Avicenna J Dent Res. 14(1):47-52.
doi: 10.34172/ajdr.2022.09
Case Report
A Hollow Complete Denture Fabricated Using Neutral Zone Approach for a Severely Resorbed Ridge: A Case Report
Romal Shende 1, *  , Suryakant Deogade 2, Arun Khalikar 3, Sattyam Wankhade 2, Pronoy Mukhopadhyay 1
, Suryakant Deogade 2, Arun Khalikar 3, Sattyam Wankhade 2, Pronoy Mukhopadhyay 1
Author information:
1Postgraduate Student, Department of Prosthodontics, Government Dental College and Hospital, Nagpur, Maharashtra, India-440003
2Associate Professor, Department of Prosthodontics, Government Dental College and Hospital, Nagpur, Maharashtra, India-440003
3Professor & Head, Department of Prosthodontics, Government Dental College and Hospital, Nagpur, Maharashtra, India-440003
Abstract
Prosthetic rehabilitation using complete dentures is quite a challenging task when accompanied by severely atrophic ridges. Various modifications are required in the treatment strategy to optimize the prognosis of the finished prosthesis. Moreover, the increased inter-arch space demands the hollowing of the maxillary denture to mitigate the issues in retention due to increased weight. This case report aims to demonstrate a technique used to fabricate a hollow maxillary denture and a mandibular denture using the neutral zone approach in the case of a severely atrophied ridge.
Keywords: Neutral zone, Hollow denture, Atrophic ridge, All green technique, Increased inter-ridge distance
Copyright and License Information
© 2022 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Shende R, Deogade S, Khalikar A, Wankhade S, Mukhopadhyay P. A hollow complete denture fabricated using neutral zone approach for a severely resorbed ridge: a case report. Avicenna J Dent Res. 2022; 14(1):47-52. doi:10.34172/ajdr.2022.09
Introduction
Complete denture prosthesis is a conventional yet enigmatic treatment strategy in the field of prosthetic dentistry. Establishing adequate retention, stability, and support for a lower denture is still considered a challenging therapeutic intervention due to the lesser surface area for the coverage of the denture-bearing surface (1). Additionally, neuromuscular coordination of the peri-oral muscles considerably influences the stability of the denture (2). The neutral zone is the “area of minimal muscular influence” where the buccal and lingual displacing forces represent an equilibration. Many materials and techniques have been documented in the literature to successfully record the neutral zone area and arrange artificial teeth in the “zone of no-influence” to enhance the stability of a denture fabricated for a severely atrophied mandibular ridge (1).Ridge atrophy is accompanied by an augmented restorative space that equally adds weight and precludes achieving good retention. Hollowing the denture with a retrievable material works toward reducing the weight of the prosthesis and off-loading forces onto the ridge to prevent any further resorption (3).This article aims to describe a case of complete denture rehabilitation using the neutral zone concept and hollowing the maxillary denture to optimize the prognosis of the intended treatment strategy.
Case Report
A 67-year-old male patient was reported to the Department of Prosthodontics with the chief complaint of difficulty in chewing and poor facial appearance due to missing teeth. On examination, the patient presented with completely edentulous maxillary and mandibular arches. The patient was reported to have lost his teeth due to their loosening almost 2-3 years back and was hesitant to get a prosthesis. Following carefully inspecting the topography of the basal seat, the mandibular and maxillary ridge was found to be atrophic (Atwood’s order V). After thorough history taking, the patient was informed about the whole process of the treatment strategy to be psychologically re-assured for better co-operation.
Treatment Strategy
1. Preliminary impressions were, first, made using a high-fusing impression compound (DPI Pinnacle, Bombay Burmah Trading Corporation, Mumbai, India), and primary casts were poured using dental plaster. Then, wax spacers were adapted in consideration with the selective-pressure-impression technique, and custom trays were fabricated as well.
2. The maxillary arch was peripherally traced by the conventional sectional technique using the low-fusing compound (DPI Pinnacle Tracing Sticks, Bombay Burmah Trading Corporation, Mumbai, India). Wax spacer was removed, and a wash impression was made using metal-oxide impression paste. For the atrophic mandibular arch, an all-green method was employed to perform peripheral tracing, followed by trimming the low-fusing compound for the crestal region and making a wash impression record using metal-oxide impression paste. Both the definitive impressions were then poured by applying Type III Dental Stone (Kalstone, Kalabhai Pvt., Ltd., Mumbai, India).
3. Record rims were fabricated over the definitive impression, and a tentative jaw relation record was made accordingly. Using an arbitrary ear-piece type of Facebow, the orientation relation was recorded, and the maxillary cast was mounted onto a semi-adjustable articulator (Figure 1). A tentative centric relation record was used to mount the mandibular cast. The tentative jaw relation record demonstrated an increased inter-ridge distance, adding to the weight of the maxillary denture and thus compromising the retention (Figure 2). At this stage, the decision was made to fabricate a hollow maxillary denture to optimize the retention.

Figure 1.
Facebow Record.
.
Facebow Record.
4. On the mandibular denture base, first, wire pins were attached using auto-polymerizing resin (Trevalon, Dentsply India Pvt. Ltd., Gurgaon, India). Then, a rim of a low-fusing compound was fabricated to record the neutral zone. With the thermally-softened rim placed intra-orally, the patient was asked to perform functional movements such as swallowing and pursing the lips to make the neutral zone record. The neutral zone record was then indexed using putty-consistency condensation silicone (Zeta Plus, Zhermack) on the labial and lingual sides (Figure 3). The compound rim was removed, and the index was applied to fabricate a rim of modelling wax (Y Dents Modelling Wax, MDM Corporation, India) within the confines of the recorded neutral zone (Figure 4).

Figure 4.
Rim of Modelling Wax.
.
Rim of Modelling Wax.
5. Cross-linked acrylic teeth of the anatomic form were set in accordance with the located neutral zone, and a trial was performed accordingly (Figure 5). The trial mandibular denture was then employed to make the external contour impression using light-body addition silicone (ExpressTM VPS impression material light body) by asking the patient to perform the same movements as for making the neutral zone record. Next, the trial dentures were waxed up and prepared for processing. The land area of the maxillary cast was scored with index notches.
6. For hollowing the maxillary denture, a duplicate of the waxed trial was made using irreversible hydrocolloid (Vignette, Dentsply, India) and poured via type III dental stone. Using a 1 mm thick vacuum-formed acrylic sheet, a template of the trial denture was obtained on the duplicated cast (Figure 6). The trial denture was flasked and dewaxed conventionally (Figure 7).
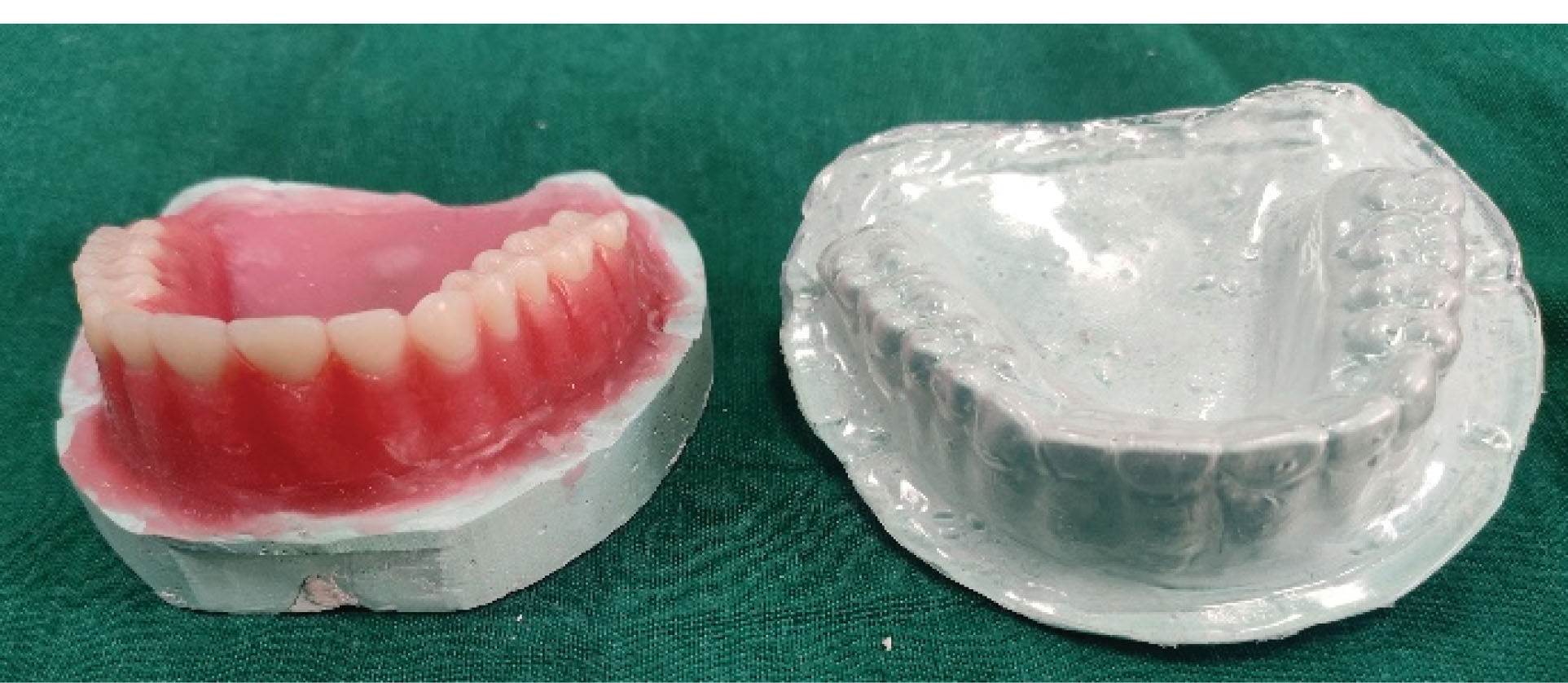
Figure 6.
Duplicated Cast and Template.
.
Duplicated Cast and Template.
7. With the temporary denture base in place and waxed to the cast, a putty spacer was adapted and carved with the acrylic template as a guide for the three-dimensional (3-D) assessment of the proposed hollow cavity. The waxed denture base was dewaxed and packed with heat-polymerising resin to derive the permanent denture base.
8. A replica of the putty spacer was carved onto a glycerine soap bar (Pears, Hindustan Unilever Ltd., Mumbai, India) using a carver (Figure 8), and the 3-D hollow was re-verified using the template over the permanent denture base (Figure 9). With the counter of the trial denture, first, a trial pack was performed using the putty spacer. The putty spacer was then replaced with the glycerin soap spacer, and the final flask closure was then performed for acrylization. The mandibular trial denture was processed by the conventional compression moulding technique.

Figure 8.
Glycerin Soap Spacer and Putty Spacer.
.
Glycerin Soap Spacer and Putty Spacer.
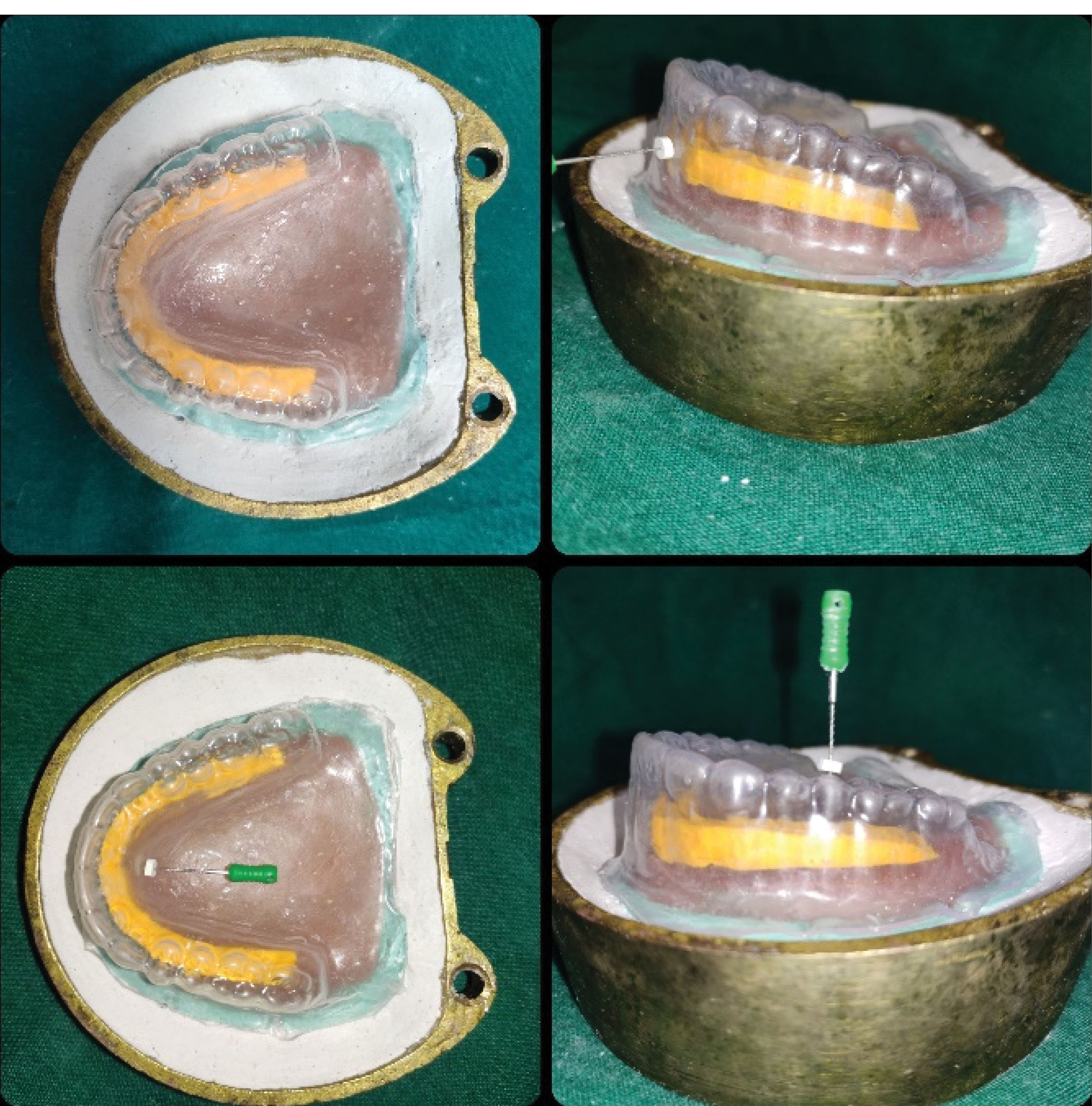
Figure 9.
Re-verification of Three-dimensional Hollow Using the Template.
.
Re-verification of Three-dimensional Hollow Using the Template.
9. Once the dentures were retrieved, openings were drilled on the distal aspect of the maxillary denture behind the second molar (Figure 10). The denture was then immersed into a beaker of water for the dissolution of the soap spacer. Water spray was also conducted to mechanically push and dissolve the spacer out. After complete hollowing, the openings were sealed using auto-polymerizing resin (Figure 11). The dentures were then finished and polished.
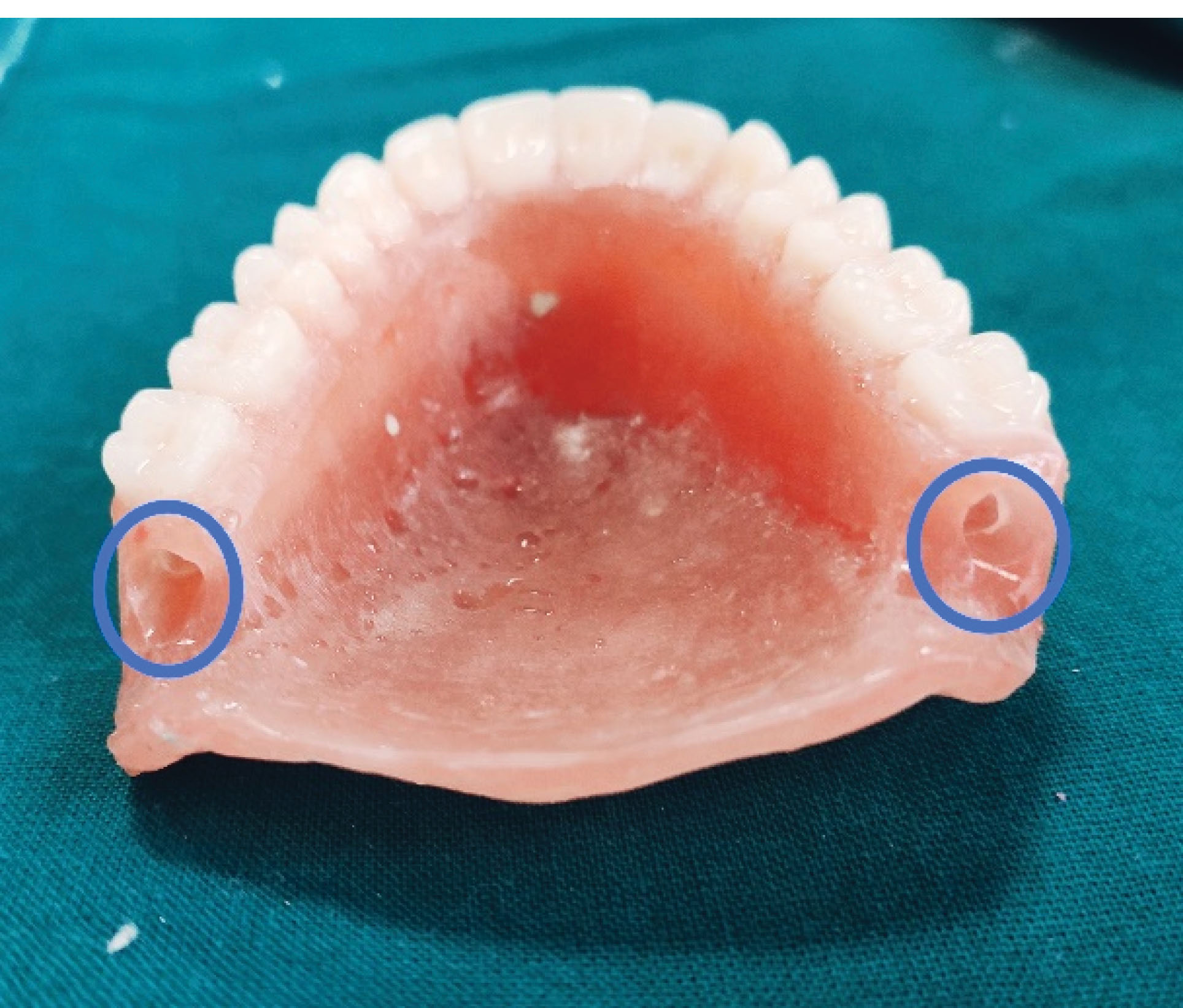
Figure 10.
Drilling of Openings.
.
Drilling of Openings.
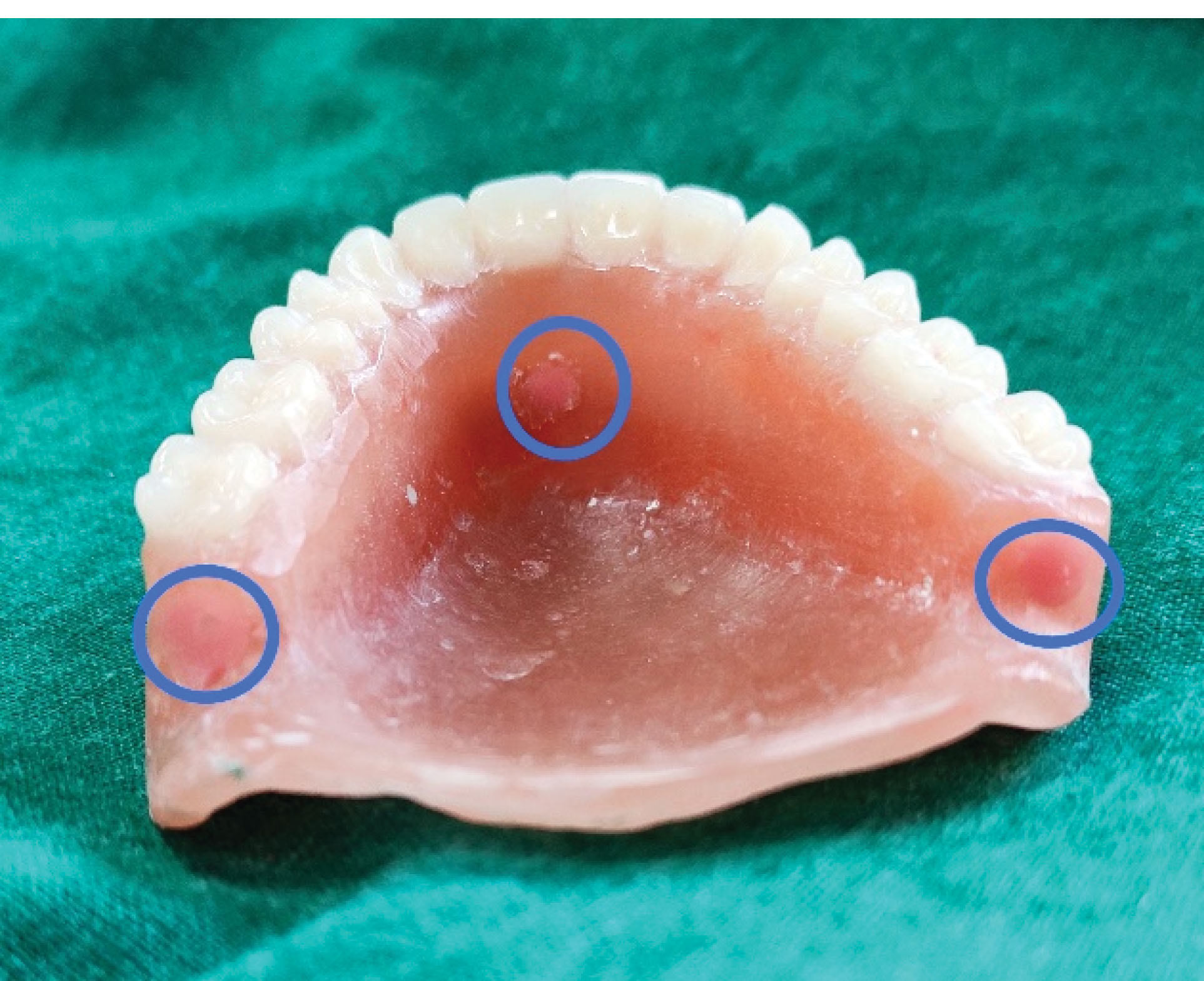
Figure 11.
Sealing of Opening Using Auto-polymerizing Resin.
.
Sealing of Opening Using Auto-polymerizing Resin.
10. To physically confirm the hollowing out process, the maxillary denture was placed in a beaker of water and evidently floated to demonstrate reduced weight (Figure 12). The dentures were then inserted, and instructions for maintenance were explained to the patient. The patient was followed up after 24 hours, a week, and a month. With only minor adjustments performed in subsequent follow-ups, the patient was satisfied with provided prostheses (Figure 13).
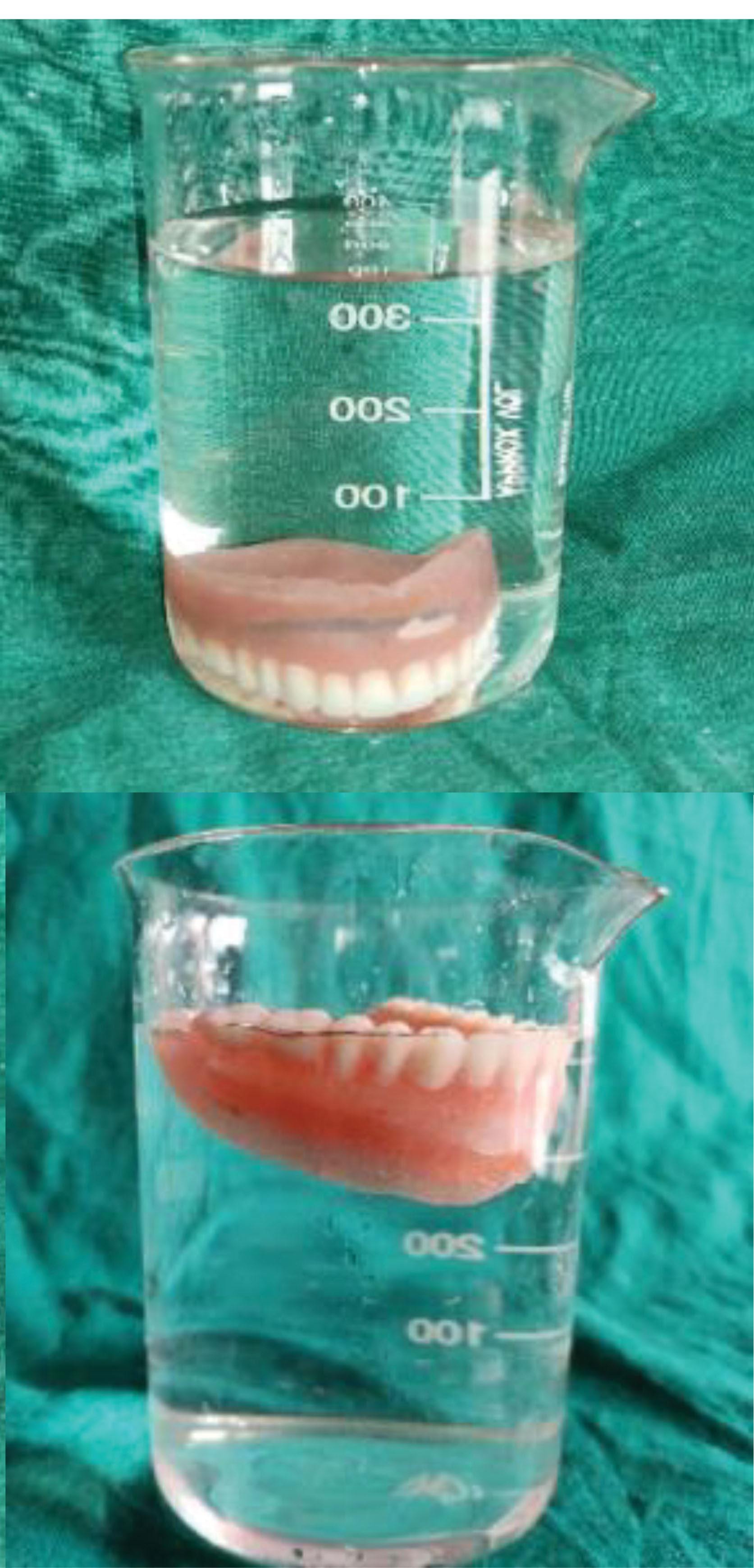
Figure 12.
Floated Denture Demonstrating Reduced Weight.
.
Floated Denture Demonstrating Reduced Weight.

Figure 13.
Preoperative and Postoperative Profiles.
.
Preoperative and Postoperative Profiles.
Discussion
The prognostic value of a complete denture prosthesis lies in how well the denture fulfils the requirements of retention, stability, and support in function. The resorption of the basal seat is usually accompanied by an increase in the inter-arch space, reduced retentive ability, and poor stability of the complete denture (4). Prosthetically rehabilitating such cases involves mitigating the issues of poor denture foundation support and handling the increased weight of the maxillary denture which, in conjunction with the effects of gravity, contributes to a non-retentive prosthesis (5). Various impression techniques have been postulated and developed over the years that work to optimize the retention and support derived from the basal seat (6). The all-green technique used in this report works towards better recording the supporting tissues at their functional state. This technique provides a chance to record the tissues of a resorbed ridge by distributing the stresses mostly over the primary stress-bearing area (the buccal shelf area) using a less viscous compound to avoid extensive compression (7). The neutral zone record using the anthropoidal pouch technique allows setting the denture teeth in an area not influenced by the labial, buccal, and lingual musculature, further enhancing the retentive abilities and the stability of the denture (8).
Numerous techniques have been confirmed in the literature for reducing the weight of the maxillary denture using various intervening spacer materials (9-15). Ideally, the applied material must be able to withstand the temperature and pressures of compression during processing and must also be retrievable thereafter (16). In this technique, the putty spacer allows the trial packing of the denture without the spacer being affected, and the soap spacer works to withstand the processing technique, as well as being easily retrievable for successfully hollowing out the maxillary denture.(17) The difficulty in retrieving was encountered in the inter-canine region due to its curvature, but the excellent water-solubility of the glycerine soap spacer worked to mitigate this issue. Moreover, the vacuum-form template allows the operator to better visualise the 3-D coverage of the spacer to be used, thus ensuring better resin coverage throughout the intaglio surface without the inclusion of extensive porosities or voids.
Conclusions
A versatile approach is imperative in prosthetic rehabilitation using complete dentures. The dynamism with which edentulous patients are present, requires the clinician to be prepared with modified techniques to maintain prognostically-favourable standards of care. In the cases of severely atrophic ridges, modifying various treatment phases to optimize the retention of the finished denture is a difficult yet possible task. This report sought to document such versatility in the required treatment strategy.
Authors’ Contribution
RS: concept and design of case, SD: reviewing the case report.
AK: final approval, SW: critical revision for important intellectual content, PM: drafting the manuscript.
Conflict of Interest Disclosures
The authors declare that they have no conflict of interests.
Ethical Statement
Written informed consent was obtained from the patient for the use of the patient’s clinical information and images for publication.
References
- Gahan MJ, Walmsley AD. The neutral zone impression revisited. Br Dent J 2005; 198(5):269-72. doi: 10.1038/sj.bdj.4812118 [Crossref] [ Google Scholar]
- Salinas TJ. Treatment of edentulism: optimizing outcomes with tissue management and impression techniques. J Prosthodont 2009; 18(2):97-105. doi: 10.1111/j.1532-849X.2009.00438.x [Crossref] [ Google Scholar]
- O’Sullivan M, Hansen N, Cronin RJ, Cagna DR. The hollow maxillary complete denture: a modified technique. J Prosthet Dent 2004; 91(6):591-4. doi: 10.1016/j.prosdent.2004.03.021 [Crossref] [ Google Scholar]
- Fattore LD, Fine L, Edmonds DC. The hollow denture: an alternative treatment for atrophic maxillae. J Prosthet Dent 1988; 59(4):514-6. doi: 10.1016/0022-3913(88)90053-4 [Crossref] [ Google Scholar]
- Carlsson GE. Clinical morbidity and sequelae of treatment with complete dentures. J Prosthet Dent 1998; 79(1):17-23. doi: 10.1016/s0022-3913(98)70188-x [Crossref] [ Google Scholar]
- McCord JF, Grant AA. Impression making. Br Dent J 2000; 188(9):484-92. doi: 10.1038/sj.bdj.4800516 [Crossref] [ Google Scholar]
- Tunkiwala A, Ram S. Management of mandibular poor foundation: conventional complete dentures. Dent Pract 2013; 11(5):34-7. [ Google Scholar]
- Prashanti E, Suresh S, Jagan MR. Use of neutral zone technique in unstable mandibular dentures. Indian Dentist Research and Review 2007; 2:26-32. [ Google Scholar]
- Radke U, Mundhe D. Hollow maxillary complete denture. J Indian Prosthodont Soc 2011; 11(4):246-9. doi: 10.1007/s13191-011-0082-9 [Crossref] [ Google Scholar]
- Worley JL, Kniejski ME. A method for controlling the thickness of hollow obturator prostheses. J Prosthet Dent 1983; 50(2):227-9. doi: 10.1016/0022-3913(83)90022-7 [Crossref] [ Google Scholar]
- Gardner LK, Parr GR, Rahn AO. Simplified technique for the fabrication of a hollow obturator prosthesis using vinyl polysiloxane. J Prosthet Dent 1991; 66(1):60-2. doi: 10.1016/0022-3913(91)90354-y [Crossref] [ Google Scholar]
- Caculo SP, Aras MA, Chitre V. Hollow dentures: treatment option for atrophic ridges a clinical report. J Prosthodont 2013; 22(3):217-22. doi: 10.1111/j.1532-849X.2012.00921.x [Crossref] [ Google Scholar]
- Shetty V, Gali S, Ravindran S. Light weight maxillary complete denture: a case report using a simplified technique with thermocol. J Interdiscip Dent 2011; 1(1):45-8. doi: 10.4103/2229-5194.77208 [Crossref] [ Google Scholar]
- Chalian VA, Barnett MO. A new technique for constructing a one-piece hollow obturator after partial maxillectomy. J Prosthet Dent 1972; 28(4):448-53. doi: 10.1016/0022-3913(72)90250-8 [Crossref] [ Google Scholar]
- Gundawar S, Zamad A, Gundawar S. Light weight dentures: an innovative technique. Contemp Clin Dent 2014; 5(1):134-7. doi: 10.4103/0976-237x.128695 [Crossref] [ Google Scholar]
- Shaikh N, Pattanaik S, Pattanaik B, Sunder A. Maxillary hollow denture: a literature review. Int J Appl Dent Sci 2021; 7(2):517-20. doi: 10.22271/oral.2021.v7.i2h.1258 [Crossref] [ Google Scholar]
- Qanungo A, Aras MA, Chitre V, Mysore A, Da Costa GC. An innovative and simple technique of hollow maxillary complete denture fabrication. J Clin Diagn Res 2016; 10(8):ZD23-5. doi: 10.7860/jcdr/2016/20383.8264 [Crossref] [ Google Scholar]