Avicenna J Dent Res. 17(1):14-20.
doi: 10.34172/ajdr.1985
Review Article
Prevalence of Tortuous Temporomandibular Joint Disorders: A Systematic Review and Meta-analysis
K Yesoda Aniyan Conceptualization, Data curation, Writing – original draft, 1, * 
C L Krithika Conceptualization, Data curation, 1
G Anuradha Writing – review & editing, 1
Author information:
1SRM Dental College, Ramapuram, Bharathi Salai, Chennai, TN, India
Abstract
Background: Temporomandibular disorder (TMD) is a cumulative terminology that demonstrates musculoskeletal and neuromuscular disorders. It is of extreme relevance that the number of subjects with TMD-related pain has noticeably increased over the recent years. This could be attributed to the increased stress in lifestyles and use of electronic devices (smartphones/laptops/tablets), altering the posture across the boundaries of age, gender, and geography. Thus, this systematic review and meta-analysis was conducted to derive the prevalence of TMD disorders across the aforementioned boundaries.
Methods: The method used in this study to quantify the prevalence of TMD across the countries and populations was in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. MEDLINE, Scopus, Web of Science, and Google Scholar were systematically searched until July 30, 2024.
Results: The quality of the prevalence studies was assessed using Critical Appraisal Skills Programme (CASP) Tools. The bias within the study data was evaluated using RevMan software, and the prevalence was calculated as 25.8%. Finally, the forest plot was employed to determine the weightages and risk ratios of the studies.
Conclusion: Based on the findings, there has been a slow and steady increase in the prevalence of TMD, and thus sustainable measures are imminent for controlling this disorder.
Keywords: Temporomandibular disorder, Temporomandibular joint, Prevalence, Evidence-based dentistry, Systematic review, Meta-analysis
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Yesoda Aniyan K, Krithika C L, Anuradha G. Prevalence of tortuous temporomandibular joint disorders: a systematic review and meta-analysis. Avicenna J Dent Res. 2025;17(1):14-20. doi:10.34172/ajdr.1985
Background
The temporomandibular joint (TMJ) is a synovial joint present on both sides of the craniomandibular complex. The connecting anatomical configurations are key in jaw movement, enabling everyday tasks of chewing, swallowing, and speaking. The manner of its function ensures non-damage of the anatomy from the stresses generated from each of the aforesaid functions (1). Temporomandibular disorder (TMD) is a cumulative terminology representing musculoskeletal and neuromuscular disorders, symptomized by pain and/or dysfunction in the masticatory muscles, TMJ, and associated structures. Additional related comorbidities are inclusive of headaches, fibromyalgia, tinnitus, chronic fatigue syndrome, depression, and sleep disturbances (2).
The diagnosis and management of this disorder become challenging with its myriad associated symptoms. This is compounded by the varied classifications, followed by Research Diagnostic Criteria (RDC/TMD) and diagnostic criteria (DC/TMD), which are currently being used among diagnosticians (3,4). It is highly noticeable that the number of subjects being reported with TMD-related pain has considerably increased over the years. This could be associated with the increased stress in lifestyles and use of electronic devices (laptops/smartphones/tablets) that has altered the posture across gender, age, and geography boundaries (5). The existing literature predominantly reports the prevalence of TMD among adults alone. Researchers indicate that the knowledge of the prevalence of the disorder would aid as a first step answer to the aforementioned obstacles. It would enable patient literacy of the important preventive methods against disorder development as well as maintenance against symptom worsening. With these research questions as a crux, the following systematic review and meta-analysis was performed to derive the prevalence of TMD disorders across the world.
Materials and Methods
Protocol
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis checklist (PRISMA) (6).The protocol was elaborated in accordance with PRISMA-P (7). All the methods of data collection/analysis and the inclusion/exclusion criteria were prespecified and documented in the review protocol.
Eligibility Criteria
Inclusion Criteria
-
Studies reporting the prevalence of TMD in the general population
-
No restrictions pertaining to the age or gender of the participants in the study
-
Language of referenced articles with no restrictions
-
All diagnoses of TMD, irrespective of the presence and absence of pain
Exclusion Criteria
-
Narrative reviews, systematic reviews, meta-analyses, case reports or series patients, animal or biomechanical studies, and post-conference abstracts
-
Duplicate studies
-
Studies with patients reporting secondary oral and systemic conditions such as prosthesis, orthodontic treatment, and partial or completely edentulous subjects
-
Studies with restrictions in subject selection, such as fibromyalgia, systemic joint hypermobility, arthritis, tinnitus, post-traumatic stress disorder, trigeminal neuralgia, burning mouth syndrome, atypical facial pain, migraine, atypical odontalgia, cervical pain, neuropathic pain, and dentoskeletal deformities or fractures and congenital/developmental disorders or syndromes associated with TMD
-
Data from reviews, letters, books, conference abstracts, expert opinions, technique articles, posters, guidelines, and pilot studies
Information Sources and Search
A detailed and rigorous systematic review search was conducted primarily in PubMed, followed by Scopus and Web of Science (Figure 1), by two researchers (Y.A. and K.C.L.), with the opinion of the third author (A.G.) used in the event of any disagreement. An additional literature search was performed in Google Scholar, and a manual search was conducted in the institute’s central library in the event of non-accessibility of a complete literature text. The MeSH terminologies searched in this regard included “Temporomandibular joint disorders AND prevalence”, “Temporomandibular joint disorders AND epidemiology”, and “Temporomandibular joint disorders AND population” from January 1, 2019 to July 30, 2024. The Cohen kappa statistic between the reviewers was 0.97, indicating substantial agreement.
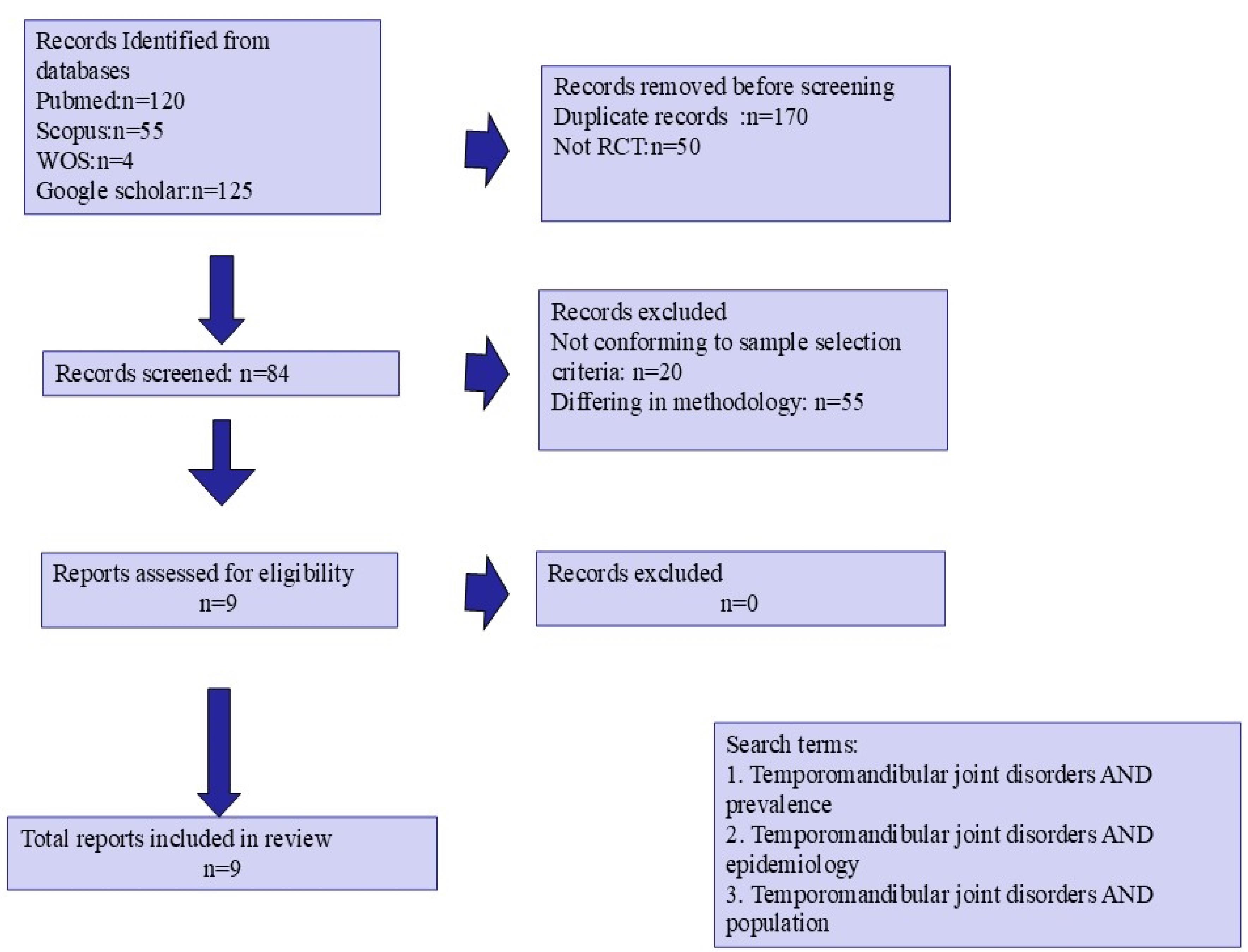
Figure 1.
PRISMA Flowchart Illustrating the Search Strategy. Note. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analysis Checklist
.
PRISMA Flowchart Illustrating the Search Strategy. Note. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analysis Checklist
Risk of Bias in Individual Studies
Two of the authors (K.C.L. and A.G.) used the Critical Appraisal Skills Programme (CASP) Tools for the quality assessment of the selected studies. The CASP had 11 points per study, according to four quality domains, namely, basic study design, methodology validation, the completeness and quality of results, and finally the helpfulness of the results in the local scenario. In the currently reported study, all articles were ascribed to the CASP checklist. The data were further tabulated, inclusive of the main assessment criterion, in Tables 1 and 2, respectively. Further, the risk assessment within the study was performed using RevMan software.
Table 1.
Summary of Selected Articles
|
Study
|
Place
|
Year
|
Sample/
Male: Female
|
Mean Age
(y)
|
Diagnostic Criteria
|
| Filho et al (8) |
Brazil |
2020 |
2624
F = 1,647
M = 977 |
21.5 |
American Academy of Orofacial Pain |
| Yap and Natu (9) |
Singapore |
2020 |
400
M = 191
F = 209 |
19.26 ± 1.89 |
RDC/TMD |
| Natu et al (10) |
Singapore |
2018 |
181
M = 37
F = 207 |
19 |
-
Fonseca’s Anamnestic Index
-
Oral Health Impact Profile for Temporomandibular Disorders
|
| Paz-Cortés et al (11) |
Spain |
2024 |
70
M = 38
F = 32 |
21.5 |
-
DC/TMD criteria
-
Fonseca Anamnestic Index
-
Helkimo Index modified by Maglione
|
| Wu et al (12) |
China |
2021 |
754
M = 354
F = 400 |
21.5 |
DC/TMD |
| Romani et al (13) |
Italy |
2018 |
106
M = 47
F = 59 |
10.4 |
Fonseca’s Questionnaire |
| Sanders et al (14) |
USA |
2013 |
3263 |
31.5 |
RDC/TMD criteria |
| Jomhawi et al (15) |
Jordan |
2021 |
396
M = 200
F = 196 |
16 |
RDC/TMD |
| de Melo Júnior et al (16) |
Brazil |
2019 |
1342
M = 421
F = 921 |
12 |
RDC/TMD |
Note. DC/TMD: Diagnostic Criteria for Temporomandibular Disorders; RDC/TMD: Research Diagnostic Criteria for Temporomandibular Disorders.
Table 2.
Summary of Data of Selected Articles
|
Study
|
Diagnosis
|
Other Assessed Factors
|
Sampling
|
Prevalence
|
Outcomes
|
| Filho et al (8) |
TMD |
-
Oral Health Impact Profile (OHIP-14)
|
Random |
557 (21%)
M:F = NA |
-
TMD prevalence: 557 (72%)
-
Impact on quality of life (with TMD): 133 (17.38%)
|
| Yap and Natu (9) |
TMD |
-
Patient Health Questionnaire-15 (PHQ-15)
-
Depression, Anxiety, and Stress Scales-21
-
TMD pain screener
|
Random |
34 (9%)
M:F = 11:23 |
-
TMD prevalence: 8.5% (34)
-
M = 11, F = 23
-
PHQ-15 mean: 11.5
-
Depression scores mean: 14.94
-
Anxiety scores mean: 14.82
-
Stress scores mean: 17.06
|
| Natu et al (10) |
TMD |
-
Depression Anxiety Stress Scales-21
-
Pittsburgh Sleep Quality Index
|
Random |
102 (41.8)
M:F = NA |
-
Total TMD prevalence: 41.8%
-
Mild TMD: 32.4% (79)
-
Moderate TMD: 9.4%
-
F > M = 83.3%
-
An increase in the OHIP score as per TMD severity
-
An increase in depression and anxiety scores as per TMD severity
|
| Paz-Cortés et al (11) |
TMD |
-
Perceived Stress Scale (PSS-14)
-
Salivary cortisol
-
Criteria for Classification of Occlusion.
-
State-Trait Anxiety Inventory
|
Random |
38 (54.28%) |
-
No significant association with gender, occlusion, and TMD observed
-
Positive correlation with stress and anxiety
|
| Wu et al (12) |
TMD |
-
Patient Health Questionnaire-9 (PHQ-9)
-
Generalized Anxiety Disorder
-
Scale-7
-
Pittsburgh Sleep Quality Index
|
Random |
239 (31.7%) |
-
TMD prevalence: 31.7%
-
Mild depression: 52.3%
-
Moderate depression: 15.5%
-
Severe depression: 2.1%
-
Depression: 69.9%
-
Anxiety: 69.5%
-
Sleep disorder: 51.5%
|
| Romani et al (13) |
TMD signs |
Revised Children’s Manifest Anxiety Scale |
Random |
91 (86.39%)
F = 74 (82%)
M = 32% |
-
TMD prevalence: 86.79%
-
F = 39%, M = 23%
-
Positive association between TMD and anxiety
|
| Sanders et al (14) |
TMD signs |
-
OPPERA Comprehensive Pain and Symptom Questionnaire
-
Health status
-
Pittsburgh Sleep Quality Index
-
Anthropometric Status
-
Cigarette Smoking
-
Short Form 12 Health Survey V2 (SF-12v2)
|
Random |
260 (8%) |
Positive association of an increase in TMD incidence in association-assessed factors of chronic back pain, altered sleep, smoking, and health disorders |
| Jomhawi et al (15) |
TMD |
Nil |
Random |
TMD prevalence = 29%
15 years = 20 (40%)
16 years = 49 (28.2%)
17 years = 46 (27.4%) |
-
TMD prevalence: 29%
-
M > F = disability, depression, and unspecific physical symptoms
-
Low disability-low-intensity pain: 64.9%
-
Severe depression: 69.6%
-
TMD without pain: 53%
-
TMD with pain: 57.4%
|
| de Melo Júnior et al (16) |
TMD |
Brazilian Economic Classification Criteria |
Random |
TMD = 446 (33.2%) |
-
TMD prevalence: 446 (33.2%)
-
Peak age: 12 years
-
TMD with headache: 162.16 (36.4%)
-
Low disability: 24.6%
-
High disability: 3.2%
-
Females: 68%
-
Low socio-economic level: 60%
|
Note. TMD: Temporomandibular Disorders; OPPERA: Orofacial Pain: Prospective Evaluation and Risk Assessment.
Results
In the selected studies (N = 8), the total number of subjects amounted to 5992, including 754 males and 2691 females, and 2547 of them were of unspecified gender. The ages of the participants ranged from 10 years to 40 years. In addition, DC/TMD (1 study), RDC/TMD (n = 2), American Academy of Orofacial Pain (n = 1), TMD pain screener (n = 1), Fonseca’s Anamnestic Index (n = 3), Oral Health Impact Profile for RMD (n = 1), and Helkimo Index modified by Maglione (n = 1) were used for diagnosis. The study reports ranged from 7 varied countries, with the sample size varying from 70 to 3,263. A summary of the descriptions of the studies is listed in Tables 1 and 2.
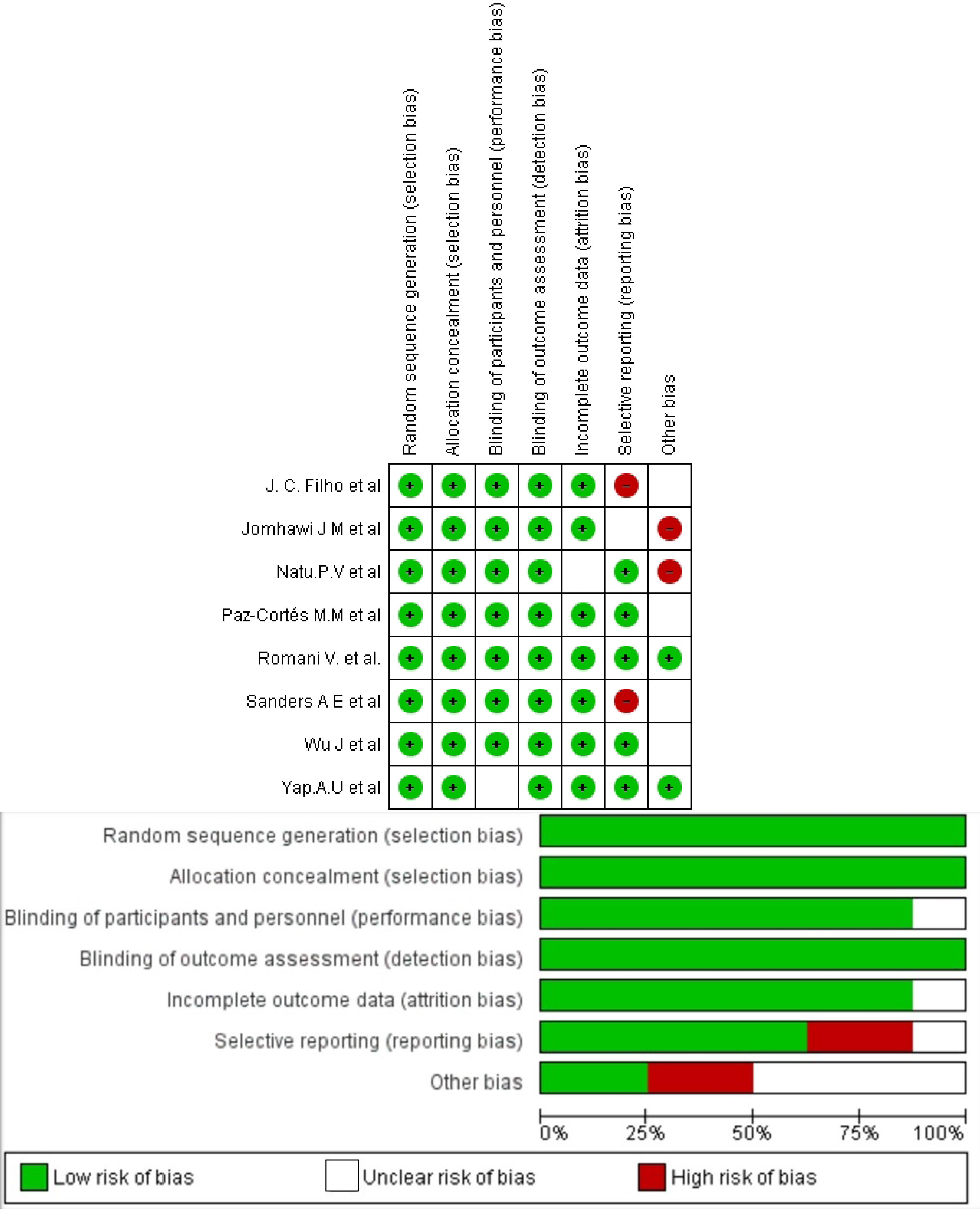
Figure 2.
Risk of Bias Assessment of Selected Articles
.
Risk of Bias Assessment of Selected Articles
For article selection, articles using RDC/TMD, DC/TMD, Fonseca’s Questionnaire, Oral Health Impact Profile for RMD, and American Academy of Orofacial Pain were included in the study as the authors convened that under the expert supervision, the criteria for diagnosis would not impact the study quality in terms of diagnosis. Conversely, they indicated that the exclusion would hamper the accurate approximation of the prevalence of the disorder. All the selected studies reported a higher observation of the disorder in the female gender. However, not all the studies ascertained a numerical value in results, thus hampering numerical calculation in this meta-analysis. The mean age of presentation ranged from 10 years to 31.5 years. Considering that the studies also reported the group prevalence, it was impossible to assess the sub-group diagnosis of which type of TMD was prevalent. The heterogeneity among the studies in the meta-analyses was high (I2 = 99%), owing to differences in the characteristics of the sample, and thus a random effect was taken into consideration. Based on the tabulated data, the prevalence of TMD in this meta-analysis at a 95% confidence interval was 25.8%. The effect estimate was 0.28.
The forest plot (Figure 3) was calculated to determine the risk ratio and weightages of the study. The study by Wu et al had the maximum weightage at 26.4%. It was concluded that the number of subjects suffering from TMD was statistically significant.
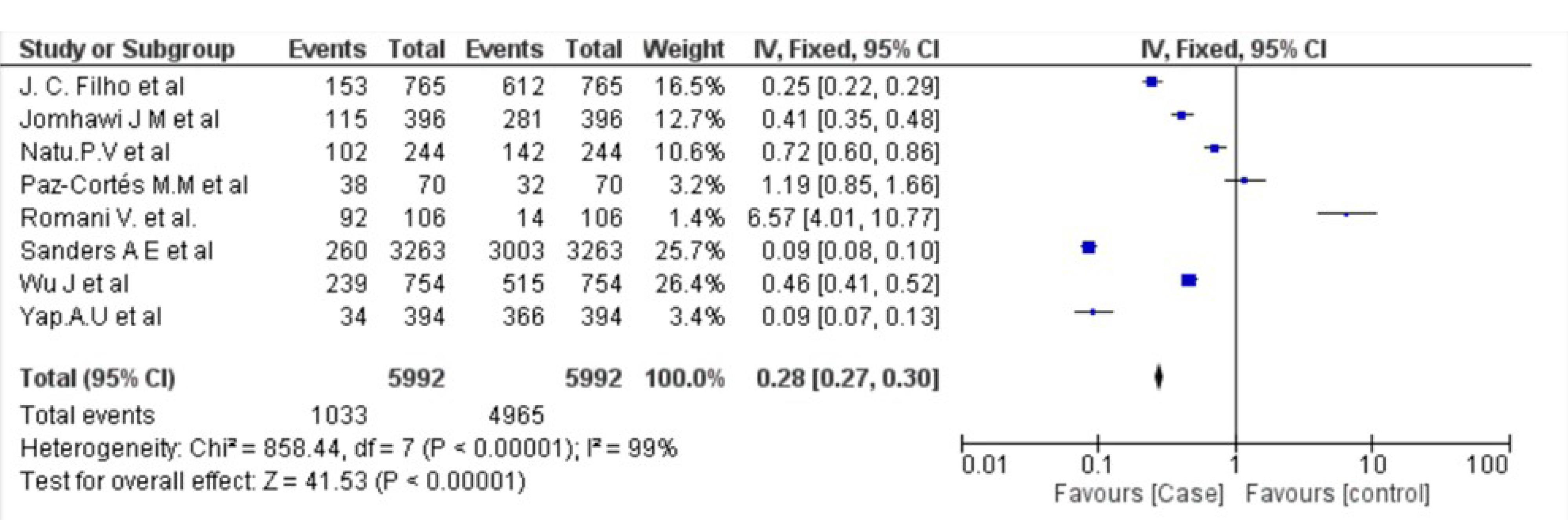
Figure 3.
Forest Plot Displaying the Weightage and Risk Ratio of Selected Studies
.
Forest Plot Displaying the Weightage and Risk Ratio of Selected Studies
Discussion
This systematic review was conducted to estimate the prevalence of TMD across the globe, populations, and age groups. The prevalence rates reported in the selected studies were acquired from educational institutions and healthcare centers of private and public domains in different geographic locations. These contribute to a more probable accurate assessment, unlike pain clinics or TMD specialization clinics, which would overreport the prevalence in a population, thus ascertaining the case group in a general population would be challenging.
Of the 8 studies, 5 evaluated the depression and anxiety scores (Table 2) using validated scales. Unanimously, a significant positive association was found irrespective of age and geographical location. It was noted that there was a significant rise in the stress scores of children and adolescents (10,11,13,15), which is in line with the reporting by Dickson et al, evaluating anxiety disorder in children (17).The mechanism is such that the inflammatory factors produced in pain cross the blood-brain barrier and alter the neurotransmitter metabolism and neuroendocrine function, thereby causing depression (18).
Among the selected studies, 4 assessed the health status of the patient through validated patient-filled questionnaires using the Quality of Life (QoL) Questionnaire (8,9,12,14). QoL is a multidimensional feature classifying the positivity with which a young individual rates his/her life circumstances and state. It crosses the boundaries of psychological symptoms to a comprehensive sense of well-being and life satisfaction inclusive of physical, psychological, and social functioning. In this study, a positive correlation was noted wherein a dip in scores of QoL was associated with TMD, which conforms to the findings of Pigozzi et al (19). One of the studies(16) evaluated the association of lower socio-economic status with the prevalence of TMD and reported a proportional alteration, which matches the results of a meta-analysis performed by Minervini et al (20).
In this meta-analysis, the obtained prevalence was 25.8%. However, this rate was 23% in a previous meta-analysis by Valesan et al (21). The previous study reported this value around 5 years earlier. The researchers were in consensus that there was a gradual rise in the prevalence of the disorder. This can be attributed to lifestyle changes, along with anxiety and depression levels in the community.
The greatest limitation of this study was the unanimous absence of imaging studies for the confirmation of TMD (22). Additionally, adequate sample size representation and calculation require multicentric observations, which were reported in only two studies performed by Jomhawi et al and de Melo Júnior et al, respectively (15,16).
Conclusion
Based on the findings, the prevalence of TMD represents a gradual rise. Considering the chronic nature of the disorder and the high cost of treatment, sustainable treatment alternatives and prevention strategies are the need of the time (23). Oral literacy programs for prevention and the need for management at the first sign of the disorder can be introduced at the school level as the manifestation of this disorder starts in the age group. Sustainable medications from natural resources with lower costs and adverse effects are the other challenges that need to be overcome.
Competing Interests
Nil.
Ethical Approval
Not applicable.
Funding
This study was not funded by any private or public organization.
References
- Li DT, Leung YY. Temporomandibular disorders: current concepts and controversies in diagnosis and management. Diagnostics (Basel) 2021; 11(3):459. doi: 10.3390/diagnostics11030459 [Crossref] [ Google Scholar]
- Kapos FP, Exposto FG, Oyarzo JF, Durham J. Temporomandibular disorders: a review of current concepts in aetiology, diagnosis and management. Oral Surg 2020; 13(4):321-34. doi: 10.1111/ors.12473 [Crossref] [ Google Scholar]
- Schiffman E, Ohrbach R, Truelove E, Look J, Anderson G, Goulet JP. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. J Oral Facial Pain Headache 2014; 28(1):6-27. doi: 10.11607/jop.1151 [Crossref] [ Google Scholar]
- Dworkin SF, LeResche L. Research diagnostic criteria for temporomandibular disorders: review, criteria, examinations and specifications, critique. J Craniomandib Disord 1992; 6(4):301-55. [ Google Scholar]
- Al-Baghdadi M, Durham J, Araujo-Soares V, Robalino S, Errington L, Steele J. TMJ disc displacement without reduction management: a systematic review. J Dent Res 2014; 93(7 Suppl):37S-51S. doi: 10.1177/0022034514528333 [Crossref] [ Google Scholar]
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009; 6(7):e1000097. doi: 10.1371/journal.pmed.1000097 [Crossref] [ Google Scholar]
- Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. Bmj 2015; 350:g7647. doi: 10.1136/bmj.g7647 [Crossref] [ Google Scholar]
- Filho JC, Vedovello SA, Venezian GC, Vedovello Filho M, Degan VV. Women’s oral health-related quality of life as a risk factor for TMD symptoms A case-control study. Cranio 2023; 41(2):139-43. doi: 10.1080/08869634.2020.1833159 [Crossref] [ Google Scholar]
- Yap AU, Natu VP. Inter-relationships between pain-related temporomandibular disorders, somatic and psychological symptoms in Asian youths. J Oral Rehabil 2020; 47(9):1077-83. doi: 10.1111/joor.13033 [Crossref] [ Google Scholar]
- Natu VP, Yap AU, Su MH, Irfan Ali NM, Ansari A. Temporomandibular disorder symptoms and their association with quality of life, emotional states and sleep quality in South-East Asian youths. J Oral Rehabil 2018; 45(10):756-63. doi: 10.1111/joor.12692 [Crossref] [ Google Scholar]
- Paz-Cortés MM, Martín-Vacas A, Mendoza PA, Rozalén M, Alvaredo M. Analysis of the effect of exams on perceived stress and temporomandibular joint status in physiotherapy students: a pilot study. Medicina (Kaunas) 2024; 60(6):952. doi: 10.3390/medicina60060952 [Crossref] [ Google Scholar]
- Wu J, Huang Z, Chen Y, Chen Y, Pan Z, Gu Y. Temporomandibular disorders among medical students in China: prevalence, biological and psychological risk factors. BMC Oral Health 2021; 21(1):549. doi: 10.1186/s12903-021-01916-2 [Crossref] [ Google Scholar]
- Romani V, Di Giorgio R, Castellano M, Barbato E, Galluccio G. Prevalence of craniomandibular disorders in orthodontic pediatric population and possible interactions with anxiety and stress. Eur J Paediatr Dent 2018; 19(4):317-23. doi: 10.23804/ejpd.2018.19.04.13 [Crossref] [ Google Scholar]
- Sanders AE, Slade GD, Bair E, Fillingim RB, Knott C, Dubner R. General health status and incidence of first-onset temporomandibular disorder: the OPPERA prospective cohort study. J Pain 2013; 14(12 Suppl):T51-62. doi: 10.1016/j.jpain.2013.06.001 [Crossref] [ Google Scholar]
- Jomhawi JM, Elsamarneh AM, Hassan AM. Prevalence of temporomandibular disorder among schoolchildren in Jordan. Int J Clin Pediatr Dent 2021; 14(2):304-10. doi: 10.5005/jp-journals-10005-1939 [Crossref] [ Google Scholar]
- de Melo Júnior PC, Aroucha J, Arnaud M, de Souza Lima MG, Gomes SG, Ximenes R. Prevalence of TMD and level of chronic pain in a group of Brazilian adolescents. PLoS One 2019; 14(2):e0205874. doi: 10.1371/journal.pone.0205874 [Crossref] [ Google Scholar]
- Dickson SJ, Oar EL, Kangas M, Johnco CJ, Lavell CH, Seaton AH. A systematic review and meta-analysis of impairment and quality of life in children and adolescents with anxiety disorders. Clin Child Fam Psychol Rev 2024; 27(2):342-56. doi: 10.1007/s10567-024-00484-5 [Crossref] [ Google Scholar]
- Meda RT, Nuguru SP, Rachakonda S, Sripathi S, Khan MI, Patel N. Chronic pain-induced depression: a review of prevalence and management. Cureus 2022; 14(8):e28416. doi: 10.7759/cureus.28416 [Crossref] [ Google Scholar]
- Pigozzi LB, Pereira DD, Pattussi MP, Moret-Tatay C, Irigaray TQ, Weber JB. Quality of life in young and middle age adult temporomandibular disorders patients and asymptomatic subjects: a systematic review and meta-analysis. Health Qual Life Outcomes 2021; 19(1):83. doi: 10.1186/s12955-021-01727-7 [Crossref] [ Google Scholar]
- Minervini G, Franco R, Marrapodi MM, Fiorillo L, Cervino G, Cicciù M. Economic inequalities and temporomandibular disorders: a systematic review with meta-analysis. J Oral Rehabil 2023; 50(8):715-23. doi: 10.1111/joor.13491 [Crossref] [ Google Scholar]
- Valesan LF, Da-Cas CD, Réus JC, Denardin AC, Garanhani RR, Bonotto D. Prevalence of temporomandibular joint disorders: a systematic review and meta-analysis. Clin Oral Investig 2021; 25(2):441-53. doi: 10.1007/s00784-020-03710-w [Crossref] [ Google Scholar]
- Sivakumar A, Ganesan A, Lakshmi KC, Aniyan Y, Kannan S. Evaluation of the articular disc using the magnetic resonance CartiGram in asymptomatic and symptomatic temporomandibular disorders. Indian J Radiol Imaging 2025; 35(1):50-8. doi: 10.1055/s-0044-1788608 [Crossref] [ Google Scholar]
- Aniyan KY, Patil K, Guledgud MV. Assessment of knowledge, attitude, and practice of oral disease management among doctors practicing the Ayurveda system of medicine: a questionnaire-based study guide to unconventional dentistry. J Indian Acad Oral Med Radiol 2023; 35(2):222-5. doi: 10.4103/jiaomr.jiaomr_291_22 [Crossref] [ Google Scholar]