Avicenna J Dent Res. 17(2):101-108.
doi: 10.34172/ajdr.1973
Original Article
Marginal Microleakage Evaluation in Class II Cavities Restored With Composite, Resin-Modified Glass Ionomer, and Bulk-Fill Bioactive Composite: An In Vitro Study
Safaa Shihabi Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Writing – original draft, Writing – review & editing, 1, * 
Mohammed Bashier AL-Monaquel Supervision, Validation, Visualization, 1
Author information:
1Pediatric Dentistry, Faculty of Dentistry, Damascus University, Syria
Abstract
Background: Restoring primary teeth with an aesthetic restorative material such as composite is a challenge in pediatric dentistry. Despite advancements, the ideal aesthetic restoration material remains just a debate. Thus, current studies are seeking to find a bio-restorative material to avoid composite negatives while maintaining cosmetic benefits. The bioactive composite is one of these materials, but its effectiveness and properties are still under study. This in-vitro study aimed to evaluate the marginal microleakage of class II cavities in primary molars restored with the bioactive composite and to compare it with the conventional composite and resin-modified glass ionomer (RMGI) cement.
Methods: Overall, 45 standardized class II cavities were prepared in primary molars and restored with the bioactive composite, conventional composite, and RMGI according to manufacturers’ instructions. The restored teeth were subjected to 1000 thermocycles, followed by sealing the internal surfaces with wax before immersion in 0.5% methylene blue for 4 hours. Then, the teeth were sectioned mesiodistally to evaluate dye penetration under a microscope by two specialized pedodontists and according to a 4-degree scale.
Results: Statistical analysis revealed no statistically significant difference in the marginal microleakage of occlusal and gingival surfaces among the bioactive composite, RMGI, and conventional composite (P values 0.104 and 0.160, respectively). However, within the same group, a statistically significant difference was observed between occlusal and gingival surfaces in the bioactive composite, traditional composite, and RMGI, with lower occlusal microleakage (P values 0.020, 0.046, and 0.000, respectively). Multiple nominal logistic regression demonstrated no influence of being the molar upper or lower first or second on the marginal microleakage (P>0.05).
Conclusion: Based on the present microleakage study, there was no significant difference between the microleakage values of the bioactive composite compared with the conventional composite and RMGI.
Keywords: Microleakage, Bioactive composite, Bulk-Fill, RMGI, Class II cavity, Primary teeth
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Shihabi S, AL-monaquel MB. Marginal microleakage evaluation in class II cavities restored with composite, resin-modified glass ionomer, and bulk-fill bioactive composite: an in vitro study. Avicenna J Dent Res. 2025;17(2):101-108. doi:10.34172/ajdr.1973
Background
The use of restoration materials placed on primary teeth with caries is the myost common procedure among pediatric dentists (1). In pediatric dentistry, there are many restoration materials used to restore decayed teeth, such as amalgam, composite, glass ionomer cement, resin-modified glass ionomer cement (RMGI), and compomer (2,3). In recent years, there has been a notable shift toward aesthetic considerations even in pediatric dental procedures, leading to a decline in using traditional amalgam fillings compared with composite, RMGI, and other aesthetic restoration materials (3).
Nowadays, composite has become the first esthetic choice for restoring posterior and anterior primary teeth, especially in low-income countries, because of its satisfactory esthetic quality, conservative procedure, repairability, and cost-efficiency (1).Despite improvements in the clinical performance of the resin composite, its application is still a challenge in pediatric dentistry because of the sensitivity of the procedure, which requires cooperative children to perform a satisfactory restoration with fewer steps in a short time(4). Furthermore, the integrity at the tooth-composite interface cannot be achieved because of polymerization shrinkage stress, leading to marginal microleakage, secondary caries, and subsequently the failure of the restoration (3).
Despite advancements, the ideal aesthetic restoration material remains elusive due to concerns such as recurrent caries, microleakage, and material longevity (5).
Microleakage, defined as the passage of bacteria, fluids, ions, and saliva between the cavity wall and the restoration material, remains the main factor that affects the permanence and longevity of composite restoration in the oral cavity. Therefore, achieving a perfect seal to reduce secondary caries, sensitivity, and failure due to polymerization shrinkage is paramount in selecting aesthetic restoration materials in clinical practice. (3,4,5,6)
Literature reviews suggest that RMGI has a remineralization effect, can release ions in acidic environments, and offers superior adhesion and sealing properties along with satisfactory aesthetics, but its mechanical properties and abrasion resistance remain controversial (7).
Recently, the bioactive composite has been introduced as a restoration material that combines the desirable characteristics of both conventional composites and RMGI (4). It has the ability to release calcium, sodium, and phosphate ions in an aqueous environment, stimulating remineralization processes; for instance, releasing such ions raises pH and inhibits the pathogenesis of oral microorganisms. It can also stimulate apatite formation at the restoration-tooth interface, preventing the development of recurrent carious lesions and reducing marginal microleakage while maintaining high physical properties (8).
Moreover, it is introduced as a bulk-fill composite, which simplifies the application procedure and decreases chair time, especially in the case of deep class II cavities in primary teeth (9).
To the best of our knowledge, the number of studies that evaluate the marginal microleakage of class II bioactive composite restorations in primary teeth is limited, and many studies should be performed to support or refute the findings previously published in the medical literature.
Accordingly, this study aimed to determine the marginal microleakage of the bioactive composite compared with the conventional composite and RMGI in class II cavities in primary teeth.
Hypotheses of the Study
Null Hypothesis (H0): There is no statistically significant difference in occlusal/gingival microleakage among the bioactive composite, traditional composite, and RMGI.
Alternative Hypothesis (H1): There is a statistically significant difference in occlusal/gingival microleakage among the bioactive composite, traditional composite, and RMGI.
Materials and Methods
The Checklist for Reporting In-Vitro Studies guidelines were followed for reporting this in-vitro experimental study (10).
Sample Calculation and Collection
This was an experimental, randomized, and single-blinded study. The sample size was calculated by G*Power 3.1.9.7. A total of 45 upper and lower primary molars were freshly extracted for orthodontic reasons and utilized as samples.
There were some inclusion criteria for this investigation; each tooth had to have at least one-third of the root, exhibit an intact and non-carious surface devoid of restorations, and have enamel developmental disorders, white spot lesions, cracks, or fractures. These criteria were assessed under a stereoscopic microscope (Meiji; Japan) at 2x magnification (11).
Preparation of Specimens and Group Allocation
The teeth were cleaned with a hand scaler (Ck-6, Zeffiro; Italy) to remove residual tissue, polished with a rubber cup and pumice, and then stored in 0.5% chloramine T in plastic containers for one week. Following this initial storage period, the teeth were transferred to containers filled with distilled water and kept at room temperature until utilized in the study. (11-13).
Randomization, Blinding, and Group Assignment
The teeth were randomly divided into three groups according to restoration material (Table 1), each containing 15 upper or lower primary molars as follows:
-
Group A: Bioactive Composite (ACTIVATM KIDS BioACTIv97VE, PulpDent®)
-
Group B: Composite filling (Tetric® n-ceram, Ivoclar Vivadent)
-
Group C: RMGI (GC FUJI® II 2 LC CAPSULE)
Table 1.
The Composition of Restoration Materials
|
Materials
|
Composition
|
Manufacturers
|
| ACTIVATM KIDS |
Blend of diurethane and other methacrylates with modified polyacrylic acid, silica, and amorphous sodium fluoride. |
PulpDent® |
| Composite filling |
Monomer matrix (Bis-MMA, UDMA, Bis-EMA) fillers contain barium glass, ytterbium trifluoride mixed oxide, and copolymers. |
Tetric®n-ceram, Ivoclar vivadent |
| RMGI |
HEMA, UDMA, and polyacrylic acid |
GC FUJI® |
Note. RMGI: Resin-modified glass ionomer.
Procedure
Cavity Preparation
First, the clinician was trained to prepare an ideal cavity before the beginning of sample preparation (Figure 1).
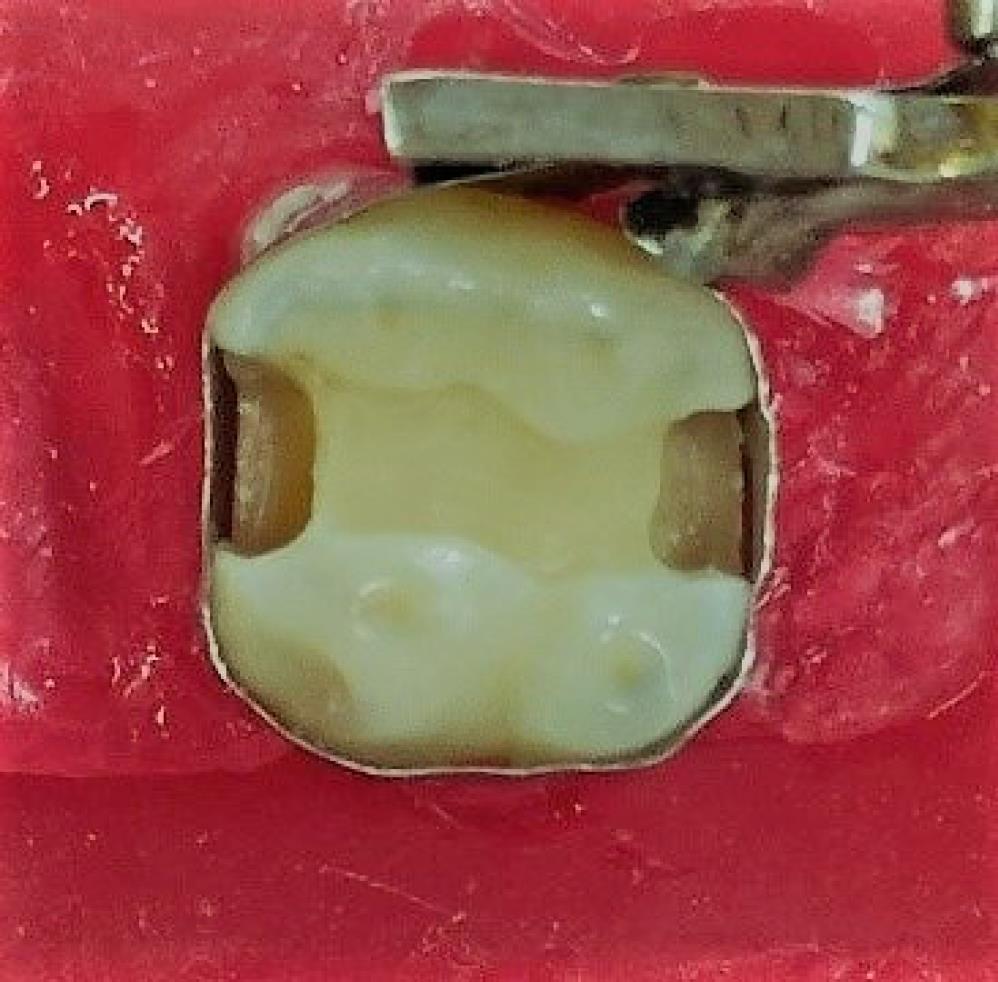
Figure 1.
One of the Experimental Cavities for Identifying the Dimension
.
One of the Experimental Cavities for Identifying the Dimension
All the cavities were prepared using a cylinder bur (Zeffiro; Italy), which was changed every 5 cavities, and a high-speed handpiece (NSK S-Max M800L) with water cooling. One mesial class II cavity was performed according to standardized dimensions as follows:
The occlusal-pulpal depth was set at 1.5 mm, with a buccal-lingual width of 2 mm and a mesial-distal dimension of 1.5 mm. (14-16).
The box cavity: The occlusal-gingival depth was standardized at 3 mm, with a buccal-lingual width of 3 mm and a gingival wall width of 1 mm (14,15).
All the dimensions were measured with a WHO periodontal probe (Zeffiro; Italy). Then, the teeth were rinsed with 5 mL of distilled water and placed in a wax block to receive the restoration materials (13).
Cavities Restoration
Following the adaptation of stainless-steel matrix bands, all the teeth in each group were restored according to the manufacturer’s instructions (Table 2).
Table 2.
The Manufacturers’ Instructions for the Three Restorative Materials
|
Bioactive Composite
|
Composite
|
RMGI
|
- The cavities were rinsed and dried.
- The etchant was applied for 15 seconds on dentine and 30 seconds on enamel.
- The etchant was rinsed for 10 seconds, and tooth surfaces were dried with a cotton pellet.
- The bonding agent (Tetric® n-Bond, Ivoclar Vivadent) was applied, light air-sprayed for 3-5 seconds, and cured with an LED light curing unit (Woodpecker, China).
- The bioactive composite was applied by the bulk-fill technique and light-cured for 20 seconds.
- The restoration was finished with finishing burs and rubber cups. |
- The cavities were rinsed and dried.
- The etchant was applied for 15 seconds on dentine and 30 seconds on enamel.
- The etchant was rinsed for 10 seconds, and tooth surfaces were dried with a cotton pellet.
- A bonding agent was applied, light air-sprayed for 3-5 seconds, and cured with an LED light curing unit (Woodpecker, China).
- The composite was applied incrementally in 5 layers and cured for 20 seconds.
- The restoration was finished with finishing burs and rubber cups. |
- The cavities were rinsed and dried.
- The RMGI capsule was mixed with an amalgam mixer ( ± 4000 cycles) for 10 seconds.
- The mixed capsule was applied to the RMGI applier and injected into the cavity.
- The RMGI was light-cured for 20 seconds.
- The restoration was finished with finishing burs and rubber cups. |
Note. RMGI: Resin-modified glass ionomer.
Thermocycling and Dye Penetration
The restored teeth were subjected to 1000 cycles of alternating thermal cycles between temperatures of 5 °C and 55 °C for one minute in each cycle, with a 5-second transfer time between paths. Then, the apexes and the internal surfaces of the roots were sealed with wax (Figure 2), and the teeth were covered with two layers of nail varnish (1 mm thick) before restoration (Figure 3) (17).

Figure 2.
Sealing the Internal Walls of the Root Using Wax
.
Sealing the Internal Walls of the Root Using Wax

Figure 3.
Painting the Teeth Expect for Restoration by Nail Varnish
.
Painting the Teeth Expect for Restoration by Nail Varnish
All the teeth were immersed in 0.5% methylene blue for 4 hours and then rinsed with distilled water and sectioned mesiodistally to evaluate the degree of dye marginal microleakage. Dye penetration was assessed by two blinded specialized pedodontists using the following scale (Figure 4) (18):
For the occlusal cavity:
-
No dye penetration
-
Dye penetration is up to the first third of the axial wall.
-
Dye penetration is up to the second third of the axial wall.
-
Dye penetration is up to the internal part of the axial wall.
-
Dye penetration includes the pulpal wall.
For the box cavity:
-
No dye penetration
-
Dye penetration is up to the first third of the gingival wall.
-
Dye penetration is up to the second third of the gingival wall.
-
Dye penetration is up to the internal part of the gingival wall.
-
Dye penetration includes the pulpal wall.
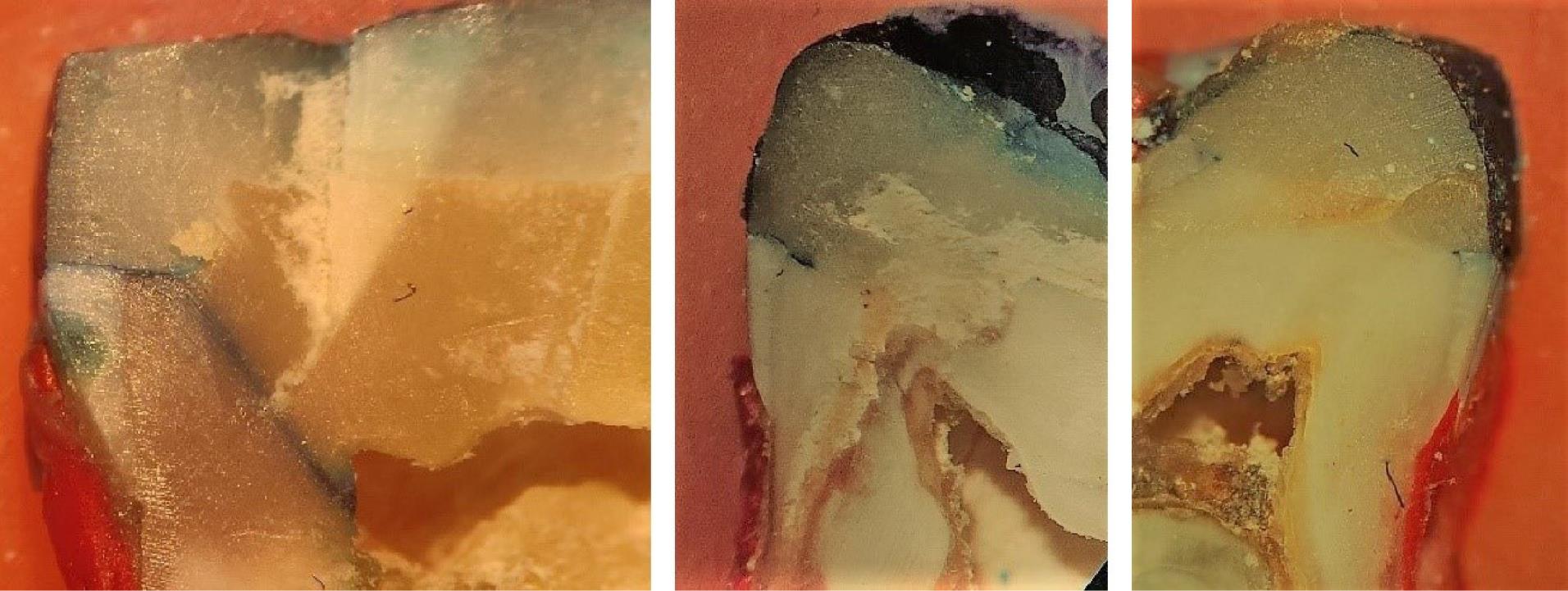
Figure 4.
Dye Penetration in the Occlusal and Gingival Wall for Some Samples
.
Dye Penetration in the Occlusal and Gingival Wall for Some Samples
Statistical Analysis
The data were collected and analyzed using SPSS, version 27. The Kappa coefficient was utilized to evaluate the compatibility between the two operators’ readings, and the results exhibited good consistency (P = 0.000, Table 3). The Kruskal-Wallis test was utilized to compare the mean difference between the three groups. Additionally, the Mann-Whitney U test was employed to compare microleakage between the occlusal and gingival surfaces within each group.
Table 3.
Kappa Coefficient Analysis for Evaluating Compatibility Between the Two Operators
|
Surface
|
Kappa Value
|
T Value
|
P
Value
|
| Occlusal surfaces |
0.914 |
11.796 |
0.000 |
| Gingival surfaces |
0.898 |
8.751 |
0.000 |
Multiple nominal logistic regression was used to evaluate if there was any positive or negative influence of the molar being upper/lower or first/second on the degree of the occlusal/gingival microleakage.
Results
According to the results of the Kruskal-Wallis analysis, no significant difference was found between the three groups (bioactive composite, traditional composite, and RMGI) when comparing microleakage on the occlusal surface (P = 0.104, Table 4). However, descriptive statistics showed that 93.3% of bioactive restoration revealed no dye penetration (degree 1), while the corresponding percentages were 73.3% and 53.3% for composite restoration and RMGI, respectively (Table 5, Figure 5).
Table 4.
Kruskal-Wallis Results of the Microleakage on the Occlusal and Gingival Surface Between Groups
|
Surfaces
|
Restorative Material
|
Number of Samples
|
Mean Ranks
|
Kruskal-Wallis Value
|
P
Value
|
| Occlusal |
Bioactive |
15 |
18.77 |
4.523 |
0.104 |
| composite |
15 |
23.63 |
| RMGI |
15 |
26.60 |
| Gingival |
Bioactive |
15 |
17.87 |
3.671 |
0.160 |
| composite |
15 |
25.10 |
| RMGI |
15 |
26.03 |
Note. RMGI: Resin-modified glass ionomer.
Table 5.
Descriptive Statistic of the Percentages of Dye Penetration of Occlusal and Gingival Surfaces in Each Group
|
Restorative Material
|
Surfaces
|
1 (%)
|
2 (%)
|
3 (%)
|
4 (%)
|
5 (%)
|
| Bioactive |
Occlusal |
93.3 |
0 |
0 |
0 |
6.7 |
| Gingival |
53.3 |
13.3 |
6.7 |
0 |
26.7 |
| Composite |
Occlusal |
73.3 |
6.7 |
0 |
0 |
20 |
| Gingival |
33.3 |
6.7 |
0 |
20 |
40 |
| RMGI |
Occlusal |
53.3 |
40 |
6.7 |
0 |
0 |
| Gingival |
0 |
13.3 |
40 |
33.3 |
13.3 |
Note. RMGI: Resin-modified glass ionomer.
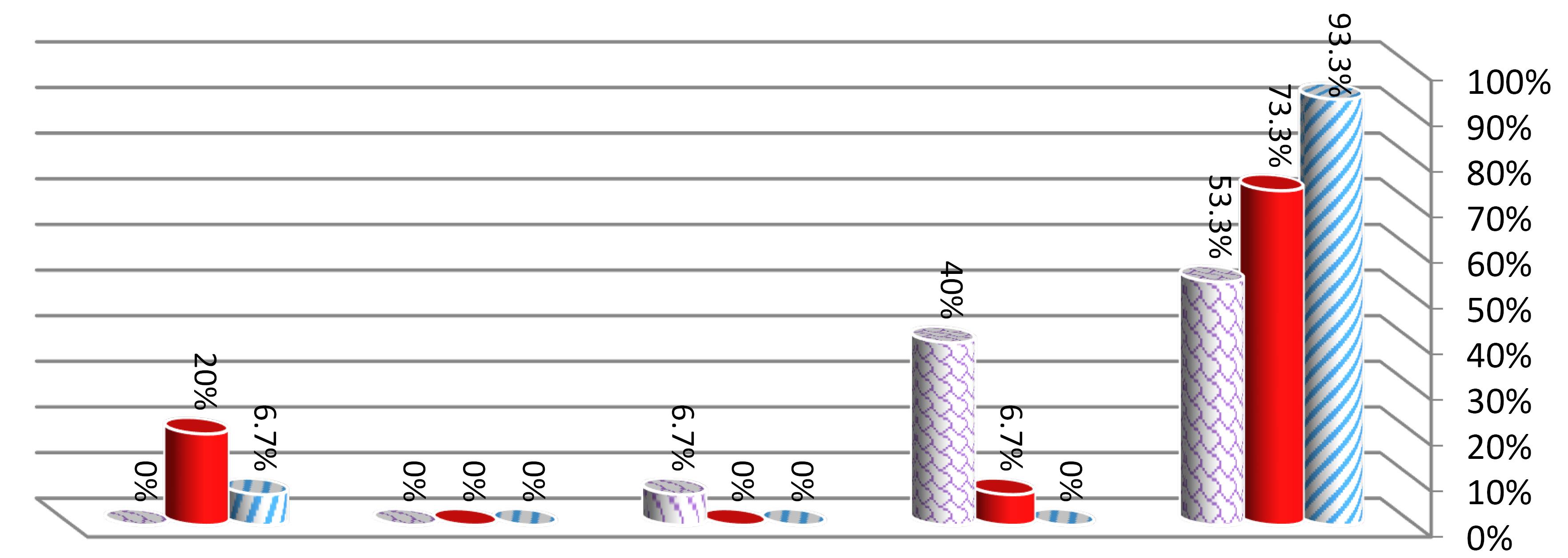
Figure 5.
Descriptive Statistic of Percentage of Occlusal Microleakage for Restorative Materials
.
Descriptive Statistic of Percentage of Occlusal Microleakage for Restorative Materials
In addition, descriptive statistics for gingival microleakage indicated that 53.3% of bioactive restorations demonstrated no dye penetration (degree 1), while the corresponding percentage was 33.3% for composite restorations and 0% for RMGI (Table 5, Figure 6). However, no statistically significant difference was observed between the three groups (bioactive composite, traditional composite, and RMGI) in comparing gingival microleakage (P = 0.160, Table 4).
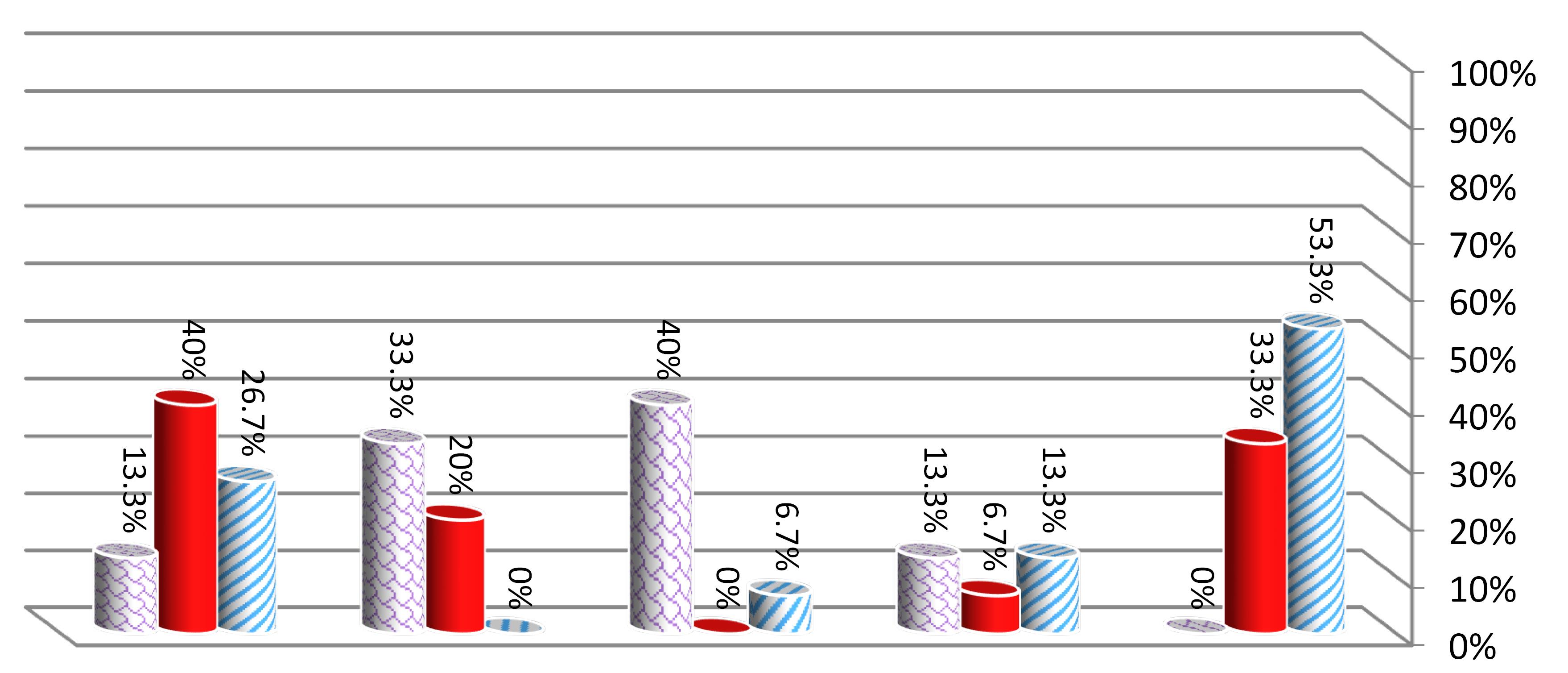
Figure 6.
Descriptive Statistic of Percentage of Gingival Microleakage for Restorative Materials
.
Descriptive Statistic of Percentage of Gingival Microleakage for Restorative Materials
Regarding the comparison between occlusal and gingival microleakage within the same group, the results of the Mann-Whitney U test confirmed a significant difference between the occlusal and gingival surfaces for the three groups (bioactive composite, traditional composite, and RMGI). Thus, the lowest microleakage was in favor of the occlusal surface in each group (P= 0.020, P =0.046, P =0.000, respectively; Table 6).
Table 6.
Mann-Whitney U Analysis for Comparing Microleakage Values Between the Gingival and Occlusal Surface in Each Group
|
Restorative Material
|
Surfaces
|
Number of Samples
|
Mean Ranks
|
Z Value
|
P
Value
|
| Bioactive composite |
Occlusal |
15 |
12.60 |
2.327 |
0.020 |
| Gingival |
15 |
18.40 |
| Conventional composite |
Occlusal |
15 |
12.60 |
1.991 |
0.046 |
| Gingival |
15 |
18.40 |
| RMGI |
Occlusal |
15 |
8.73 |
4.330 |
0.000 |
| Gingival |
15 |
22.27 |
Note. RMGI: Resin-modified glass ionomer.
Multiple nominal logistic regression revealed that the position of the molars (upper/lower) and whether it is first or second have no influence on the occlusal or gingival microleakage (P value > 0.05) as shown in Tables 7, 8.
Table 7.
Multiple Nominal Logistic Regression to Evaluate the Relationship Between the Degree of Occlusal Microleakage and the Position of the Molars
|
Degree of Occlusal Microleakage
|
Factors
|
Estimate
(B)
|
Std. Error
|
Sig.
|
Odd Ratio
Exp (B)
|
| Intercept |
-3.265 |
1.167 |
.005 |
|
| 2 |
Upper/lower |
1.642 |
1.156 |
.156 |
5.166 |
| First/second |
.773 |
.960 |
.420 |
2.167 |
| Intercept |
-21.741 |
1.058 |
.001 |
|
| 3 |
Upper/lower |
19.661 |
.879 |
.392 |
3.456 |
| First/second |
-19.351 |
.995 |
.415 |
3.945 |
| Intercept |
-2.936 |
1.120 |
.009 |
|
| 5 |
Upper/lower |
-.021 |
1.081 |
.985 |
.980 |
| First/second |
1.337 |
1.211 |
.270 |
3.809 |
Note. The reference category is set on the degree (1) of the microleakage scale. No samples were recorded at (4) degree for all materials in occlusal microleakage. Std. error: Standard deviation; Sig. Significance level.
Table 8.
Multiple Nominal Logistic Regression to Evaluate the Relationship Between the Degree of Gingival Microleakage and the Position of Molars
|
Degree of Gingival Microleakage
|
Factors
|
Estimate
(B)
|
Std. Error
|
Sig.
|
Odd Ratio
Exp (B)
|
| Intercept |
-1.766 |
.973 |
.070 |
|
| 2 |
Upper/lower |
.824 |
1.085 |
.448 |
2.279 |
| First/second |
.824 |
1.085 |
.448 |
2.279 |
| Intercept |
-1.686 |
.923 |
.068 |
|
| 3 |
Upper/lower |
1.344 |
1.018 |
.187 |
3.834 |
| First/second |
.676 |
.975 |
.488 |
1.967 |
| Intercept |
-.456 |
.659 |
.489 |
|
| 4 |
Upper/lower |
-.038 |
.928 |
.967 |
.962 |
| First/second |
-.038 |
.928 |
.967 |
.962 |
| Intercept |
-1.025 |
.733 |
.162 |
|
| 5 |
Upper/lower |
1.117 |
.845 |
.186 |
3.055 |
| First/second |
.737 |
.835 |
.377 |
2.091 |
Note. The reference category is set on the degree (1) of the microleakage. Std. error: Standard deviation; Sig. Significance level.
Discussion
Composite restoration has been a cornerstone in dental practice for nearly half a century, continuously evolving to enhance its esthetic and mechanical properties, including wear resistance, radiopacity, and biocompatibility (19). Despite these advancements, it presents clinical challenges such as polymerization shrinkage, marginal microleakage, and handling difficulties, particularly in restoring primary posterior teeth (1). These cases often necessitate patient cooperation and extended treatment sessions, posing a significant hurdle in pediatric dentistry (6,20).
Therefore, RMGI has emerged as a restorative material in primary teeth, which gives an esthetic appearance and releases fluoride; hence, it can be a good alternative for composite and glass ionomer cement, especially in high-risk patients, but its physical and mechanical properties are still debatable (3). Recently, bulk fill bioactive composite has made a revolution in dental materials. It releases and recharges calcium, phosphate, and fluoride and stimulates apatite formation at the material/tooth interface that seals margins against microleakage, which is considered the main failure factor of dental materials. Moreover, it decreases the application time because of its bulk-fill technique (21).
In-vitro microleakage studies provide clinicians with valuable insights into the potential clinical longevity of restoration materials (22). Conducting such a study allows for a better understanding of how these materials may function in real-world conditions, aiding in informed decision-making regarding their use in patient care (23).
First and second, upper and lower primary molars were selected in this study due to their ease of collection during orthodontic serial extraction procedures, and their larger size could facilitate the preparation of ideal class II cavities (11). Overall, 1000 thermal cycles were performed on the restored teeth to mimic the changes in the oral cavity within one year. Dye penetration was chosen to evaluate marginal microleakage since it is a simple, non-toxic, effective, available, and economical method (24).
The bulk-fill bioactive composite demonstrated the least occlusal and gingival microleakage, potentially attributed to apatite formation at the material-tooth interface, a mechanism likely sealing gaps induced by polymerization shrinkage. This observation is consistent with the findings reported by Adeyeye et al, Pangabdian et al, and Jain et al, suggesting promising outcomes for bioactive composites that recorded smaller amounts of microleakage (21,25,26).
However, our results do not match those of Neves et al, indicating that the bioactive composite has a higher degree of microleakage compared with the traditional composite; this may be because the restorations were class V and on permanent molars, and the radioactive isotope was the diagnostic method(4). In addition, our findings contradict the results of artínez-Sabio et al, demonstrating that their bioactive restorations recorded a higher degree of microleakage, which may be attributed to the difference in the methodology as they immersed the samples in 0.5% methylene blue for 8 weeks without thermocycling (27).
A significant difference was observed between occlusal and gingival microleakage in groups (A), (B), and (C). The lowest values were related to the occlusal surface; this may be due to difficulties in sealing between the restoration material and gingival surface and a decrease in the bonding with enamel at the gingival wall; thus, the enamel thickness at the cementoenamel junction was at its lowest(28). However, for the bioactive composite, it may be due to the bulk-fill technique. Nonetheless, the thickness of the restorative material (occlusal-gingival 3 mm) does not allow for the good penetration of the curing light from the occlusal to the gingival sides (12,29).
Finally, there was no difference in occlusal or gingival microleakage between the teeth being the first or second and being extracted from the upper or lower jaw. This may be due to the absence of clinical factors that affect the results, such as isolation, the child’s cooperation, mechanical forces, and caries risk. Therefore, in clinical studies, the microleakage may differ according to the position of the teeth.
Limitations of the Study
Our study had some limitations. It was an in-vitro experimental study with a small sample size; thus, many factors that could affect the results were successfully excluded, including saliva and blood contamination, failure in achieving an ideal isolation in some in-oral cavities, difficulties in instruments in some cases, and the impossibility of unifying the dimension in clinical practice. Furthermore, more accurate diagnostic methods, such as scanning electron microscopy, bacterial infiltration, and radioactive isotopes, can be used in other studies to support or refute our results.
Conclusion
Within the limitations of the study, it was concluded that marginal microleakage values on occlusal and gingival surfaces were the lowest in the bulk-fill bioactive composite with no significant difference in comparison with the conventional composite and RMGI. Further, in-vitro investigations and long-term clinical studies utilizing alternative evaluation methods, such as scanning electron microscopy, are necessary to corroborate these findings.
Acknowledgments
This study was performed at the Faculty of Dentistry, Damascus University, Syria, which deserves a great appreciation for academic and financial support. The authors would also like to thank Dr. Salma AL-Nesser for writing assistance and critical reading for the article.
Competing Interests
The authors declared no potential conflict of interests.
Ethical Approval
Ethical approval for the study was obtained from the Ethics Committee of Damascus University (Decision No. 2327).
Funding
Damascus University funded the research.
References
- Chisini LA, Collares K, Cademartori MG, de Oliveira LJ, Conde MC, Demarco FF. Restorations in primary teeth: a systematic review on survival and reasons for failures. Int J Paediatr Dent 2018; 28(2):123-39. doi: 10.1111/ipd.12346 [Crossref] [ Google Scholar]
- American Academy on Pediatric Dentistry Clinical Affairs Committee-Restorative Dentistry Subcommittee; American Academy on Pediatric Dentistry Council on Clinical Affairs. Guideline on pediatric restorative dentistry. Pediatr Dent. 2008;30(7 Suppl):163-9.
- Leal SC, Takeshita EM. Pediatric Restorative Dentistry. Springer; 2019. doi: 10.1007/978-3-319-93426-6.
- Neves P, Pires S, Marto CM, Amaro I, Coelho A, Sousa J. Evaluation of microleakage of a new bioactive material for restoration of posterior teeth: an in vitro radioactive model. Appl Sci 2022; 12(22):11827. doi: 10.3390/app122211827 [Crossref] [ Google Scholar]
- Carrilho E, Abrantes M, Paula A, Casalta-Lopes J, Botelho M, Ferreira M. Microleakage study of a restorative material via radioisotope methods. Rev Port Estomatol Med Dent Cir Maxilofac 2014; 55(3):129-34. doi: 10.1016/j.rpemd.2014.08.005 [Crossref] [ Google Scholar]
- Frankenberger R, Dudek MC, Winter J, Braun A, Krämer N, von Stein-Lausnitz M. Amalgam alternatives critically evaluated: effect of long-term thermomechanical loading on marginal quality, wear, and fracture behavior. J Adhes Dent 2020; 22(1):107-16. doi: 10.3290/j.jad.a44001 [Crossref] [ Google Scholar]
- Sidhu SK, Nicholson JW. A review of glass-ionomer cements for clinical dentistry. J Funct Biomater 2016; 7(3):16. doi: 10.3390/jfb7030016 [Crossref] [ Google Scholar]
- Sajini SI, Alshawi BA, Alharbi LM. Assessment of remineralisation potentials of bioactive dental composite using an in-vitro demineralised dentine model. J Taibah Univ Med Sci 2022; 17(4):640-7. doi: 10.1016/j.jtumed.2021.12.004 [Crossref] [ Google Scholar]
- Van Ende A, De Munck J, Lise DP, Van Meerbeek B. Bulk-fill composites: a review of the current literature. J Adhes Dent 2017; 19(2):95-109. doi: 10.3290/j.jad.a38141 [Crossref] [ Google Scholar]
- Krithikadatta J, Gopikrishna V, Datta M. CRIS guidelines (checklist for reporting in-vitro studies): a concept note on the need for standardized guidelines for improving quality and transparency in reporting in-vitro studies in experimental dental research. J Conserv Dent 2014; 17(4):301-4. doi: 10.4103/0972-0707.136338 [Crossref] [ Google Scholar]
- Adi A, Altinawi MK. Marginal microleakage evaluation of class II bulk-fill composite restorations in primary molars–in vitro study. J Stomatol 2020; 73(2):74-80. doi: 10.5114/jos.2020.96164 [Crossref] [ Google Scholar]
- Somani R, Som NK, Jaidka S, Hussain S. Comparative evaluation of microleakage in various placement techniques of composite restoration: an in vitro study. Int J Clin Pediatr Dent 2020; 13(3):264-8. doi: 10.5005/jp-journals-10005-1764 [Crossref] [ Google Scholar]
- Sudhapalli SK, Sudhapalli S, Razdan RA, Singh V, Bhasin A. A comparative evaluation of microleakage among newer composite materials: an in vitro study. Contemp Clin Dent 2018; 9(4):587-91. doi: 10.4103/ccd.ccd_621_18 [Crossref] [ Google Scholar]
- Jokstad A. Class 2 Cavity Preparations and Restoration Performance. University of Oslo, Dental Faculty, Department of Anatomy and NIOM, Scandinavian Institute of Dental Materials; 1992.
- Zwain AM. Cavity Preparation Incipient Class I Cavity 1992;29(4):1-5.
- Oldenburg TR, Vann WF Jr, Dilley DC. Composite restorations for primary molars: results after four years. Pediatr Dent 1987; 9(2):136-43. [ Google Scholar]
- Punathil S, Almalki SA, Aljameel AH, Gowdar IM, Vijay Amarnath MC, Chinnari K. Assessment of microleakage using dye penetration method in primary teeth restored with tooth-colored materials: an in vitro study. J Contemp Dent Pract 2019; 20(7):778-82. doi: 10.5005/jp-journals-10024-2596 [Crossref] [ Google Scholar]
- Popoff DA, Gonçalves FS, Magalhães CS, Moreira AN, Ferreira RC, Mjör IA. Repair of amalgam restorations with composite resin and bonded amalgam: a microleakage study. Indian J Dent Res 2011; 22(6):799-803. doi: 10.4103/0970-9290.94672 [Crossref] [ Google Scholar]
- Cavalheiro CP, de Souza PS, de Oliveira Rocha R, Mendes FM, Braga MM, Raggio DP. Choosing the criteria for clinical evaluation of composite restorations: an analysis of impact on reliabilty and treatment decision. Pesqui Bras Odontopediatria Clin Integr 2020; 20:e5088. doi: 10.1590/pboci.2020.055 [Crossref] [ Google Scholar]
- Bhati S, Panwar S, Gurav R. Composites and its applications: a review. Compliance Engineering Journal 2020; 11(9):273-81. doi: 10.2139/ssrn.3904471 [Crossref] [ Google Scholar]
- Adeyeye A, Spivey V, Stoeckel D, Welch D. Comparison of the marginal microleakage of a bioactive composite resin and traditional dental restorative materials. Gen Dent 2023; 71(3):52-6. [ Google Scholar]
- Kidd EA. Microleakage: a review. J Dent 1976; 4(5):199-206. doi: 10.1016/0300-5712(76)90048-8 [Crossref] [ Google Scholar]
- Kaisarly D, Gezawi ME. Polymerization shrinkage assessment of dental resin composites: a literature review. Odontology 2016; 104(3):257-70. doi: 10.1007/s10266-016-0264-3 [Crossref] [ Google Scholar]
- Déjou J, Sindres V, Camps J. Influence of criteria on the results of in vitro evaluation of microleakage. Dent Mater 1996; 12(6):342-9. doi: 10.1016/s0109-5641(96)80044-3 [Crossref] [ Google Scholar]
- Pangabdian F, Wijaya YH, Widyanita DA. The comparison of microleakage between bioactive composite resin and compomer. Denta Jurnal Kedokteran Gig 2021; 15(2):86-91. doi: 10.30649/denta.v15i2.5 [Crossref] [ Google Scholar]
- Jain K, Katge F, Poojari M, Shetty S, Patil D, Ghadge S. Comparative evaluation of microleakage of bioactive, ormocer, and conventional GIC restorative materials in primary molars: an in vitro study microleakage of three restorative materials. Int J Dent 2022; 2022:7932930. doi: 10.1155/2022/7932930 [Crossref] [ Google Scholar]
- Martínez-Sabio L, Peñate L, Arregui M, Veloso Duran A, Blanco JR, Guinot F. Comparison of shear bond strength and microleakage between activaTM bioactive restorativeTM and bulk-fill composites-an in vitro study. Polymers (Basel) 2023; 15(13):2840. doi: 10.3390/polym15132840 [Crossref] [ Google Scholar]
- de Menezes Oliveira MA, Torres CP, Gomes‐Silva JM, Chinelatti MA, de Menezes FC, Palma‐Dibb RG. Microstructure and mineral composition of dental enamel of permanent and deciduous teeth. Microsc Res Tech 2010; 73(5):572-7. doi: 10.1002/jemt.20796 [Crossref] [ Google Scholar]
- Misilli U, Yılmaz F. Evaluation of marginal microleakage in composite restorations with different placement techniques. Int Dent Res 2018; 8(2):70-7. doi: 10.5577/intdentres.2018.vol8.no2.4 [Crossref] [ Google Scholar]