Avicenna J Dent Res. 16(2):128-133.
doi: 10.34172/ajdr.1677
Case Report
Periodontally Accelerated Osteogenic Orthodontic in Patients Treated With In-house Clear Aligner: A Case Report
Leila Shahsavand Baghdadi 1, *  , Mohammad Amin Nouroozi 2
, Mohammad Amin Nouroozi 2
Author information:
1Department of Periodontics, Dental Research Center, School of Dentistry, Hamadan University of Medical Sciences, Hamadan, Iran
2Orthodontist, Private Office, Shiraz, Iran
Abstract
The thickness of the alveolar bone is one of the limiting factors of orthodontic tooth movement. Crossing these limitations in orthodontic movements may cause periodontal diseases, root resorption, pulpitis, and the like. Osteogenic orthodontics that is accelerated by the periodontium is one method for overcoming these restrictions and negative effects. Over the last ten years, a large body of research has been conducted on the well-known and efficient technique of alveolar decortication-assisted orthodontic treatment. Corticotomy combined with guided bone regeneration can increase the range of orthodontic treatment by allowing predictable and faster movements beyond traditional methods. Piezo surgery is an innovative procedure that can be used for corticotomy. Piezo surgery has selective cutting (no soft tissue damage) and less bleeding during the surgical procedure.
Keywords: Corticotomy, Piezo surgery, Accelerated osteogenic orthodontic
Copyright and License Information
© 2024 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Shahsavand Baghdadi L, Nouroozi MA. Periodontally accelerated osteogenic orthodontic in patients treated with in-house clear aligner: A case report. Avicenna J Dent Res. 2024; 16(2):128-133. doi:10.34172/ajdr.1677
Background
The limits of tooth movement are defined by the thickness of the alveolar bone and the envelope of discrepancy. If these limits are crossed periodontal tissues may suffer from negative effects. The diminished volume of the cortical bone, sometimes with minimum and other times nonexistent, is a risk factor for loss of attachment because bone resorption occurs along with the direction of tooth movement (1). Treatment for the reduced alveolar bone volume is a challenging issue for orthodontics. Previous research has shown that marginal bone loss occurs in regions where teeth migrate toward the cortical plane (2). Reducing cortical alveolar bone may increase the incidence of dehiscence and fenestrations, which are the most common alveolar defects. An alveolar fenestration is a limited defect of the cortical plate that exposes the underlying root surface without harming the marginal bone; an alveolar dehiscence is the absence of facial or lingual cortical plates, which exposes the root surface (3-5). Alveolar decortication-assisted orthodontic therapy is a well-known and effective method that has undergone substantial research over the last 10 years. It is defined as a surgical method that facilitates orthodontic tooth movement by causing controlled surgical injury to the bone that stimulates bone metabolism. It is performed to temporarily increase tissue turnover and osteopenia, which is followed by a faster rate of orthodontic tooth movement (5). Bryan first described corticotomy surgery’s use in the treatment of malocclusion in 1892 (6). However, Heinrich Kole was the one who brought back alveolar corticotomy in 1959 to treat malocclusion. He coupled an osteotomy apical to the teeth with an interdental alveolar corticotomy procedure (7). Regional accelerated phenomenon (RAP) occurs following surgery. Accelerated bone turnover and reduced regional bone density are two of the main characteristics of RAP, a complicated physiological process. RAP promotes both hard and soft tissue regeneration and local rearrangement (8,9). Corticotomy combined to guided bone regeneration can increase the range of orthodontic treatment by allowing predictable movements beyond traditional methods. The corticotomy technique with bone grafting or periodontally accelerated osteogenic orthodontic (PAOO) seems to be an effective method to minimize the risk of marginal bone loss and fenestration during dental orthodontics (10,11).
Traditional tools such as burs, chisels, and other rotating tools used to cut bone, despite being effective, can cause damage to soft tissues and adjacent nerves. By producing excessive temperature, these devices can disrupt bone regeneration and cause bone necrosis (12,13).
Piezo surgery is an innovative procedure used by Vercellotti to get beyond the restrictions of conventional bone surgery equipment (14). The platform of this gadget houses a potent piezoelectric handpiece that operates between functional frequencies between 25 and 29 kHz. This equipment also has a washing and cooling system with a configurable sterile solution flow from 0 to 60 mL/min. Special scalpels function with a linear vibration pattern and an ultrasonic power that exceeds, with an output range of 5-16 watts and a spatial range of 60-210 µm. Piezoelectric ultrasonic vibrations are used to conduct osteotomies securely and efficiently. Alveolar crown expansion, sinus transplant, and pre-prosthetic surgery were all performed using this method for the first time. The piezoelectric device creates a safe and accurate osteotomy without any osteonecrosis damage thanks to micrometric and selective cutting. This device protects soft tissues and their blood supply by operating on mineral tissues. Osteotomy is one of the most delicate operations in oral and maxillofacial surgery (13). When compared to osteotomy with a burr, which offers a greater field of vision during surgery, piezo surgery has the benefit of reducing bleeding during surgery. In a shorter period of time, piezo surgery can achieve full recovery of sensory and neurological disorders in most patients compared to burs. During piezo osteotomy, the incisions are more precise, and cutting edges are more regular in comparison to burr osteotomy edges. Compared to rotary instruments, piezoelectric devices are safe and effective during surgery. Bone loss during piezo osteotomy cutting was less compared to burr osteotomy, which allowed the areas cut with piezo-osteotomy to fuse properly (15).
Using the piezo surgery with orthodontic treatment accelerates tooth movement, and the effect of combining corticotomy with bone grafting was successful (16).
In this method, the cortical bone, which is highly resistant to orthodontic forces, is cut (17) or drilled without affecting the medullary bone (18).
We have reported periodontal accelerated osteogenic orthodontic in the patient treated with the in-house aligner.
Case Presentation
Diagnosis
A 23-year-old female patient was treated with fixed orthodontic treatment by four quadrant premolar extraction, and re-treatment was sought in terms of relapse in upper incisors due to loss of the retainer in Hamadan University of Medical Sciences, Hamadan, Iran. She had no medical problems. She had excellent oral hygiene and no cavities in dental records. Without any temporomandibular joint issues, the patient’s oral function was normal. In the maxillary segment, she had a diastema between her incisors and labial frenum. Her profile was symmetrical and straight (Figure 1). A cl II dental occlusion was found after an intraoral examination on both sides, with a slight irregularity in the top anterior section. Upper laterals had an inadequate inclination in terms of their previous palatal position (Figure 2). Moreover, they showed bone loss and root kissing with their proximal centrals in the panoramic view (Figure 3). Panoramic radiograph illustrated the existing upper third molar and semi-impaction of lower ones. The cephalometric analysis demonstrated skeletal class I malocclusion with a decreased overbite.

Figure 1.
Extraoral Photographs at the Beginning of Treatment.
.
Extraoral Photographs at the Beginning of Treatment.

Figure 2.
Intraoral Photographs at the Beginning of Treatment.
.
Intraoral Photographs at the Beginning of Treatment.
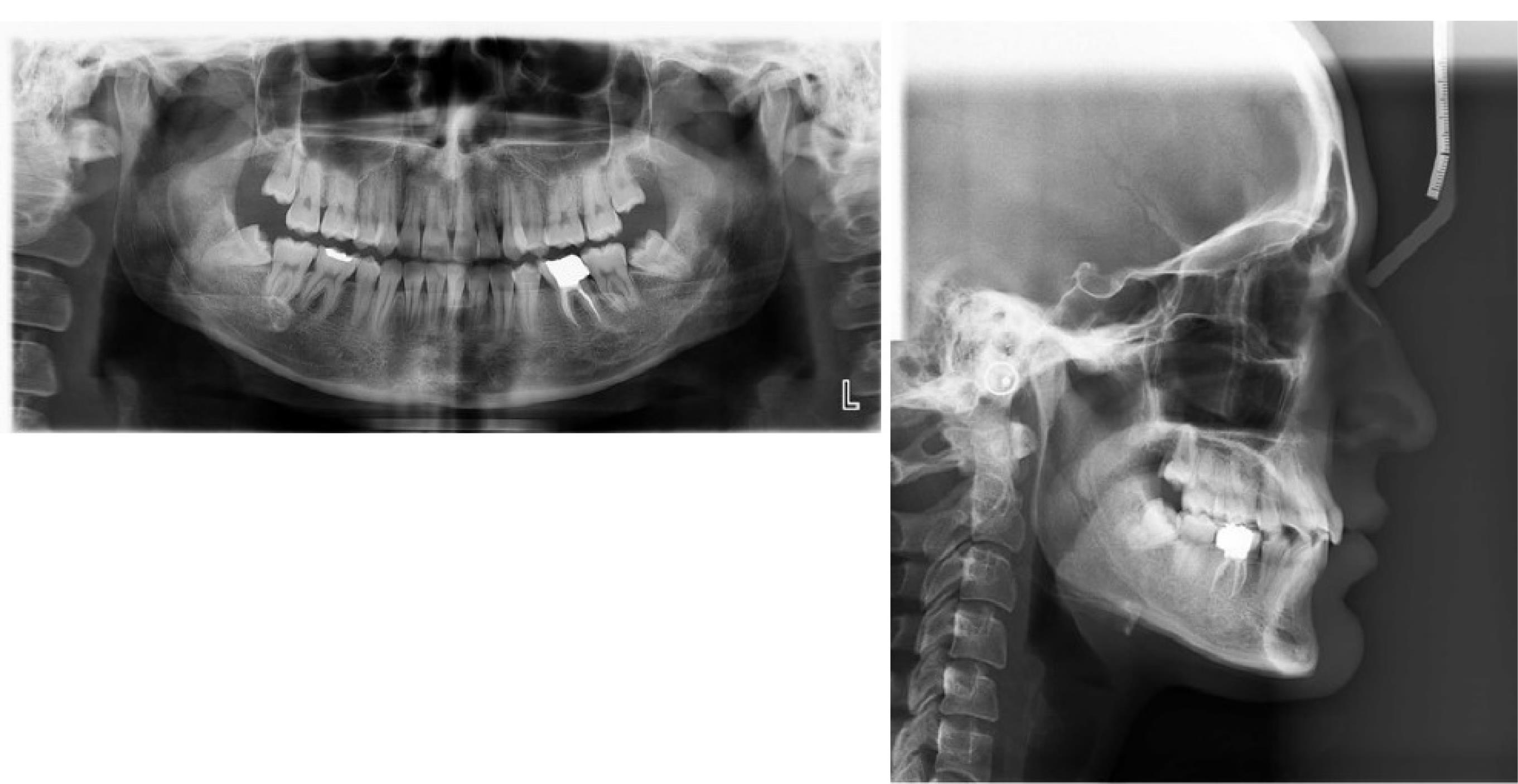
Figure 3.
Initial Radiographs.
.
Initial Radiographs.
Treatment
The patient can be either treated with a fixed orthodontic appliance or in-house clear aligner therapy (CAT). The patient preferred CAT due to several reasons. She had some slight crowding in her upper arch, had fixed orthodontic treatment in the past, and valued its simplicity and aesthetic results. The treatment was performed without tooth extraction and with the help of in-house clear aligner therapy and paralleling roots of teeth 21 and 22 were done. The 3 Shape System was used to conduct an intraoral scan. Following virtual setup and 3D model printing, the # 11 Clear aligner was planned for fabrication. Root paralleling #22 was planned with four clear aligners before corticotomy in that area because of adequate bone between adjacent teeth. The corticotomy technique with bone grafting was applied in #21 and #22 areas. Linear tooth movement and rotational movement were 0.2 mm and 2° per aligner, respectively. The total treatment time was about 5 months, and the patient received a clear aligner every two weeks.
Surgical Procedure
Corticotomy was performed in two areas of #12 and #22 teeth. Before the surgery, the patient used 2.0% chlorhexidine mouthwash for one minute. Then, local anesthesia with lidocaine and epinephrine 1.100000 was injected. With a No. 15 blade, a sulcular incision was created around the target tooth and one to two side teeth. Only the buccal region of the full-thickness flap was pulled aside, exposing the cortical bone (Figure 4A). By employing piezo surgery, the region in issue underwent an interproximal corticotomy that included the thickness of the cortical bone. Beginning 2-3 mm more apically than the alveolar crest, the vertical corticotomy proceeded until 1-2 mm below the apex of the affected tooth (Figure 4B). Next, the bone powder was placed in the area after trimming the absorbable collagen membrane (Figure 4C), and the flap was returned to its original place with a 5-0 monofilament non-absorbable suture (Figure 4D). A periodontal pack was placed.
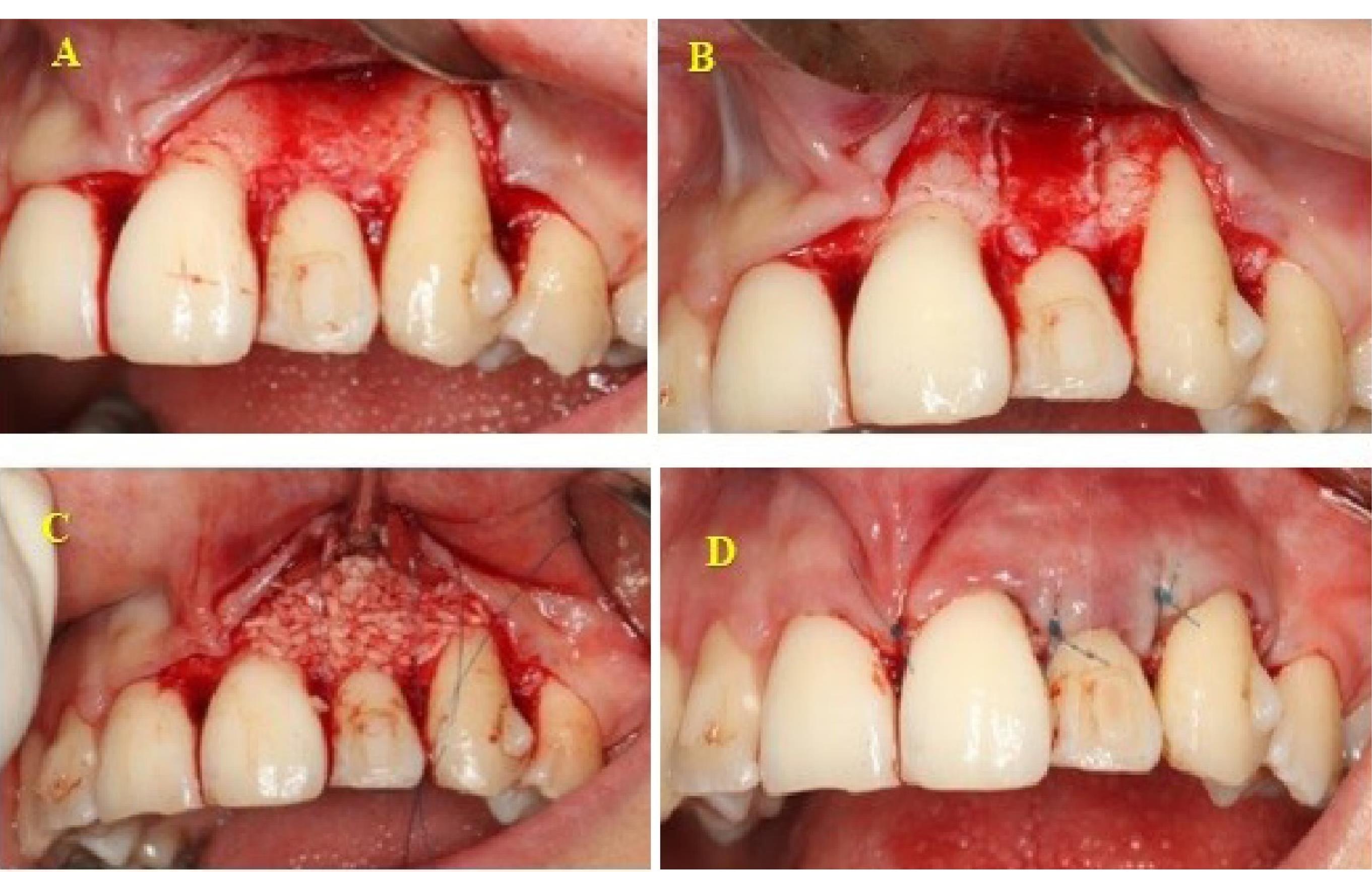
Figure 4.
Corticotomy Procedure: (A) Flap Elevation, (B) Corticotomy, (C) Bone Substitute and Absorbable Collagen Membrane, and (D) Suturing With Monofilament Non-absorbable.
.
Corticotomy Procedure: (A) Flap Elevation, (B) Corticotomy, (C) Bone Substitute and Absorbable Collagen Membrane, and (D) Suturing With Monofilament Non-absorbable.
Post-surgery recommendations included using 500 mg amoxicillin antibiotic for 5 days, 0.2% chlorhexidine mouthwash twice a day for a week, and the acetaminophen pain reliever for three days. The sutures were removed after ten days, and the patient was taught the necessary recommendations to observe hygiene in this area. The three-month follow-up photographs were taken, which are depicted in Figures 5 and 6.

Figure 5.
Extraoral Photographs at the End of Treatment.
.
Extraoral Photographs at the End of Treatment.

Figure 6.
Intraoral Photographs at the End of Treatment.
.
Intraoral Photographs at the End of Treatment.
Discussion
Corticotomy primarily aims to aid difficult orthodontic tooth movement, and its secondary benefit is to shorten treatment times (19). Utilizing corticotomy results in regulated surgical damage to the bone that accelerates bone metabolism for around 4-6 months, shortening the length of time needed for orthodontic therapy (20,21). PAOO seems to be an effective method to minimize the risk of marginal bone loss and bony dehiscence in the case which needs arch expansion and can help correct alveolar dehiscence during orthodontic treatment (22). Moreover, alveolar decortication with augmentation grafting was described by Wilcko et al in 2001 (8).
The combination of this processor with orthodontic treatment accelerates tooth movement and provides increased alveolar volume. Additionally, using CAT as an aesthetic method is a relatively new modality in comparison to fixed orthodontic treatment. As a consequence, it is a developing segment of the orthodontic market and has lately gained popularity because of its attractiveness, clarity, and usability (23). PAOO combined with CAT to benefit from periodontal advantages has not been reported so far in the literature.
Thin alveolar bone is strongly linked with the occurrence of dehiscence (24,25). Dehiscence and fenestration during orthodontic treatment are affected by the direction of movement, the frequency and intensity of orthodontic pressures, the volume and anatomical integrity of periodontal tissues, and other factors (26). The patient in the present case study had an upper anterior segment dehiscence and insufficient inclination of their upper lateral incisors (Figure 4A). Torque correction and re-treatment may deteriorate the current bone dehiscence in such a situation. Selective corticotomy combined with bone grafting and CAT were considered for the patient to resolve the existing bone dehiscence and help correct the lingual root torque of upper lateral incisors. Furthermore, grafting material was used because of the necessity of excessive labiolingual movements. The bone graft is employed to cover fenestrations and dehiscence and improve bone condition (27).
Upper incisors and canine irregularity were relieved after completing clear aligner treatment. Using a clear aligner increased the cooperation of the patient because it is easy to put on and take off and its invisible appearance. This is because, in response to the traumatic stimulation of corticotomy, alveolar turnover is increased in 4 months (8). A combination of orthodontic treatment with corticotomy leads to a reduction in the treatment time (20,21).
The findings of the present paper support those of earlier studies, indicating that corticotomy therapy plus clear aligners may be used to complete treatment in around one-third the time of traditional orthodontics. Transparent aligners are almost undetectable and simple to use. When corticotomy is employed for faster orthodontic movements, by helping a clear aligner, more control over orthodontic movements without the risk of anchorage loss seems more appropriate. Periodontal indicators also improved with the help of clear aligners in terms of easier hygiene (28).
In another study, using the corticotomy along with bone augmentation led to an increase in bone volume and, consequently, greater arch length, and finally, a decrease in the need for tooth extraction, an increase in dental movements, and a reduction in relapse (29).
Another research looked at the effects of aesthetic orthodontic treatment using clear aligners and faster orthodontic movement. The results demonstrated the efficiency of combining these two approaches to shorten treatment times and cope with challenging orthodontic cases (30).
It seems that alveolar decortication and augmentation grafting are useful modalities that provide enhanced treatment outcomes, as well as accelerated leveling and alignment with reduced risk of loss of attachment.
Acknowledgements
The authors would like to thank Nazli Rabienejad, Department of Periodontics, Dental Research Center, School of Dentistry, Hamadan University of Medical Sciences, Hamadan, Iran for her support.
Authors’ Contribution
Conceptualization: Leila Shahsavand Baghdadi, Mohammad Amin Nouroozi.
Data curation: Leila Shahsavand Baghdadi, Mohammad Amin Nouroozi.
Formal analysis: Leila Shahsavand Baghdadi.
Funding acquisition: Leila Shahsavand Baghdadi.
Investigation: Leila Shahsavand Baghdadi.
Methodology: Leila Shahsavand Baghdadi.
Project administration: Leila Shahsavand Baghdadi, Mohammad Amin Nouroozi.
Resources: Leila Shahsavand Baghdadi, Mohammad Amin Nouroozi
Supervision: Leila Shahsavand Baghdadi.
Validation: Leila Shahsavand Baghdadi.
Visualization: Leila Shahsavand Baghdadi.
Writing – original draft: Leila Shahsavand Baghdadi, Mohammad Amin Nouroozi.
Writing – review & editing: Leila Shahsavand Baghdadi.
Competing Interests
The authors declare that they have no conflict of interests.
Ethical Approval
The authors published photos of the patient after obtaining her parents’ consent.
Funding
This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Handelman CS. The anterior alveolus: its importance in limiting orthodontic treatment and its influence on the occurrence of iatrogenic sequelae. Angle Orthod 1996; 66(2):95-110. doi: 10.1043/0003-3219(1996)066<0095:taaiii>2.3.co;2 [Crossref] [ Google Scholar]
- Lund H, Gröndahl K, Gröndahl HG. Cone beam computed tomography evaluations of marginal alveolar bone before and after orthodontic treatment combined with premolar extractions. Eur J Oral Sci 2012; 120(3):201-11. doi: 10.1111/j.1600-0722.2012.00964.x [Crossref] [ Google Scholar]
- Elliot JR, Bowers GM. Alveolar dehiscence and fenestration. Periodontics 1963; 1:245-8. [ Google Scholar]
- Edel A. Alveolar bone fenestrations and dehiscences in dry Bedouin jaws. J Clin Periodontol 1981; 8(6):491-9. doi: 10.1111/j.1600-051x.1981.tb00898.x [Crossref] [ Google Scholar]
- Abdelmalek RG, Bissada NF. Incidence and distribution of alveolar bony dehiscence and fenestration in dry human Egyptian jaws. J Periodontol 1973; 44(9):586-8. doi: 10.1902/jop.1973.44.9.586 [Crossref] [ Google Scholar]
- Guilford SH. Orthodontia, or Malposition of the Human Teeth: Its Prevention and Remedy. Spangler & Davis; 1893.
- Köle H. Surgical operations on the alveolar ridge to correct occlusal abnormalities. Oral Surg Oral Med Oral Pathol 1959; 12(5):515-29. doi: 10.1016/0030-4220(59)90153-7 [Crossref] [ Google Scholar]
- Wilcko WM, Wilcko T, Bouquot JE, Ferguson DJ. Rapid orthodontics with alveolar reshaping: two case reports of decrowding. Int J Periodontics Restorative Dent 2001; 21(1):9-19. [ Google Scholar]
- Shih MS, Norrdin RW. Regional acceleration of remodeling during healing of bone defects in beagles of various ages. Bone 1985; 6(5):377-9. doi: 10.1016/8756-3282(85)90336-9 [Crossref] [ Google Scholar]
- Germeç D, Giray B, Kocadereli I, Enacar A. Lower incisor retraction with a modified corticotomy. Angle Orthod 2006; 76(5):882-90. doi: 10.1043/0003-3219(2006)076[0882:lirwam]2.0.co;2 [Crossref] [ Google Scholar]
- Lee W, Graber V, Robert Jr L, Vig K. Orthodontics: Current Principles and Techniques. India: Elsevier; 2016.
- Köhnke R, Kolk A, Kluwe L, Ploder O. Piezosurgery for sagittal split osteotomy: procedure duration and postoperative sensory perturbation. J Oral Maxillofac Surg 2017; 75(9):1941-7. doi: 10.1016/j.joms.2017.05.003 [Crossref] [ Google Scholar]
- Robiony M, Polini F, Costa F, Vercellotti T, Politi M. Piezoelectric bone cutting in multipiece maxillary osteotomies. J Oral Maxillofac Surg 2004; 62(6):759-61. doi: 10.1016/j.joms.2004.01.010 [Crossref] [ Google Scholar]
- Vercellotti T. Piezoelectric surgery in implantology: a case report--a new piezoelectric ridge expansion technique. Int J Periodontics Restorative Dent 2000; 20(4):358-65. [ Google Scholar]
- Raj H, Singh M, Shah AK. Piezo-osteotomy in orthognathic surgery: a comparative clinical study. Natl J Maxillofac Surg 2022; 13(2):276-82. doi: 10.4103/njms.njms_357_21 [Crossref] [ Google Scholar]
- Apalimova A, Roselló À, Jané-Salas E, Arranz-Obispo C, Marí-Roig A, López-López J. Corticotomy in orthodontic treatment: systematic review. Heliyon 2020; 6(5):e04013. doi: 10.1016/j.heliyon.2020.e04013 [Crossref] [ Google Scholar]
- Lee W. Corticotomy for orthodontic tooth movement. J Korean Assoc Oral Maxillofac Surg 2018; 44(6):251-8. doi: 10.5125/jkaoms.2018.44.6.251 [Crossref] [ Google Scholar]
- Murphy KG, Wilcko MT, Wilcko WM, Ferguson DJ. Periodontal accelerated osteogenic orthodontics: a description of the surgical technique. J Oral Maxillofac Surg 2009; 67(10):2160-6. doi: 10.1016/j.joms.2009.04.124 [Crossref] [ Google Scholar]
- Cassetta M, Pandolfi S, Giansanti M. Minimally invasive corticotomy in orthodontics: a new technique using a CAD/CAM surgical template. Int J Oral Maxillofac Surg 2015; 44(7):830-3. doi: 10.1016/j.ijom.2015.02.020 [Crossref] [ Google Scholar]
- Kim SJ, Park YG, Kang SG. Effects of corticision on paradental remodeling in orthodontic tooth movement. Angle Orthod 2009; 79(2):284-91. doi: 10.2319/020308-60.1 [Crossref] [ Google Scholar]
- Fischer TJ. Orthodontic treatment acceleration with corticotomy-assisted exposure of palatally impacted canines. Angle Orthod 2007; 77(3):417-20. doi: 10.2319/0003-3219(2007)077[0417:otawce]2.0.co;2 [Crossref] [ Google Scholar]
- Brugnami F, Caiazzo A, Mehra P. Can corticotomy (with or without bone grafting) expand the limits of safe orthodontic therapy?. J Oral Biol Craniofac Res 2018; 8(1):1-6. doi: 10.1016/j.jobcr.2017.11.001 [Crossref] [ Google Scholar]
- Miller KB, McGorray SP, Womack R, Quintero JC, Perelmuter M, Gibson J, et al. A comparison of treatment impacts between Invisalign aligner and fixed appliance therapy during the first week of treatment. Am J Orthod Dentofacial Orthop 2007;131(3):302.e1-302.e9. 10.1016/j.ajodo.2006.05.031.
- Richman C. Is gingival recession a consequence of an orthodontic tooth size and/or tooth position discrepancy? “A paradigm shift”. Compend Contin Educ Dent 2011; 32(1):62-9. [ Google Scholar]
- Siriwat PP, Jarabak JR. Malocclusion and facial morphology is there a relationship? An epidemiologic study. Angle Orthod 1985; 55(2):127-38. doi: 10.1043/0003-3219(1985)055<0127:mafmit>2.0.co;2 [Crossref] [ Google Scholar]
- Wehrbein H, Bauer W, Diedrich P. Mandibular incisors, alveolar bone, and symphysis after orthodontic treatment A retrospective study. Am J Orthod Dentofacial Orthop 1996; 110(3):239-46. doi: 10.1016/s0889-5406(96)80006-0 [Crossref] [ Google Scholar]
- Mathews DP, Kokich VG. Accelerating tooth movement: the case against corticotomy-induced orthodontics. Am J Orthod Dentofacial Orthop 2013; 144(1):5-13. doi: 10.1016/j.ajodo.2013.04.008 [Crossref] [ Google Scholar]
- Cassetta M, Altieri F, Barbato E. The combined use of corticotomy and clear aligners: a case report. Angle Orthod 2016; 86(5):862-70. doi: 10.2319/091115-617.1 [Crossref] [ Google Scholar]
- Zimmo N, Saleh MH, Mandelaris GA, Chan HL, Wang HL. Corticotomy-accelerated orthodontics: a comprehensive review and update. Compend Contin Educ Dent 2017; 38(1):17-26. [ Google Scholar]
- Caruso S, Darvizeh A, Zema S, Gatto R, Nota A. Management of a facilitated aesthetic orthodontic treatment with clear aligners and minimally invasive corticotomy. Dent J (Basel) 2020; 8(1):19. doi: 10.3390/dj8010019 [Crossref] [ Google Scholar]