines, and ECM components that regulate cell behavior and bone formation. Several vital elements are BMPs, VEGF, and transforming growth factor beta (TGF-β). Growth factors are signaling proteins that regulate cellular processes such as proliferation, differentiation, and migration. BMPs, particularly BMP-2, BMP-7, and BMP-4, are critical for osteogenesis (bone formation) and the induction of mesenchymal stem cell (MSC) differentiation into osteoblasts. They are frequently used in BTE to promote bone regeneration (25). VEGF is essential for angiogenesis (the formation of blood vessels), which is necessary for supplying nutrients and oxygen to the developing bone tissue. The engineered tissue cannot survive and mature without proper vascularization. TGF-β regulates both osteogenesis and chondrogenesis (cartilage formation). It plays an essential role in maintaining the balance between osteoblast and osteoclast activities and modulating the ECM composition. The ECM provides structural and biochemical support to cells and is composed of various proteins, glycoproteins, and polysaccharides. It is not only essential for cell anchorage and mechanical strength but also provides bioactive cues for cellular differentiation and tissue development (27).
Osteogenesis and regeneration are highly regulated by a network of molecular signaling pathways. These pathways control stem cell differentiation, matrix deposition, mineralization, and vascularization. The Wnt/β-catenin pathway is crucial for regulating osteoblast differentiation and bone formation. In response to Wnt ligands, the β-catenin protein accumulates in the cytoplasm and translocates to the nucleus, where it activates the transcription of target genes that promote osteogenesis. This pathway also regulates the balance between osteoblast and osteoclast activity. Notch signaling is involved in regulating cell fate determination, differentiation, and tissue patterning during bone development. In BTE, Notch signaling influences MSC differentiation into osteoblasts and regulates the development of the bone marrow niche (28).
This pathway plays a vital role in bone remodeling. The receptor activator of nuclear factor κB ligand (RANKL) promotes osteoclast differentiation, while its decoy receptor, osteoprotegerin, inhibits osteoclastogenesis by binding to RANKL. The balance between RANKL and osteoprotegerin determines bone resorption and formation. In tissue engineering, controlling this pathway is important for preventing excessive resorption and promoting bone regeneration. Hedgehog signaling is involved in early skeletal patterning and bone growth regulation. It influences the differentiation of chondrocytes and osteoblasts and is essential for the formation of bone structures during embryogenesis and postnatal bone regeneration. The mitogen-activated protein kinase pathway, specifically the extracellular signal-regulated kinase pathway, regulates osteoblast differentiation, matrix production, and mineralization. It also responds to mechanical loading and extracellular stimuli that are important for the adaptive response of bone tissues (29). The phosphatidylinositol 3-kinases/protein kinase B signaling pathway regulates cell survival, proliferation, and metabolism. In BTE, it promotes osteoblast differentiation and bone formation by activating downstream targets such as the mechanistic target of rapamycin, which controls cell growth and protein synthesis. Parathyroid hormone-related peptide (PTHrP) and PTH regulate bone remodeling by influencing osteoblast and osteoclast activity (29,30). PTH and PTHrP stimulate the production of RANKL, thereby promoting osteoclastogenesis and bone resorption. Scaffolds should mimic the mechanical properties of bones, facilitate cell attachment, and provide a supportive microenvironment for growth factor delivery. Biodegradable materials such as collagen, poly(lactic-co-glycolic acid) (PLGA), or HA are commonly used, and they may be combined with bioactive molecules to enhance osteogenesis. In vivo BTE requires the establishment of vascular networks to supply oxygen and nutrients. This can be achieved through using pro-angiogenic factors such as VEGF or by incorporating vascular endothelial cells into scaffolds. The immune response can significantly impact the success of BTE. Inflammation and immune rejection may interfere with tissue integration and regeneration. Using biomaterials with anti-inflammatory properties or immunomodulatory agents may help improve the success of bone regeneration in vivo (31).
In vivo BTE relies on a highly regulated biochemical environment and complex molecular signaling pathways to promote the regeneration of functional bone tissues. Growth factors, ECM components, and signaling pathways such as Wnt/β-catenin, BMP, and VEGF are central to the process of osteogenesis and tissue integration. Understanding and manipulating these factors can improve the effectiveness of BTE strategies, leading to better clinical outcomes in bone regeneration and repair (31,32).
Cellular Interactions and the Role of Stem Cells
BTE is a rapidly advancing field that seeks to develop functional bone replacements for repairing bone defects due to trauma, disease, or congenital disorders. The process of engineering bone tissue in vivo involves not only biomaterials and scaffolds but also the intricate cellular interactions that are essential for the regeneration of functional bone tissues. Stem cells play a pivotal role in this process, driving bone repair and regeneration by differentiating into osteogenic cells and interacting with the surrounding microenvironment. Stem cells are undifferentiated cells capable of self-renewal and differentiation into multiple cell types, including osteoblasts and bone-forming cells. Several types of stem cells are used in BTE. MSCs are adult stem cells found in various tissues such as bone marrow, adipose tissue, and umbilical cord blood. MSCs are multipotent and have the potential to differentiate into osteoblasts under appropriate conditions. Induced pluripotent stem cells are somatic cells reprogrammed to an embryonic-like state and can be differentiated into any cell type, including osteogenic lineages. Embryonic stem cells, as pluripotent stem cells, are derived from embryos, which can also differentiate into osteoblasts, though their use in clinical settings is limited due to ethical and regulatory concerns (33,34).
In vivo, bone tissue regeneration occurs in a complex microenvironment composed of various cell types such as osteoblasts, osteoclasts (bone-resorbing cells), endothelial cells (blood vessel-forming cells), and immune cells. These cells interact with each other through soluble factors, cell-cell contact, and ECM molecules to support bone formation. MSCs can differentiate into osteoblasts in response to signals such as BMPs, TGF-β, and mechanical stimuli. In vivo, stem cells interact with ECM proteins such as collagen type I, osteopontin, and fibronectin, leading to osteogenesis promotion. Bone regeneration requires the formation of new blood vessels (angiogenesis) to supply oxygen and nutrients to the growing tissue. Stem cells interact with endothelial cells to promote angiogenesis, which is essential for the survival of the newly formed bone tissue. Inflammatory responses play a critical role in tissue regeneration, but chronic inflammation can impair healing. MSCs have immunomodulatory properties and can suppress excessive inflammation, ensuring a balance between tissue repair and immune response (35,36).
MSCs, when seeded into scaffolds and implanted into bone defects, undergo osteogenic differentiation in response to signals from the local microenvironment. This results in the formation of bone matrix and mineralization, which are critical steps in bone regeneration. The tissue must be vascularized for successful bone regeneration. Stem cells interact with endothelial cells to promote the formation of blood vessels, which supply oxygen and nutrients to the newly formed bone tissue (Table 2) (37). This is a crucial aspect of in vivo bone regeneration. MSCs have the ability to modulate the immune response, potentially reducing the risk of inflammation and rejection in tissue engineering applications. This immunosuppressive function allows for better integration of implanted cells and scaffolds. The engineered bone tissue needs to integrate with the surrounding native bone tissue. Mechanical properties, such as stiffness and porosity, influence how well the scaffold integrates and supports stem cell differentiation into bone tissue. Finally, it must be mentioned that in vivo BTE involves a complex interplay of stem cells, scaffolds, growth factors, and the surrounding cellular microenvironment. Stem cells are key players in the regeneration of bone tissues by differentiating into osteogenic lineages and interacting with other cells to promote angiogenesis, immune modulation, and tissue integration. Continued research into improving stem cell-based therapies, scaffold designs, and in vivo models will likely yield more effective treatments for bone regeneration and repair (38).
Table 2.
The Key Aspects of Cellular Interactions and the Role of Stem Cells in Bone Tissue Engineering In Vivo
|
Aspect
|
Description
|
Key Cell Types Involved
|
Key Factors and Mechanisms
|
| Stem cells in bone regeneration |
Stem cells are pivotal for osteogenesis, capable of differentiating into osteoblasts, chondrocytes, or adipocytes, depending on the signals in their microenvironment. They form the basis of engineered bone tissue. |
- MSCs
- Adipose-derived stem cells
- Induced pluripotent stem cells
- Perivascular stem cells |
Growth factors: BMPs, TGF-β, fibroblast growth factor
- Cell adhesion molecules: Integrins, cadherins (28). |
| Osteogenesis (bone formation) |
Stem cells differentiate into osteoblasts under appropriate biochemical and mechanical cues. Osteoblasts secrete ECM proteins that form the bone matrix and later become osteocytes. |
- Osteoblasts
- Osteocytes |
BMPs: Stimulate osteogenesis
- Mechanical loading: Influencing differentiation via mechanotransduction
- ECM (Collagen): Providing structural scaffolds for osteoblast function and mineralization (39). |
| ECM interactions |
The ECM provides structural and biochemical support for stem cells. The composition of the ECM influences stem cell behavior, such as differentiation, migration, and proliferation. |
- Fibroblasts
- MSCs
- Osteoblasts |
Collagen type I: Major ECM protein in bones
- Integrins: Cell-surface receptors that mediate cell
- ECM interactions
- Hyaluronic acid and fibronectin: Supporting cell adhesion and migration (40). |
| Mechanical stimulation |
Mechanical forces, such as compression, tension, and shear, influence stem cell differentiation by triggering mechanotransduction pathways that affect gene expression related to osteogenesis. Stem cells can respond to mechanical cues via mechanotransduction, influencing osteogenic differentiation. |
- MSCs
- Osteoblasts
- Osteocytes |
Biomechanical forces: Compression and shear stress influence stem cell differentiation into osteoblasts
- Mechanosensitive channels: Piezo1 and TRPV4 mediate mechanical signal transduction to alter gene expression (41). |
| Chondrogenesis and endochondral ossification |
In large bone defects, stem cells may differentiate into chondrocytes, forming a cartilage template that is later replaced by bone. This process (endochondral ossification) is essential for the formation of long bones and the healing of critical-size defects. |
- Chondrocytes
- MSCs |
Cartilage matrix: Aggrecan, type II collagen
- BMP-2, TGF-β: Stimulating chondrogenesis
- Hypoxic conditions: Promoting chondrocyte differentiation
- Endochondral ossification: Cartilage is replaced by bone during healing (42). |
Abbreviations: ECM, extracellular matrix; MSCs, mesenchymal stem cells; BMPs, bone morphogenetic proteins; TGF-β, transforming growth factor beta.
Vascularization: Ensuring Nutrient and Oxygen Supply
Vascularization is one of the key challenges in BTE, particularly when creating bone substitutes that are intended to integrate with native bone tissues. The process ensures that the engineered tissue can receive a continuous supply of nutrients and oxygen, which are essential for cellular survival, proliferation, and differentiation. Without sufficient vascularization, the inner regions of a bone scaffold can become hypoxic, leading to necrosis, poor healing, and eventual failure of the tissue construct (43).
Bone is a highly vascularized tissue, and its health depends on a rich network of blood vessels that supply it with oxygen and nutrients and remove metabolic waste. As bone tissue is complex and relatively large, scaffolds for bone regeneration must also support vascular networks to sustain cellular activities deep within the structure (44). Oxygen and nutrient delivery to cells at the center of the scaffold can become inadequate, leading to tissue necrosis and failure of new bone formation. Inadequate vascularization in the engineered bone can delay or prevent bone regeneration, as angiogenesis is crucial for bone remodeling and repair. Poor vascular supply can lead to a higher risk of infection and inflammatory responses. Various strategies have been developed to encourage the formation of a functional vascular network within BTE. Creating scaffolds with a well-defined, interconnected pore structure that mimics the natural architecture of bones, is one of the strategies. These pores serve as channels through which endothelial cells can migrate and form blood vessels. Scaffolds made from biodegradable polymers (e.g., PLGA, polylactide, or collagen) or natural materials (e.g., gelatin or HA) can degrade over time, allowing space for blood vessel growth and integration with the host tissue (45). Materials can be engineered to mimic the native bone environment or designed to release growth factors, such as VEGF and fibroblast growth factor, to actively promote angiogenesis and the formation of blood vessels within the scaffold. Many growth factors contribute to angiogenesis in BTE. VEGF is one of the most important pro-angiogenic factors. By incorporating VEGF into scaffolds or using gene delivery systems, researchers can enhance endothelial cell proliferation and capillary formation. Fibroblast growth factor also promotes angiogenesis by stimulating endothelial cell migration and proliferation. BMPs, particularly BMP-2 and BMP-7, play a role in bone formation and vascularization. Using hydrogels or microspheres to release growth factors in a controlled manner over time can provide a sustained pro-angiogenic effect. Animal models (e.g., mouse, rat, and rabbit models) are commonly used to study BTE and vascularization. These models allow researchers to monitor the integration of engineered bone tissues with the host’s vasculature and assess the functional outcomes. In human applications, vascularization is essential for bone grafts, particularly in the context of large bone defects, critical-sized bone defects, or non-unions. Engineering bone tissues with adequate vascular support can improve the success rates of bone implants and prosthetics (46).
Thus, vascularization is a critical factor for the success of in vivo BTE. Without an adequate blood supply, engineered bone constructs cannot survive, integrate, or function properly. Through innovative approaches in biomaterial design, growth factor delivery, and prevascularization techniques, researchers are making significant strides in developing vascularized bone tissues for clinical applications. However, challenges remain in ensuring long-term and sustainable vascular networks, particularly in large-scale bone regeneration. The continued development of these strategies promises to improve outcomes in bone healing, bone replacement, and regenerative medicine. Scaffolds with interconnected pore structures mimic the natural architecture of bone, providing physical space for endothelial cells to migrate into the scaffold and form a functional vascular network. The pore size and connectivity are key factors in ensuring efficient vascularization (47).
Immune Response and Biocompatibility
In vivo BTE aims to repair or replace damaged bone tissues using biomaterials, cells, and growth factors. A successful BTE approach requires not only the development of biomaterials that can mimic the natural bone structure and function but also the consideration of the immune response and biocompatibility of these materials within the biological environment. The immune system plays a critical role in the success or failure of biomaterial implants and tissue regeneration strategies (48). When a biomaterial is introduced into the body, it interacts with the host immune system, which may respond in several ways depending on the material, its degradation products, and the surrounding microenvironment. Two main types of immune responses can influence the outcome of BTE (49). The acute immune response occurs immediately after implantation and involves the activation of the innate immune system. The biomaterial triggers the release of pro-inflammatory cytokines and the recruitment of immune cells such as neutrophils and macrophages. This response typically aims at recognizing and eliminating foreign materials. Macrophages play a pivotal role in the immune response. Initially, they are activated to a pro-inflammatory (M1) phenotype, which promotes tissue destruction and fibrosis. However, in tissue regeneration, macrophages must polarize toward an anti-inflammatory (M2) phenotype, which promotes tissue healing and remodeling. The foreign body reaction is a chronic inflammation that can occur if the material is perceived as foreign by the immune system. It can lead to fibrosis, encapsulation, and failure of the implanted material to integrate with the surrounding tissue. In the chronic immune response, the biomaterial cannot be effectively integrated or resorbed by the body (50). The immune system can mount a chronic inflammatory response. If a biomaterial is not biodegradable, it may become surrounded by a layer of immune cells, forming a granuloma, which can interfere with tissue regeneration. The outcome of the immune response depends on several factors, including the material’s surface properties, degradation rate, and interactions with the surrounding cells (51). For successful bone regeneration, controlling the immune response is critical to preventing chronic inflammation and ensuring effective healing. Biocompatibility refers to the ability of a material to perform its intended function without eliciting harmful effects on the surrounding tissues. The composition of the biomaterial plays a key role in its interaction with biological tissues and cells. Biomaterials used in BTE must have osteoconductivity, osteoinductivity, and osteointegration. Osteoconductivity is the ability to support the attachment, proliferation, and differentiation of bone cells (osteoblasts) and promote the formation of new bone tissues. The ability to stimulate stem cells or progenitor cells to differentiate into bone-forming cells in the presence of appropriate growth factors is called osteoinductive (52). In addition, tom osteointegration is the ability of the biomaterial to integrate with the surrounding bone tissue without inducing a foreign body reaction. This is essential for long-term success. Materials such as HA, tricalcium phosphate, and bioactive glass are commonly utilized in BTE due to their similarity to natural bone minerals and their ability to support osteogenesis. More recently, composite biomaterials that combine these materials with polymers or other biocompatible substances have been developed to enhance mechanical properties and degradation rates. BTE often involves the use of biodegradable materials that gradually degrade and resorb over time as the new bone tissue forms. The degradation rate must match the rate of bone regeneration. The material may not provide sufficient support during the critical early stages of healing if it degrades too quickly. Conversely, it may elicit a foreign body response if it degrades too slowly. The by-products of degradation must also be non-toxic and non-inflammatory to prevent complications. For example, materials such as PLGA and polycaprolactone are commonly used for bone regeneration due to their adjustable degradation rates and biocompatibility (53,54).
The success of in vivo BTE is highly dependent on the interaction between the immune system, the biomaterials, and the surrounding tissues. A well-designed biomaterial should be biocompatible, promoting osteogenesis while minimizing adverse immune reactions. Advances in material science, immune modulation, and cell-based therapies hold the potential to improve the outcomes of BTE, offering promising strategies for the repair of complex bone defects and injuries (55).
Bone Remodeling and Long-term Integration
BTE seeks to create functional bone substitutes that can integrate with the host tissue to restore or replace damaged bones. This process involves a combination of biomaterials, cells, and bioactive factors designed to promote bone regeneration and remodeling. The long-term success of BTE depends on the ability of the engineered construct to undergo proper bone remodeling and integrate with the host tissue in vivo (56).
Osteoclast activity subsides and resorption sites are cleared in the reversal phase. This phase also facilitates the recruitment of osteoblasts to begin the deposition of a new bone matrix, effectively bridging the gap between resorption and bone formation. Bone remodeling is a dynamic and continuous process that involves the coordinated action of osteoclasts (bone-resorbing cells), osteoblasts (bone-forming cells), and osteocytes (bone-embedded cells that regulate remodeling). This process is essential for maintaining bone homeostasis, repairing microdamages, and adapting bone structure to mechanical loading. Bone remodeling in vivo can be divided into four major phases. In the activation phase, the recruitment and activation of osteoclasts resorb bone at the site of the injury or implant. In the resorption phase, osteoclasts break down the bone matrix, creating a resorption pit. In the reversal phase (bone resorption), the resorption sites are cleared, and osteoblasts are recruited to begin the deposition of the new bone matrix. At the end of the process, osteoblasts secrete osteoid (the unmineralized bone matrix), which is then mineralized to form a new bone (57).
Long-term integration refers to the process by which the engineered bone tissue becomes indistinguishable from the host bone over time, with full vascularization, innervation, and functional mechanical properties. Several factors influence this integration process. The scaffold must mimic the mechanical and biological properties of the natural bone. It should be osteoconductive (supporting bone cell attachment and growth), osteoinductive (stimulating new bone formation), and biodegradable (gradually resorbing to be replaced by the new bone). The scaffold’s porosity, surface roughness, and degradation rate are crucial to the remodeling process. Osteoprogenitor cells (e.g., MSCs or induced pluripotent stem cells) seeded into the scaffold can enhance bone formation by differentiating into osteoblasts (58). Additionally, osteoclasts are critical for bone remodeling, as they resorb the engineered material during the early stages of healing. Vascularization is crucial for the long-term survival of the bone graft, as it provides nutrients and oxygen to the tissue and removes waste products. Engineering vascular networks or promoting angiogenesis in the graft can significantly enhance integration. Failure to form blood vessels can lead to necrosis and failure of the graft (59). Further, bone is a mechanosensitive tissue, and loading can stimulate bone formation. Functional mechanical loads can promote osteoblast activity and the mineralization of a newly formed bone. Properly designed BTE constructs must be able to withstand these loads during the remodeling process without compromising their integrity (60). A prolonged inflammatory response can impede the healing process, leading to fibrosis or the formation of scar tissue instead of functional bone. The immune response must be carefully modulated to ensure that the body accepts the implant while still effectively responding to infection and injury. A prolonged inflammatory response can impede healing by causing fibrosis or scar tissue formation instead of the functional bone. Therefore, careful modulation of the immune response is essential, as it allows for effective tissue healing while minimizing the risk of chronic inflammation that could interfere with the graft’s integration into the host bone. Several strategies have been developed to improve the long-term integration and success of BTE in in vivo conditions. The addition of growth factors such as BMPs, VEGF, and platelet-derived growth factors can enhance osteogenesis and angiogenesis, promoting better integration with the host bone. Advances in material science have led to the development of advanced scaffolds made from natural polymers (e.g., collagen or hyaluronic acid), synthetic polymers (e.g., PLGA), or composite materials (e.g., calcium phosphate or HA). These materials can be engineered to release bioactive molecules in a controlled manner to stimulate tissue growth and remodeling. Engineering vascular networks or co-culturing osteoblasts and endothelial cells (which form blood vessels) in the scaffold can help the tissue integrate more rapidly by providing an early blood supply. Three-dimensional printing technologies allow for the fabrication of scaffolds with complex geometries and microstructures that mimic the natural bone structure. This can improve cell migration, vascularization, and mechanical properties of the graft. Using bioreactors to provide mechanical stimulation (e.g., shear stress or compression) can enhance bone formation and remodeling by mimicking the mechanical forces experienced by bone in vivo (33).
Animal models (e.g., rodents, rabbits, pigs, and non-human primates) are commonly used to study BTE and long-term integration. These models allow researchers to assess the biological and mechanical performance of engineered bone grafts under conditions that closely mimic the human body. Critical parameters such as bone healing time, vascularization, bone mineral density, and mechanical strength are evaluated during the healing process (61).
While promising in preclinical studies, the clinical translation of BTE faces several challenges. The variability in patient-specific factors, such as age, underlying health conditions, and mechanical demands, complicates the ability to predict the long-term success of engineered bone grafts. Moreover, the high cost and complexity of manufacturing cell- or biomaterial-based therapies represent significant barriers to widespread adoption in clinical practice. Nonetheless, advances in tissue engineering, biomaterials, and stem cell biology hold promise for the development of more effective and reliable strategies to regenerate bone tissues, particularly for conditions such as critical-sized bone defects, osteoporosis, and bone cancers (45). The long-term success of BTE depends on the ability of engineered constructs to undergo appropriate bone remodeling and integrate with the host tissue in vivo. Achieving this goal requires a deep understanding of the complex biological processes involved in bone regeneration and the development of materials and techniques that can mimic these processes. By enhancing the vascularization, mechanical properties, and biological signals within the engineered construct and using advanced preclinical models, it is possible to develop functional bone substitutes that can be successfully integrated into the body for the repair of bone defects (62).
Conclusion
In vivo conditions play a pivotal role in the success of BTE, as they provide a complex and dynamic environment that mimics the biological processes essential for bone regeneration. The ability to recreate the mechanical, biochemical, and cellular characteristics of the natural bone tissue within a living organism is crucial for the development of effective bone substitutes. While in vitro studies offer valuable insights, in vivo models provide a more accurate representation of how engineered constructs interact with surrounding tissues, vascular networks, and immune responses. BTE strategies must account for several in vivo factors, including scaffold integration, osteointegration, growth factor release, vascularization, and the regulation of cell differentiation. Furthermore, challenges posed by immune rejection, inflammatory responses, and the optimization of mechanical properties need to be carefully addressed to ensure the longevity and functionality of the engineered bone tissue. Advancements in biomaterials, gene therapy, and stem cell technology are significantly improving the prospects of in vivo bone regeneration, bringing us closer to clinically viable solutions for bone defects and disorders. Eventually, the continued refinement of in vivo models and a deeper understanding of the tissue microenvironment are necessary for developing BTE therapies that are effective, sustainable, and safe and can provide long-term functional outcomes for patients.
Acknowledgements
The authors would like to thank the tissue engineering group of Hamadan University of Medical Sciences for supporting this study.
Competing Interests
There is no conflict of interests or personal relationship among the authors that is known to have influenced or caused a conflict of interests in this work.
Ethical Approval
The ethical issues have been fully addressed in this review.
Funding
There is no funding for this study.
References
- Tsiklin IL, Shabunin AV, Kolsanov AV, Volova LT. In vivo bone tissue engineering strategies: advances and prospects. Polymers (Basel) 2022; 14(15):3222. doi: 10.3390/polym14153222 [Crossref] [ Google Scholar]
- Shin M, Yoshimoto H, Vacanti JP. In vivo bone tissue engineering using mesenchymal stem cells on a novel electrospun nanofibrous scaffold. Tissue Eng 2004; 10(1-2):33-41. doi: 10.1089/107632704322791673 [Crossref] [ Google Scholar]
- Jiang T, Nukavarapu SP, Deng M, Jabbarzadeh E, Kofron MD, Doty SB. Chitosan-poly(lactide-co-glycolide) microsphere-based scaffolds for bone tissue engineering: in vitro degradation and in vivo bone regeneration studies. Acta Biomater 2010; 6(9):3457-70. doi: 10.1016/j.actbio.2010.03.023 [Crossref] [ Google Scholar]
- van Gaalen SM, Kruyt MC, Geuze RE, de Bruijn JD, Alblas J, Dhert WJ. Use of fluorochrome labels in in vivo bone tissue engineering research. Tissue Eng Part B Rev 2010; 16(2):209-17. doi: 10.1089/ten.TEB.2009.0503 [Crossref] [ Google Scholar]
- Leyendecker Junior A, Gomes Pinheiro CC, Lazzaretti Fernandes T, Franco Bueno D. The use of human dental pulp stem cells for in vivo bone tissue engineering: a systematic review. J Tissue Eng 2018; 9:2041731417752766. doi: 10.1177/2041731417752766 [Crossref] [ Google Scholar]
- Healy KE, Guldberg RE. Bone tissue engineering. J Musculoskelet Neuronal Interact 2007; 7(4):328-30. [ Google Scholar]
- Roseti L, Parisi V, Petretta M, Cavallo C, Desando G, Bartolotti I. Scaffolds for bone tissue engineering: state of the art and new perspectives. Mater Sci Eng C Mater Biol Appl 2017; 78:1246-62. doi: 10.1016/j.msec.2017.05.017 [Crossref] [ Google Scholar]
- Salgado AJ, Coutinho OP, Reis RL. Bone tissue engineering: state of the art and future trends. Macromol Biosci 2004; 4(8):743-65. doi: 10.1002/mabi.200400026 [Crossref] [ Google Scholar]
- Bose S, Roy M, Bandyopadhyay A. Recent advances in bone tissue engineering scaffolds. Trends Biotechnol 2012; 30(10):546-54. doi: 10.1016/j.tibtech.2012.07.005 [Crossref] [ Google Scholar]
- Wubneh A, Tsekoura EK, Ayranci C, Uludağ H. Current state of fabrication technologies and materials for bone tissue engineering. Acta Biomater 2018; 80:1-30. doi: 10.1016/j.actbio.2018.09.031 [Crossref] [ Google Scholar]
- Bose S, Vahabzadeh S, Bandyopadhyay A. Bone tissue engineering using 3D printing. Mater Today 2013; 16(12):496-504. doi: 10.1016/j.mattod.2013.11.017 [Crossref] [ Google Scholar]
- Kneser U, Schaefer DJ, Polykandriotis E, Horch RE. Tissue engineering of bone: the reconstructive surgeon’s point of view. J Cell Mol Med 2006; 10(1):7-19. doi: 10.1111/j.1582-4934.2006.tb00287.x [Crossref] [ Google Scholar]
- Amini AR, Laurencin CT, Nukavarapu SP. Bone tissue engineering: recent advances and challenges. Crit Rev Biomed Eng 2012; 40(5):363-408. doi: 10.1615/critrevbiomedeng.v40.i5.10 [Crossref] [ Google Scholar]
- Costa-Pinto AR, Reis RL, Neves NM. Scaffolds based bone tissue engineering: the role of chitosan. Tissue Eng Part B Rev 2011; 17(5):331-47. doi: 10.1089/ten.teb.2010.0704 [Crossref] [ Google Scholar]
- de Misquita MR, Bentini R, Goncalves F. The performance of bone tissue engineering scaffolds in in vivo animal models: a systematic review. J Biomater Appl 2016; 31(5):625-36. doi: 10.1177/0885328216656476 [Crossref] [ Google Scholar]
- Mauney JR, Jaquiéry C, Volloch V, Heberer M, Martin I, Kaplan DL. In vitro and in vivo evaluation of differentially demineralized cancellous bone scaffolds combined with human bone marrow stromal cells for tissue engineering. Biomaterials 2005; 26(16):3173-85. doi: 10.1016/j.biomaterials.2004.08.020 [Crossref] [ Google Scholar]
- Steffens L, Wenger A, Stark GB, Finkenzeller G. In vivo engineering of a human vasculature for bone tissue engineering applications. J Cell Mol Med 2009; 13(9B):3380-6. doi: 10.1111/j.1582-4934.2008.00418.x [Crossref] [ Google Scholar]
- O’Keefe RJ, Mao J. Bone tissue engineering and regeneration: from discovery to the clinic--an overview. Tissue Eng Part B Rev 2011; 17(6):389-92. doi: 10.1089/ten.TEB.2011.0475 [Crossref] [ Google Scholar]
- Siddappa R, Licht R, van Blitterswijk C, de Boer J. Donor variation and loss of multipotency during in vitro expansion of human mesenchymal stem cells for bone tissue engineering. J Orthop Res 2007; 25(8):1029-41. doi: 10.1002/jor.20402 [Crossref] [ Google Scholar]
- Collins MN, Ren G, Young K, Pina S, Reis RL, Oliveira JM. Scaffold fabrication technologies and structure/function properties in bone tissue engineering. Adv Funct Mater 2021; 31(21):2010609. doi: 10.1002/adfm.202010609 [Crossref] [ Google Scholar]
- Fragogeorgi EA, Rouchota M, Georgiou M, Velez M, Bouziotis P, Loudos G. In vivo imaging techniques for bone tissue engineering. J Tissue Eng 2019; 10:2041731419854586. doi: 10.1177/2041731419854586 [Crossref] [ Google Scholar]
- Karp JM, Sarraf F, Shoichet MS, Davies JE. Fibrin-filled scaffolds for bone-tissue engineering: an in vivo study. J Biomed Mater Res A 2004; 71(1):162-71. doi: 10.1002/jbm.a.30147 [Crossref] [ Google Scholar]
- Kempen DH, Lu L, Hefferan TE, Creemers LB, Maran A, Classic KL. Retention of in vitro and in vivo BMP-2 bioactivities in sustained delivery vehicles for bone tissue engineering. Biomaterials 2008; 29(22):3245-52. doi: 10.1016/j.biomaterials.2008.04.031 [Crossref] [ Google Scholar]
- Ghassemi T, Shahroodi A, Ebrahimzadeh MH, Mousavian A, Movaffagh J, Moradi A. Current concepts in scaffolding for bone tissue engineering. Arch Bone Jt Surg 2018; 6(2):90-9. [ Google Scholar]
- Li X, Wang L, Fan Y, Feng Q, Cui FZ, Watari F. Nanostructured scaffolds for bone tissue engineering. J Biomed Mater Res A 2013; 101(8):2424-35. doi: 10.1002/jbm.a.34539 [Crossref] [ Google Scholar]
- Jin HH, Kim DH, Kim TW, Shin KK, Jung JS, Park HC. In vivo evaluation of porous hydroxyapatite/chitosan-alginate composite scaffolds for bone tissue engineering. Int J Biol Macromol 2012; 51(5):1079-85. doi: 10.1016/j.ijbiomac.2012.08.027 [Crossref] [ Google Scholar]
- Szpalski C, Barbaro M, Sagebin F, Warren SM. Bone tissue engineering: current strategies and techniques--part II: cell types. Tissue Eng Part B Rev 2012; 18(4):258-69. doi: 10.1089/ten.TEB.2011.0440 [Crossref] [ Google Scholar]
- Burg KJ, Porter S, Kellam JF. Biomaterial developments for bone tissue engineering. Biomaterials 2000; 21(23):2347-59. doi: 10.1016/s0142-9612(00)00102-2 [Crossref] [ Google Scholar]
- Malekzadeh kebria M, Karimi A, Peyravian N, Delattre C, Ghasemian M, Michaud P. Designing and synthesis of In-Situ hydrogel based on pullulan/carboxymethyl chitosan containing parathyroid hormone for bone tissue engineering. Materialia 2024; 33:102026. doi: 10.1016/j.mtla.2024.102026 [Crossref] [ Google Scholar]
- Peyravian N, Brouki Milan P, Malekzadeh Kebria M, Mashayekhan S, Ghasemian M, Amiri S. Designing and synthesis of injectable hydrogel based on carboxymethyl cellulose/carboxymethyl chitosan containing QK peptide for femoral head osteonecrosis healing. Int J Biol Macromol 2024; 270(Pt 1):132127. doi: 10.1016/j.ijbiomac.2024.132127 [Crossref] [ Google Scholar]
- Amoupour M, Malekzadeh Kebria M, Hivechi A, Peyravian N, Ghasemian M, Mehrabi A, et al. Molecular mediators of vasculogenesis and angiogenesis. In: Kargozar S, Mozafari M, eds. Biomaterials for Vasculogenesis and Angiogenesis. Woodhead Publishing; 2022. p. 13-37. doi: 10.1016/b978-0-12-821867-9.00020-2.
- Mehrabi A, Zare Jalise S, Hivechi A, Habibi S, Malekzadeh Kebria M, Haramshahi MA. Evaluation of inherent properties of the carboxymethyl cellulose (CMC) for potential application in tissue engineering focusing on bone regeneration. Polym Adv Technol 2024; 35(1):e6258. doi: 10.1002/pat.6258 [Crossref] [ Google Scholar]
- Al-Allaq AA, Kashan JS, Abdul-Kareem FM. In vivo investigations of polymers in bone tissue engineering: a review study. Int J Polym Mater Polym Biomater 2024; 73(18):1664-84. doi: 10.1080/00914037.2024.2305227 [Crossref] [ Google Scholar]
- Aslam Khan MU, Aslam MA, Bin Abdullah MF, Stojanović GM. Current perspectives of protein in bone tissue engineering: bone structure, ideal scaffolds, fabrication techniques, applications, scopes, and future advances. ACS Appl Bio Mater 2024; 7(8):5082-106. doi: 10.1021/acsabm.4c00362 [Crossref] [ Google Scholar]
- Huang X, Lou Y, Duan Y, Liu H, Tian J, Shen Y. Biomaterial scaffolds in maxillofacial bone tissue engineering: a review of recent advances. Bioact Mater 2024; 33:129-56. doi: 10.1016/j.bioactmat.2023.10.031 [Crossref] [ Google Scholar]
- Gou Y, Huang Y, Luo W, Li Y, Zhao P, Zhong J. Adipose-derived mesenchymal stem cells (MSCs) are a superior cell source for bone tissue engineering. Bioact Mater 2024; 34:51-63. doi: 10.1016/j.bioactmat.2023.12.003 [Crossref] [ Google Scholar]
- Wu J, Cheng X, Wu J, Chen J, Pei X. The development of magnesium-based biomaterials in bone tissue engineering: a review. J Biomed Mater Res B Appl Biomater 2024; 112(1):e35326. doi: 10.1002/jbm.b.35326 [Crossref] [ Google Scholar]
- Niziołek K, Słota D, Sobczak-Kupiec A. Polysaccharide-based composite systems in bone tissue engineering: a review. Materials (Basel) 2024; 17(17):4220. doi: 10.3390/ma17174220 [Crossref] [ Google Scholar]
- Mistry AS, Pham QP, Schouten C, Yeh T, Christenson EM, Mikos AG. In vivo bone biocompatibility and degradation of porous fumarate-based polymer/alumoxane nanocomposites for bone tissue engineering. J Biomed Mater Res A 2010; 92(2):451-62. doi: 10.1002/jbm.a.32371 [Crossref] [ Google Scholar]
- Wiesmann HP, Joos U, Meyer U. Biological and biophysical principles in extracorporal bone tissue engineering Part II. Int J Oral Maxillofac Surg 2004; 33(6):523-30. doi: 10.1016/j.ijom.2004.04.005 [Crossref] [ Google Scholar]
- Lu HH, Kofron MD, El-Amin SF, Attawia MA, Laurencin CT. In vitro bone formation using muscle-derived cells: a new paradigm for bone tissue engineering using polymer-bone morphogenetic protein matrices. Biochem Biophys Res Commun 2003; 305(4):882-9. doi: 10.1016/s0006-291x(03)00858-1 [Crossref] [ Google Scholar]
- Bessot A, Medeiros Savi F, Gunter J, Mendhi J, Amini S, Waugh D, et al. Humanized in vivo bone tissue engineering: in vitro preculture conditions control the structural, cellular, and matrix composition of humanized bone organs. Adv Healthc Mater. 2024:e2401939. doi: 10.1002/adhm.202401939.
- Sun J, Gao Y, Yao Y, Li Y, Feng M, Bai L. Bone tissue engineering based on sustained release of MiR29c-modified framework nucleic acids from an injectable hydrogel. Chem Eng J 2024; 487:150706. doi: 10.1016/j.cej.2024.150706 [Crossref] [ Google Scholar]
- Negrescu AM, Mocanu AC, Miculescu F, Mitran V, Constantinescu AE, Cimpean A. In vitro studies on 3D-printed PLA/HA/GNP structures for bone tissue regeneration. Biomimetics (Basel) 2024; 9(1):55. doi: 10.3390/biomimetics9010055 [Crossref] [ Google Scholar]
- Iravani S, Nazarzadeh Zare E, Makvandi P. Multifunctional MXene-based platforms for soft and bone tissue regeneration and engineering. ACS Biomater Sci Eng 2024; 10(4):1892-909. doi: 10.1021/acsbiomaterials.3c01770 [Crossref] [ Google Scholar]
- Kumari S, Mondal P, Tyeb S, Chatterjee K. Visible light-based 3D bioprinted composite scaffolds of κ-carrageenan for bone tissue engineering applications. J Mater Chem B 2024; 12(7):1926-36. doi: 10.1039/d3tb02179c [Crossref] [ Google Scholar]
- Mu Y, Du Z, Gao W, Xiao L, Crawford R, Xiao Y. The effect of a bionic bone ionic environment on osteogenesis, osteoimmunology, and in situ bone tissue engineering. Biomaterials 2024; 304:122410. doi: 10.1016/j.biomaterials.2023.122410 [Crossref] [ Google Scholar]
- Qin L, Yang S, Zhao C, Yang J, Li F, Xu Z. Prospects and challenges for the application of tissue engineering technologies in the treatment of bone infections. Bone Res 2024; 12(1):28. doi: 10.1038/s41413-024-00332-w [Crossref] [ Google Scholar]
- Xiang E, Vaquette C, Liu S, Raveendran N, Schulz BL, Nowwarote N. Biomimetic surface nanoengineering of biodegradable Zn-based orthopedic implants for enhanced biocompatibility and immunomodulation. Adv Funct Mater 2024; 34(51):2410033. doi: 10.1002/adfm.202410033 [Crossref] [ Google Scholar]
- Zhong C, Zhu H, Sheng Y, Wo J, You D, Sun G. Biocompatibility and osteogenic potential of choline phosphate chitosan-coated biodegradable Zn1Mg. Acta Biomater 2024; 175:395-410. doi: 10.1016/j.actbio.2023.12.014 [Crossref] [ Google Scholar]
- Taghvaei AH, Mosadeghian F, Mosleh-Shirazi S, Ebrahimi A, Kaňuchová M, Girman V. Fabrication and characterization of novel ZnO-loaded mesoporous bioactive glass nanospheres with enhanced physiochemical properties and biocompatibility for bone tissue engineering. J Non Cryst Solids 2024; 626:122781. doi: 10.1016/j.jnoncrysol.2023.122781 [Crossref] [ Google Scholar]
- Ansari MM, Heo Y, Do K, Ghosh M, Son Y-O. Nanocellulose derived from agricultural biowaste by-products–Sustainable synthesis, biocompatibility, biomedical applications, and future perspectives: A review. Carbohydr Polym Technol Appl 2024; 8:100529. doi: 10.1016/j.carpta.2024.100529 [Crossref] [ Google Scholar]
- Gnanasekaran R, Yuvaraj D, Muthu CMM, Ashwin R, Kaarthikeyan K, Kumar VV. Extraction and characterization of biocompatible hydroxyapatite (Hap) from red big eye fish bone: potential for biomedical applications and reducing biowastes. Sustain Chem Environ 2024; 7:100142. doi: 10.1016/j.scenv.2024.100142 [Crossref] [ Google Scholar]
- Feng H, Yue Y, Zhang Y, Liang J, Liu L, Wang Q. Plant-derived exosome-like nanoparticles: emerging nanosystems for enhanced tissue engineering. Int J Nanomedicine 2024; 19:1189-204. doi: 10.2147/ijn.S448905 [Crossref] [ Google Scholar]
- Posada VM, Ramírez J, Civantos A, Fernández-Morales P, Allain JP. Ion-bombardment-driven surface modification of porous magnesium scaffolds: enhancing biocompatibility and osteoimmunomodulation. Colloids Surf B Biointerfaces 2024; 234:113717. doi: 10.1016/j.colsurfb.2023.113717 [Crossref] [ Google Scholar]
- Feng Q, Zhou X, He C. NIR light-facilitated bone tissue engineering. Wiley Interdiscip Rev Nanomed Nanobiotechnol 2024; 16(1):e1925. doi: 10.1002/wnan.1925 [Crossref] [ Google Scholar]
- Hao Z, Chen T, Wang Y, Feng Q, Chen J, Li H. Self-assembling peptide nanofibers anchored parathyroid hormone derivative for bone tissue engineering. Adv Fiber Mater 2024; 6(2):583-606. doi: 10.1007/s42765-023-00370-9 [Crossref] [ Google Scholar]
- Anjum S, Wang Y, Xin Y, Li X, Li T, Zhang H. Bioinspired core-shell nanofiber drug-delivery system modulates osteogenic and osteoclast activity for bone tissue regeneration. Mater Today Bio 2024; 26:101088. doi: 10.1016/j.mtbio.2024.101088 [Crossref] [ Google Scholar]
- Shanmugavadivu A, Lekhavadhani S, Babu S, Suresh N, Selvamurugan N. Magnesium-incorporated biocomposite scaffolds: a novel frontier in bone tissue engineering. J Magnes Alloys 2024; 12(6):2231-48. doi: 10.1016/j.jma.2024.06.001 [Crossref] [ Google Scholar]
- Lv N, Zhou Z, Hou M, Hong L, Li H, Qian Z. Research progress of vascularization strategies of tissue-engineered bone. Front Bioeng Biotechnol 2023; 11:1291969. doi: 10.3389/fbioe.2023.1291969 [Crossref] [ Google Scholar]
- Zhang X, Nan K, Zhang Y, Song K, Geng Z, Shang D. A novel injectable hydrogel prepared from phenylboronic acid modified gelatin and oxidized-dextran for bone tissue engineering. Int J Biol Macromol 2024; 261(Pt 1):129666. doi: 10.1016/j.ijbiomac.2024.129666 [Crossref] [ Google Scholar]
- Luo S, Wang Z, He J, Tang G, Yuan D, Wu Z. Bioceramic modular tissue-engineered bone with rapid vascularization for large bone defects. Ceram Int 2024; 50(11 Pt A):18275-83. doi: 10.1016/j.ceramint.2024.02.311 [Crossref] [ Google Scholar]