Avicenna J Dent Res. 16(1):22-27.
doi: 10.34172/ajdr.1771
Original Article
Attractiveness of Modified Photographs of Class II, Division I Patients as Judged by Laypeople and Orthodontists
Hanieh Jalili Khradmand 1  , Maryam Salehzadeh 2 , Vahid Mollabashi 3, Homa Farhadifard 3, * , Maryam Farhadian 4
, Maryam Salehzadeh 2 , Vahid Mollabashi 3, Homa Farhadifard 3, * , Maryam Farhadian 4
Author information:
1Private Practice
2Department of Orthodontics, Tabriz University of Medical Sciences, Tabriz, Iran
3Department of Orthodontics, Hamadan University of Medical Sciences, Hamadan, Iran
4Department of Epidemiology, Hamadan University of Medical Sciences, Hamadan, Iran
Abstract
Background: There are two treatment alternatives that are commonly proposed to class II, division I patients, including camouflage and orthognathic surgeries.
Methods: The original profile photos of two male and two female patients were altered with Photoshop in order to simulate camouflage and surgical treatment. This was performed by increasing the nasolabial angle by 4 mm, 8 mm, and 12 mm and extending the chin-neck length by 3 mm, 6 mm, and 9 mm. The initial and actual final photos of the patient, along with the six modified pictures, were presented to the participants. They reordered the pictures from the most aesthetic to the least aesthetic.
Results: Overall, 30 orthodontists and 140 laypeople completed the task. Orthodontists perceived surgical treatment as more attractive compared to laypeople. The highest rank was assigned to post-treatment photographs of the patients, while the lowest rank was given to pre-treatment photographs.
Conclusion: Class II treatment adds to profile attractiveness as judged by laypeople and orthodontists. There are some differences in opinions between these groups.
Keywords: Laypeople, Profile attractiveness, Malocclusion angle class II, Esthetics dental
Copyright and License Information
© 2024 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Jalili Khradmand H, Salehzadeh M, Mollabashi V, Farhadifard H, Farhadian M. Attractiveness of modified photographs of class II, division I patients as judged by laypeople and orthodontists. Avicenna J Dent Res. 2024; 16(1):22-27. doi:10.34172/ajdr.1771
Background
The face is the center of attention, and it is believed that people with more attractive faces are more socially accepted and adored. They are also regarded as more intelligent and are more successful in job interviews (1,2). Skeletal malocclusion, defined as a disproportion between jaw position or size, negatively affects facial attractiveness, and this is the main reason people seek orthodontic treatment (3).
Class II, division I malocclusion, characterized by a large overjet, is one of the more prevalent subgroups witnessed in society. Some common facial features are reduced chin projection, retruded lower lip, convex profile, and short chin-neck length, which could impair facial beauty (4).
Two main treatment options are considered for class II, div I malocclusions; they are orthodontic camouflage by the extraction of two maxillary premolars, which might alter the nasolabial angle and upper lip position, as well as orthognathic surgery, which repositions jaws to achieve facial harmony. Mandibular advancement is the main surgical procedure performed, and this surgery often increases chin-neck length. All treatment modalities aim to enhance facial esthetics and affect profile, teeth, chin position, and lip posture (5).
There is no consensus on the best treatment alternative for class II, division I patients that will bring the best esthetic results. Esthetic perception is a subjective concept; thus, we decided to survey and compare the profile attractiveness of these treatment modalities. To the best of our knowledge, few studies have investigated this topic.
Methods
For this study, we modified the initial photographs of two male and two female patients who all had class II, division I malocclusion, with normal facial height and Frankfort–mandibular plane angle. Patients who had a history of rhinoplasty or other cosmetic procedures on affected areas and those with severe mandibular deficiency were excluded from the investigation. The samples were treated with either camouflage or orthognathic surgery. All image alterations were performed by Adobe Photoshop 22.0 on the original profile photographs of patients.
To simulate mandibular advancement, the chin-neck length, measured on patients’ cephalograms, was increased by 3 mm, 6 mm, and 9 mm.
To create camouflage simulations, the measured nasolabial angle was increased by four, eight, and 12 degrees.
All altered images (N = 6) were finalized and prepared for presentation, along with initial and final orthodontic photographs (Figures 1‒4).
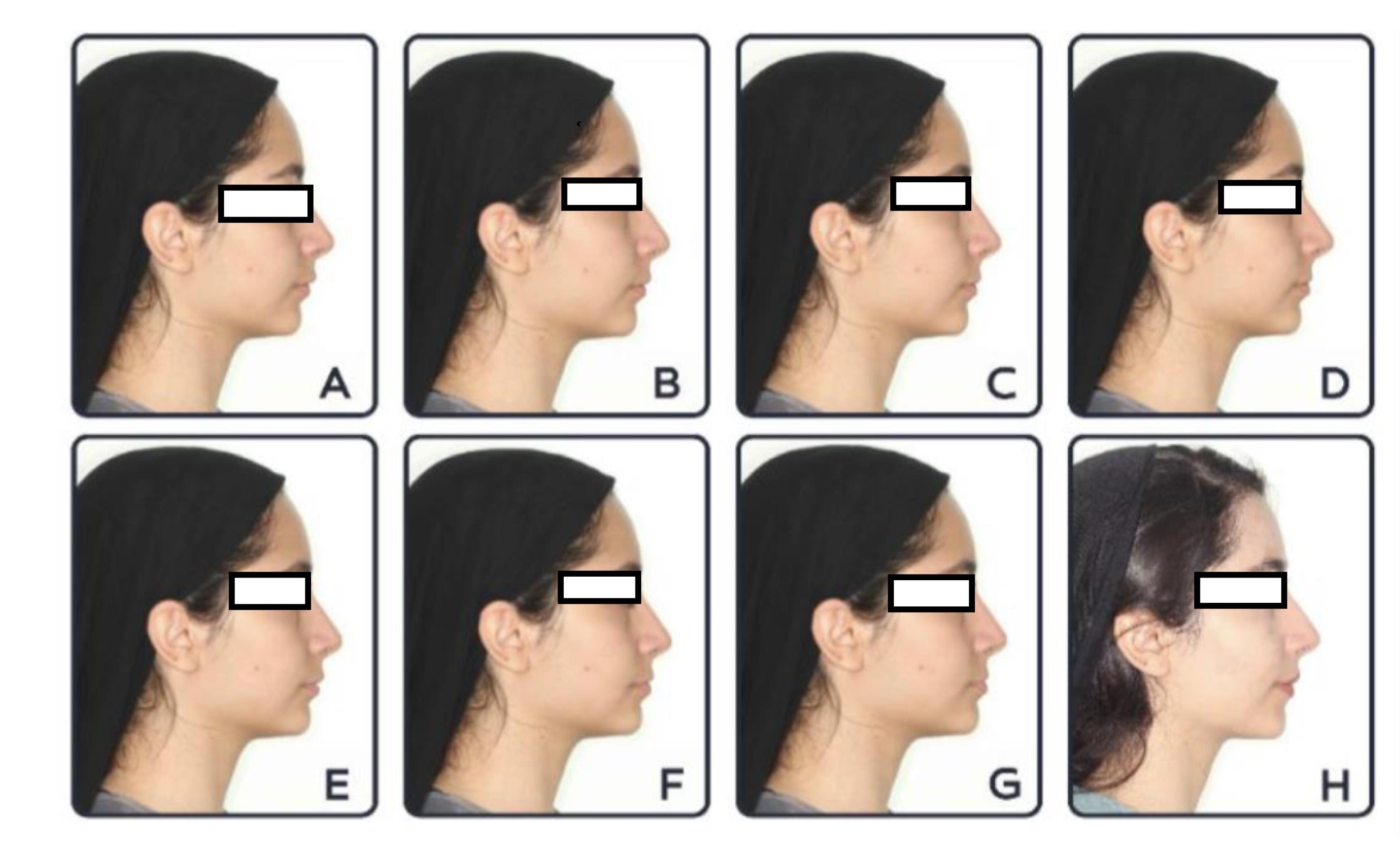
Figure 1.
Original Initial (A), Modified (B-G), and Original Final Photographs of Patient 1 [B: Nasolabial Angle Increased by 4 Degrees, C: Nasolabial Angle Increased by 8 Degrees, D: Nasolabial Angle Increased by 12 Degrees, E: Chin-neck Length Increased by 3 mm, F: Chin-neck Length Increased by 6 mm, and G: Chin-neck Length Increased by 9 mm]
.
Original Initial (A), Modified (B-G), and Original Final Photographs of Patient 1 [B: Nasolabial Angle Increased by 4 Degrees, C: Nasolabial Angle Increased by 8 Degrees, D: Nasolabial Angle Increased by 12 Degrees, E: Chin-neck Length Increased by 3 mm, F: Chin-neck Length Increased by 6 mm, and G: Chin-neck Length Increased by 9 mm]
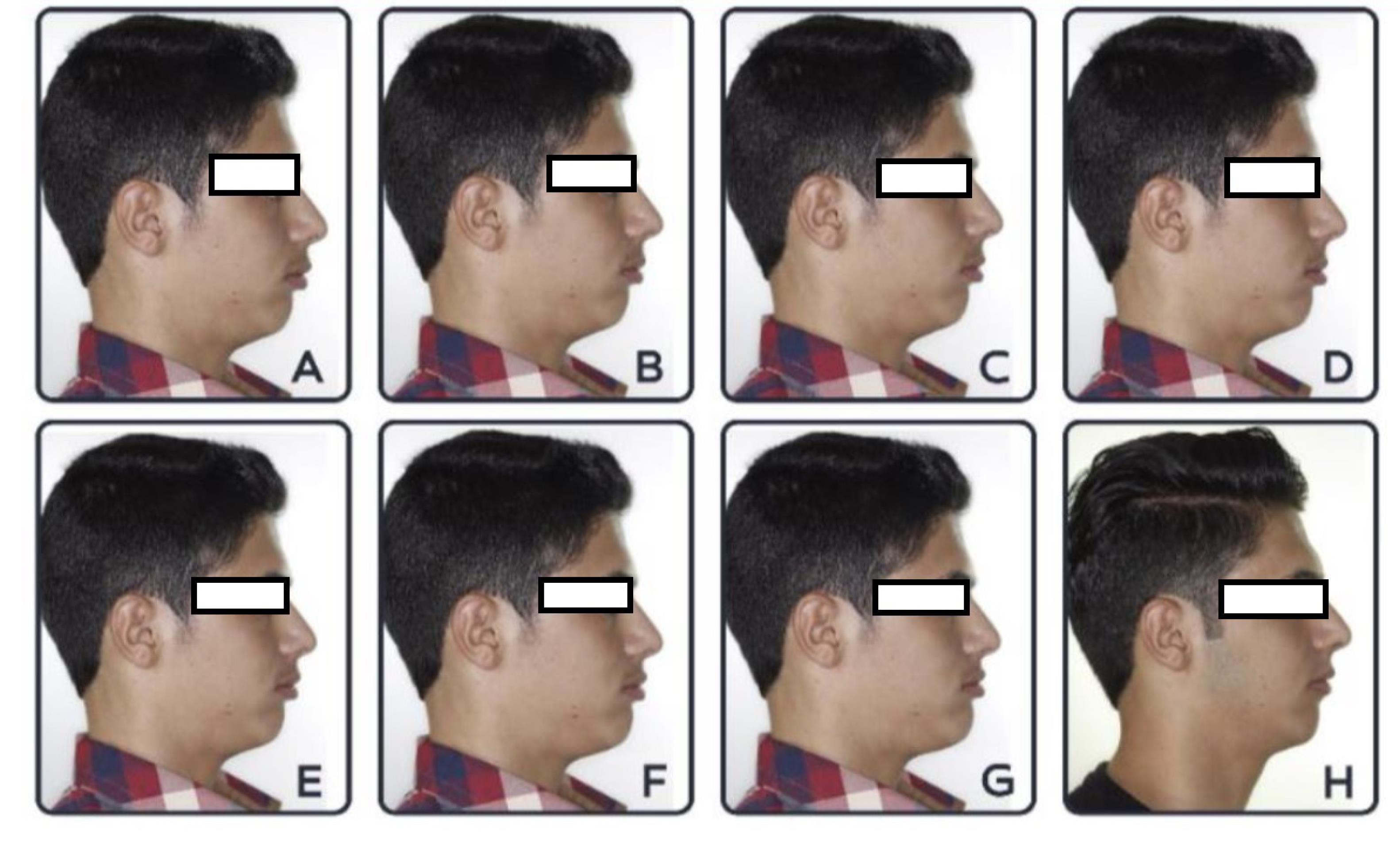
Figure 2.
Original Initial (A), Modified (B-G), and Original Final Photographs of Patient 2 [B: Nasolabial Angle Increased by 4 Degrees, C: Nasolabial Angle Increased by 8 Degrees, D: Nasolabial Angle Increased by 12 Degrees, E: Chin-neck Length Increased by 3 mm, F: Chin-neck Length Increased by 6 mm, and G: Chin-neck Length Increased by 9 mm]
.
Original Initial (A), Modified (B-G), and Original Final Photographs of Patient 2 [B: Nasolabial Angle Increased by 4 Degrees, C: Nasolabial Angle Increased by 8 Degrees, D: Nasolabial Angle Increased by 12 Degrees, E: Chin-neck Length Increased by 3 mm, F: Chin-neck Length Increased by 6 mm, and G: Chin-neck Length Increased by 9 mm]

Figure 3.
Original Initial (A), Modified (B-G), and Original Final Photographs of Patient 3 [B: Nasolabial Angle Increased by 4 Degrees, C: Nasolabial Angle Increased by 8 Degrees, D: Nasolabial Angle Increased by 12 Degrees, E: Chin-neck Length Increased by 3 mm, F: Chin-neck Length Increased by 6 mm, and G: Chin-neck Length Increased by 9 mm]
.
Original Initial (A), Modified (B-G), and Original Final Photographs of Patient 3 [B: Nasolabial Angle Increased by 4 Degrees, C: Nasolabial Angle Increased by 8 Degrees, D: Nasolabial Angle Increased by 12 Degrees, E: Chin-neck Length Increased by 3 mm, F: Chin-neck Length Increased by 6 mm, and G: Chin-neck Length Increased by 9 mm]
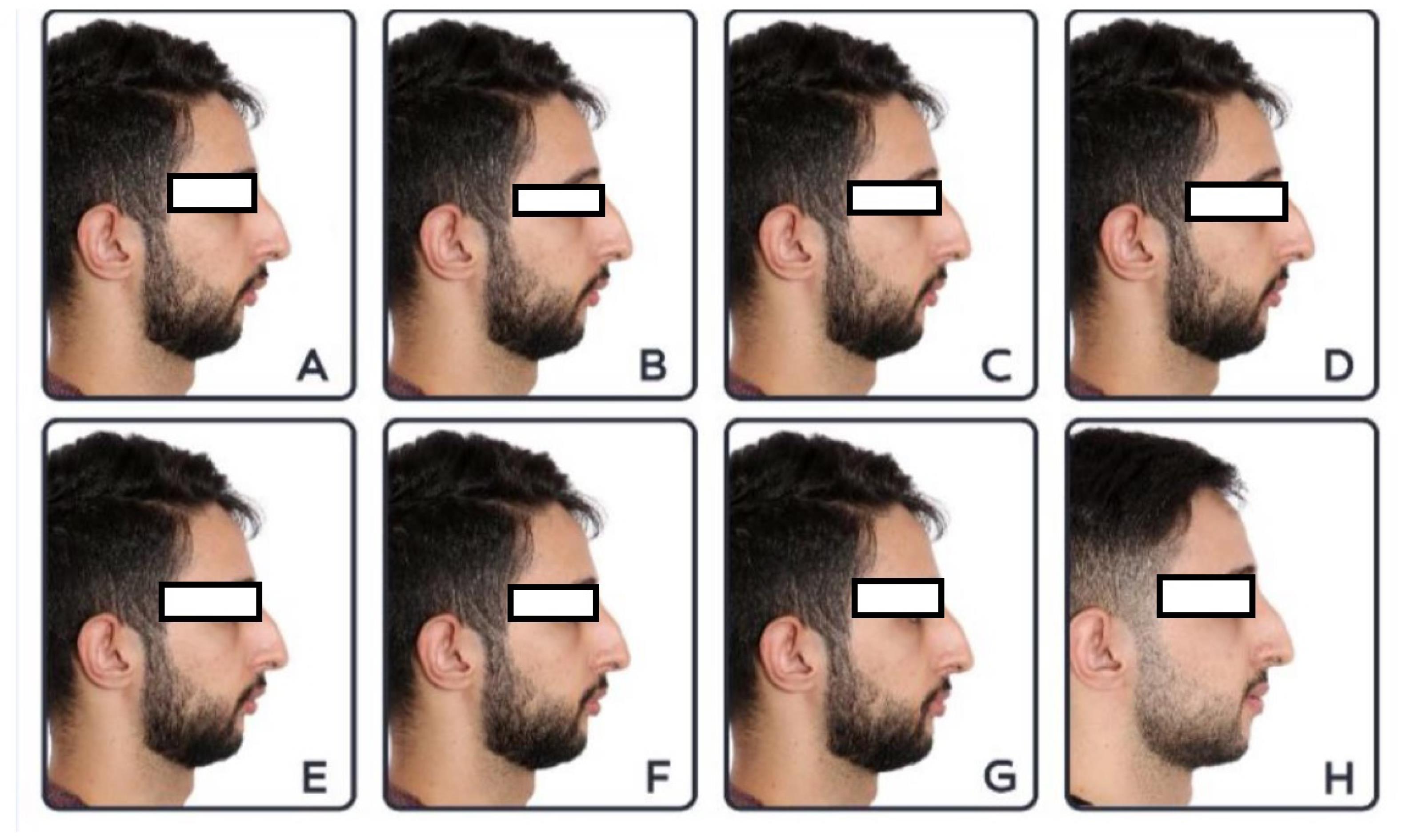
Figure 4.
Original Initial (A), Modified (B-G), and Original Final Photographs of Patient 4 [B: Nasolabial Angle Increased by 4 Degrees, C: Nasolabial Angle Increased by 8 Degrees, D: Nasolabial Angle Increased by 12 Degrees, E: Chin-neck Length Increased by 3 mm, F: Chin-neck Length Increased by 6 mm, and G: Chin-neck Length Increased by 9 mm]
.
Original Initial (A), Modified (B-G), and Original Final Photographs of Patient 4 [B: Nasolabial Angle Increased by 4 Degrees, C: Nasolabial Angle Increased by 8 Degrees, D: Nasolabial Angle Increased by 12 Degrees, E: Chin-neck Length Increased by 3 mm, F: Chin-neck Length Increased by 6 mm, and G: Chin-neck Length Increased by 9 mm]
An online questionnaire was regulated and uploaded, including five tabs. The first tab collected data about the age, gender, and profession of the electorate. The four remaining tabs, each consisting of eight profile photos of the patients, namely, the original initial photograph, six modified, and one final result of the actual treatment performed for the patient, requested the respondents to rank profile photos from most attractive to least attractive.
The respondents were either 18‒60-year-old orthodontists or laypeople with academic degrees not associated with the dental profession.
To detect a 0.2 difference between orthodontists and laypeople’s responses, considering a power of 90%, at least 140 laypeople and 30 orthodontists had to complete the questionnaires.
The data were analyzed with SPSS software, version 22.0. Chi-square, Kruskal-Wallis, Mann–Whitney, and Freidman tests were employed, and a significance level was kept at 0.05.
Results
A total of 140 laypeople and 30 orthodontists participated in this study. Their age ranged from 18 to 62, and their mean age was 30 years old.
For the first patient, laypeople considered profile H as the most attractive one, while orthodontists preferred profile F. Both groups scored A as the least attractive profile. Table 1 summarizes the mean score of each profile for patient 1.
Table 1.
Mean Ranks Assigned by Two Groups to Photo Set 1
|
|
Group
|
Mean Rank±SD
|
P
Value
|
| 1A |
Laypeople |
3.78 ± 2.43 |
0.119 |
| Orthodontists |
2.97 ± 1.87 |
| 1B |
Laypeople |
4.18 ± 1.97 |
0.509 |
| Orthodontists |
3.90 ± 1.75 |
| 1C |
Laypeople |
4.23 ± 1.98 |
0.582 |
| Orthodontists |
3.97 ± 1.56 |
| 1D |
Laypeople |
4.18 ± 2.01 |
0.328 |
| Orthodontists |
3.77 ± 2.10 |
| 1E |
Laypeople |
4.62 ± 1.69 |
0.008 |
| Orthodontists |
5.55 ± 1.67 |
| 1F |
Laypeople |
4.44 ± 1.98 |
0.000 |
| Orthodontists |
5.94 ± 2.30 |
| 1G |
Laypeople |
4.01 ± 2.50 |
0.042 |
| Orthodontists |
5.06 ± 2.82 |
| 1H |
Laypeople |
6.55 ± 2.45 |
0.000 |
| Orthodontists |
4.84 ± 2.54 |
Note. SD: Standard deviation.u
There was a significant difference between laypeople and orthodontists’ scores for profiles E, F, G, and H.
For patient two, laypeople judged H as the most attractive, and orthodontists chose G. Both groups judged A as the least attractive (Table 2). Orthodontists significantly assigned higher and lower scores to surgical treatments (F and G) and camouflage (B and H), respectively.
Table 2.
Mean Ranks Assigned by Two Groups to Photo Set 2
|
|
Group
|
Mean Rank±SD
|
P
Value
|
| 2A |
Laypeople |
3.00 ± 2.43 |
0.102 |
| Orthodontists |
1.97 ± 1.44 |
| 2B |
Laypeople |
3.44 ± 1.85 |
0.014 |
| Orthodontists |
2.52 ± 1.23 |
| 2C |
Laypeople |
3.76 ± 1.55 |
0.482 |
| Orthodontists |
3.48 ± 1.38 |
| 2D |
Laypeople |
4.08 ± 1.55 |
0.628 |
| Orthodontists |
4.23 ± 1.35 |
| 2E |
Laypeople |
4.70 ± 1.80 |
0.697 |
| Orthodontists |
4.81 ± 1.57 |
| 2F |
Laypeople |
4.94 ± 1.89 |
0.000 |
| Orthodontists |
6.16 ± 1.55 |
| 2G |
Laypeople |
5.16 ± 2.40 |
0.000 |
| Orthodontists |
6.61 ± 1.82 |
| 2H |
Laypeople |
6.97 ± 2.13 |
0.014 |
| Orthodontists |
6.16 ± 2.35 |
Note. SD: Standard deviation.
For the first and second patients, for whom camouflage treatment was completed, the simulated profile of the camouflage treatment was ranked lower in comparison to the actual result of treatment (H).
Reviewing the scores for the third patient, it was revealed that both groups judged H as the most attractive profile and A as the least attractive one (Table 3). For profiles A, B, F, and G, the scores of the two groups differed significantly. Orthodontists preferred G and H and assigned lower scores to A and B.
Table 3.
Mean Ranks Assigned by Two Groups to Photo Set 3
|
|
Group
|
Mean Rank±SD
|
P
Value
|
| 3A |
Laypeople |
2.52 ± 2.18 |
0.004 |
| Orthodontists |
1.29 ± 6.93 |
| 3B |
Laypeople |
3.23 ± 1.84 |
0.024 |
| Orthodontists |
2.29 ± 6.43 |
| 3C |
Laypeople |
3.80 ± 1.55 |
0.083 |
| Orthodontists |
3.32 ± 1.04 |
| 3D |
Laypeople |
4.28 ± 1.75 |
0.456 |
| Orthodontists |
4.35 ± 1.17 |
| 3E |
Laypeople |
4.16 ± 1.55 |
0.761 |
| Orthodontists |
4.29 ± 1.29 |
| 3F |
Laypeople |
5.21 ± 1.69 |
0.005 |
| Orthodontists |
6.16 ± .79 |
| 3G |
Laypeople |
5.46 ± 2.21 |
0.001 |
| Orthodontists |
6.71 ± 1.52 |
| 3H |
Laypeople |
7.28 ± 1.76 |
0.360 |
| Orthodontists |
7.55 ± .723 |
Note. SD: Standard deviation.
Based on the results (Table 4), for both groups, the highest and lowest scores were assigned to profiles H and A, respectively. There was a significant difference between the two groups for profiles A, B, G, and F, as laypeople judged A and B more attractive and G and F less attractive compared to the orthodontists.
Table 4.
Mean Ranks Assigned by Two Groups to Photo Set 4
|
|
Group
|
Mean Rank±SD
|
P
Value
|
| 4A |
Laypeople |
2.55 ± 2.33 |
0.102 |
| Orthodontists |
1.39 ± .98 |
| 4B |
Laypeople |
3.48 ± .1.77 |
0.014 |
| Orthodontists |
2.16 ± .53 |
| 4C |
Laypeople |
3.70 ± 1.57 |
0.482 |
| Orthodontists |
3.16 ± .96 |
| 4D |
Laypeople |
4.18 ± 1.52 |
0.628 |
| Orthodontists |
3.94 ± 1.18 |
| 4E |
Laypeople |
4.40 ± 1.59 |
0.697 |
| Orthodontists |
4.58 ± .92 |
| 4F |
Laypeople |
5.17 ± 1.72 |
0.000 |
| Orthodontists |
5.94 ± .68 |
| 4G |
Laypeople |
5.40 ± 2.29 |
0.000 |
| Orthodontists |
7.06 ± .51 |
| 4H |
Laypeople |
7.06 ± 2.12 |
0.014 |
| Orthodontists |
7.77 ± .56 |
Note. SD: Standard deviation.
For the third and fourth patients who underwent surgical advancement of the mandible, the final treatment outcome was shown to be more attractive than the predicted surgical results.
Discussion
Enhanced esthetics is the main reason people seek orthodontic treatment (2). The ideal of beauty is defined by culture, fashion, and media (6). There is a continuous need to assess the esthetic impact of facial characteristics that are affected during orthodontic treatment alternatives and more attractive facial traits; otherwise, patients may be dissatisfied with the result of their treatment even though function has improved (7), which is considered a failure. The current study compared the esthetic results of the two treatment alternatives for adult class II, Div. I patients and assessed the impacts of different amounts of mandibular advancement, incisor retraction, and nasolabial angle increase. The profile photographs were modified, and the patient’s profile was simulated for different treatments. In addition, the assessors were asked to rank the profile photographs from most to least attractive. In contrast to some studies (8,9), in this study, profile photographs of female and male patients were simultaneously used, and thus it was possible to find out whether gender affects the esthetic results.
In line with several studies (10,11), the findings of our study demonstrated that laypeople and orthodontists both prefer treatment over no treatment; this was true regardless of the gender and actual treatment of the patients.
An interesting finding in this study was that, in all cases, the actual treatment performed on the patient was more attractive than the predicted profile photographs of possible treatments. This is because real-life profile photographs are more appealing than pictures of artificial alterations made by software. Further, the final photograph of patients was taken for a minimum of 2 years after the first photographs; this elucidates the finding that there is soft tissue improvement with growth with time, increasing the effect of the treatment (12).
Laypeople rated surgical treatment in the second, which is in line with the results of other studies that reported that increasing the chin-neck length is more attractive than increasing the nasolabial angle, which indicates camouflage (13).
As orthodontic literature is replete with the concept of an ideal straight profile, orthodontists also prefer surgical treatment, which is consistent with the results of a study that concludes orthodontists rate profiles with a protrusive mandible as highly attractive (14). The preferred amount of mandibular advancement was 9 mm for 3 patients, which conforms to the findings of Kalin et al (10) and Yüksel et al (13). In contrast, 6 mm was preferred for one of the patients, which corroborates the results of Imani et al (14).
Regarding the nasolabial angle change in camouflage treatment, there is controversial evidence. In the study by Imani et al (14), increasing the angle could proportionally add to profile attractiveness. In our study, in three cases, increasing the angle by 12 degrees was considered the most attractive, while in one case, in a female patient with extraction treatment, an eight-degree increase was more attractive than four and twelve degrees, which matches the results of the study by Taghavi et al (15).
For the two patients with mandibular advancement, both groups agreed that increasing the nasolabial angle enhanced profile esthetics, and increasing the amount of advancement was associated with higher esthetic ranks. In addition, 9-mm advancement was judged the most appreciated profile, and, similar to the study by Rocha et al, orthodontists assigned higher ranks to surgical treatment (9).
There was a difference in esthetic scores between male and female patients, and both assessors preferred 9-mm advancement and a 12-degree increase in the nasolabial angle for the male patient, while for the female patient, orthodontists considered 6-mm advancement the most esthetic change, and laypeople preferred a 3-mm advancement.
Conclusion
Based on the findings, either modality of class II treatment adds to profile attractiveness as judged by laypeople and orthodontists. There are some differences in opinion between these groups. It is important to study these differences and the specific patient characteristics and apply the best treatment.
Authors’ Contribution
Conceptualization: Homa Farhadifard.
Data curation: Haniyeh Jalili Khradmand, Maryam Salehzadeh.
Formal analysis: Maryam Farhadian.
Funding acquisition: Homa Farhadifard, Vahid Mollabashi, Haniyeh Jalili Khradmand.
Investigation: Haniyeh Jalili Khradmand, Homa Farhadifard, Vahid Mollabashi.
Methodology: Homa Farhadifard, Vahid Mollabashi.
Project administration: Homa Farhadifard, Vahid Mollabashi.
Resources: Maryam Farhadian.
Software: Homa Farhadifard, Vahid Mollabashi.
Supervision: Haniyeh Jalili Khradmand, Maryam Salehzadeh.
Validation: Maryam Farhadian.
Visualization: Homa Farhadifard, Vahid Mollabashi, Marym Salehzadeh.
Writing–original draft: Homa Farhadifard, Vahid Mollabashi, Marym Salehzadeh.
Competing Interests
The authors declare that they have no conflict of interests.
Ethical Approval
This study was approved by the Ethics Committee of Hamadan University of Medical Sciences with the ethics code IR.UMSHA.REC.1400.779. All participants signed consent forms indicating that their photographs would be presented to the study population, and the eyes of the patients were covered to keep their identity confidential.
Funding
This study was approved and financially supported by the Deputy of Research and Technology of Hamadan University of Medical Sciences (grant number: 140010218616). The funder of this study had no role in the study design, data collection, data analysis, data interpretation, or writing the manuscript.
References
- Hosoda M, Stone‐Romero EF, Coats G. The effects of physical attractiveness on job‐related outcomes: a meta‐analysis of experimental studies. Pers Psychol 2003; 56(2):431-62. doi: 10.1111/j.1744-6570.2003.tb00157.x [Crossref] [ Google Scholar]
- Samsonyanová L, Broukal Z. A systematic review of individual motivational factors in orthodontic treatment: facial attractiveness as the main motivational factor in orthodontic treatment. Int J Dent 2014; 2014:938274. doi: 10.1155/2014/938274 [Crossref] [ Google Scholar]
- Santori F, Masedu F, Ciavarella D, Staderini E, Chimenti C, Tepedino M. Effect of class II functional treatment on facial attractiveness, as perceived by professionals and laypeople. Sci Rep 2021; 11(1):13989. doi: 10.1038/s41598-021-93343-0 [Crossref] [ Google Scholar]
- Haas CF, Champion A, Secor D. Motivating factors for seeking cosmetic surgery: a synthesis of the literature. Plast Surg Nurs 2008; 28(4):177-82. doi: 10.1097/PSN.0b013e31818ea832 [Crossref] [ Google Scholar]
- Manche M, Sunitha C, Naveen R, Kiran Kumar P, Saritha T. Treatment options for skeletal class II malocclusion in growing patients-a review. IOSR J Dent Med Sci 2021; 20(3):42-8. doi: 10.9790/0853-2003034248 [Crossref] [ Google Scholar]
- Psomiadis S, Gkantidis N, Sifakakis I, Iatrou I. Perceived effects of orthognathic surgery versus orthodontic camouflage treatment of convex facial profile patients. J Clin Med 2023; 13(1):91. doi: 10.3390/jcm13010091 [Crossref] [ Google Scholar]
- Ioi H, Nakata S, Nakasima A, Counts A. Influence of facial convexity on facial attractiveness in Japanese. Orthod Craniofac Res 2007; 10(4):181-6. doi: 10.1111/j.1601-6343.2007.00382.x [Crossref] [ Google Scholar]
- de Oliveira Meira AC, Custodio W, Vedovello Filho M, Borges TM, de Castro Meneghim M, Santamaria M Jr. How is orthodontic treatment need associated with perceived esthetic impact of malocclusion in adolescents?. Am J Orthod Dentofacial Orthop 2020; 158(5):668-73. doi: 10.1016/j.ajodo.2019.09.009 [Crossref] [ Google Scholar]
- Rocha AD, Casteluci C, Ferreira FP, Conti AC, de Almeida MR, de Almeida-Pedrin RR. Esthetic perception of facial profile changes after extraction and nonextraction class II treatment. Braz Oral Res 2020; 34:e003. doi: 10.1590/1807-3107bor-2020.vol34.0003 [Crossref] [ Google Scholar]
- Kalin K, Iskender SY, Kuitert R. Attractiveness assessment by orthodontists and laypeople judging female profile modifications of class II division 1 malocclusion. Am J Orthod Dentofacial Orthop 2021; 160(2):276-82. doi: 10.1016/j.ajodo.2020.04.032 [Crossref] [ Google Scholar]
- Nanda RS, Ghosh J. Facial soft tissue harmony and growth in orthodontic treatment. Semin Orthod 1995; 1(2):67-81. doi: 10.1016/s1073-8746(95)80094-8 [Crossref] [ Google Scholar]
- Yüksel AG, Iskender SY, Kuitert R, Papadopoulou AK, Dalci K, Darendeliler MA. Differences in attractiveness comparing female profile modifications of class II division 1 malocclusion. Am J Orthod Dentofacial Orthop 2017; 152(4):471-6. doi: 10.1016/j.ajodo.2017.01.025 [Crossref] [ Google Scholar]
- Mendes LM, Janson G, Zingaretti Junqueira-Mendes CH, Garib DG. Long-term profile attractiveness in class II division 1 malocclusion patients treated with and without extractions. Am J Orthod Dentofacial Orthop 2019; 155(3):362-71. doi: 10.1016/j.ajodo.2018.04.030 [Crossref] [ Google Scholar]
- Imani MM, Sanei E, Akhavan Niaki E, Saffar Shahroudi A. Esthetic preferences of orthodontists, oral surgeons, and laypersons for Persian facial profiles. Am J Orthod Dentofacial Orthop 2018; 154(3):412-20. doi: 10.1016/j.ajodo.2017.11.040 [Crossref] [ Google Scholar]
- Taghavi Bayat J, Huggare J, Mohlin B, Akrami N. Predicting orthodontic treatment need: reliability and validity of the Demand for Orthodontic Treatment Questionnaire. Eur J Orthod 2017; 39(3):326-33. doi: 10.1093/ejo/cjw056 [Crossref] [ Google Scholar]
- de Almeida-Pedrin RR, Guimarães LB, de Almeida MR, de Almeida RR, Ferreira FP. Assessment of facial profile changes in patients treated with maxillary premolar extractions. Dental Press J Orthod 2012; 17(5):131-7. doi: 10.1590/s2176-94512012000500018 [Crossref] [ Google Scholar]