Avicenna J Dent Res. 14(4):160-164.
doi: 10.34172/ajdr.2022.499
Original Article
Comparison of Dimensions of the Palate Between Individuals With and Without Nasal Septum Deviation on Cone-Beam Computed Tomography Images in an Iranian Population
Fatemeh Nasereslami 1  , Tahmineh Razi 2, Elham Banakar 3 , Parya Emamverdizadeh 2, Sedigheh Razi 2, *
, Tahmineh Razi 2, Elham Banakar 3 , Parya Emamverdizadeh 2, Sedigheh Razi 2, *
Author information:
1Private Office, Maragheh, East Azarbiajan, Iran
2Department of Oral and Maxillofacial Radiology, Faculty of Dentistry, Tabriz University of Medical Sciences, Tabriz, Iran
3Student of Dentistry, Tabriz University of Medical Sciences, Tabriz, Iran
Abstract
Background: Nasal septum deviation might disrupt the integrity of nasal septum components, resulting in deformity. Such changes might affect the morphology of adjacent structures. The aim of the present study was to evaluate the dimensions of the palate in subjects with and without nasal septum deviation on cone-beam computed tomography (CBCT) images in an Iranian population.
Methods: In the present cross-sectional study, the CBCT images of subjects with and without nasal septum deviation were evaluated in two groups (n=107) referred to the Department of Oral and Maxillofacial Radiology, Tabriz Faculty of Dentistry in 2017. The presence or absence of nasal septum deviation and its severity were evaluated in association with palatal dimensions. Data were analyzed by SPSS. Independent samples t test was used to compare the dimensions of the palate. Finally, the Mann-Whitney U test was employed to compare palatal arch depth (PAD)/palatal interalveolar length (PIL) ratios.
Results: There were no significant differences between the two groups in terms of the palatal depth (P=0.967), palatal width (P=0.223), and palatal depth/palatal width ratio (P=0.644). However, the results demonstrated significant differences in palatal depth (P<0.001) and palatal width (P=0.05) between male and female subjects.
Conclusions: Overall, no significant differences were observed in the dimensions of the palate (depth and width) and their ratios between subjects with and without nasal septum deviation, although greater palatal dimensions (depth and width) were detected in males compared to females.
Keywords: Nasal septal deviation, Depth of palate, Cone-beam computed tomography
Copyright and License Information
© 2022 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Nasereslami F, Razi T, Banakar E, Emamverdizadeh P, Razi S. Comparison of dimensions of the palate between individuals with and without nasal septum deviation on cone-beam computed tomography images in an Iranian population. Avicenna J Dent Res. 2022; 14(4):160-164. doi:10.34172/ajdr.2022.499
Introduction
Nasal septum deviation disrupts the configuration of the nasal septum components in adults (septal cartilage, ethmoid vertical plate, and vomer bone), and it might be cartilaginous, cartilaginous-osseous, and osseous. This deviation might result in a deformity at the cartilage-vomer bone conjunction and the creation of a nasal spine (1-3).
Nasal septum deviation might be congenital (4) or acquired or it might be caused by trauma or during birth (5-7) and results in obstruction, secondary infections, inflammation of mucous membranes, and infection of the middle meatus. Aging increases the risk of nasal septum deviation (8).
The structural deviation of the nasal septum causes the asymmetry of the nasal cavity and changes in the morphology of turbinates and nasal resistance (9). A deep dome-shaped palate might increase pressure on the nasal septum, leading to nasal septum deviation (10).
According to the American Academy of Otolaryngology, 80% of the population have nasal septum deviation, varying from a minor deviation from the hypothetical midline of the nasal cavity to significant deviations to join the septum to turbinates on the external wall of the nasal cavity; in the latter case, triangular bony extensions are created at the junction between the ethmoid vertical plate and the upper segment of vomer bone (11).
The prevalence of nasal septum deviation varies with age. An interventional study showed that nasal septum deformities were found in 50%-90% of adults (12,13). Based on the findings of a study, nasal septum without deviation was observed in women at a rate twice that in men (14).
In recent years, cone-beam computed tomography (CBCT) has been used for the radiographic evaluation of maxillofacial hard tissues; however, CT images are preferable to CBCT images for the functional comparison of soft tissue components in association with hard tissues due to inadequate resolution of CBCT images (15-20). In addition, CBCT images have drawn attention due to the provision of different views and a higher diagnostic efficacy (21).
Different imaging techniques can be applied to diagnose nasal septum deviation, including the CT scan, magnetic resonance imaging, and three-dimensional techniques (22,23).
The results of a study by Akbay et al demonstrated a positive relationship between nasal septum deviation and the depth of the palatal vault. Nasal septum deviation results in the obstruction of airways, interfering with the function of the nose and affecting the structure and morphology of the maxilla. Narrowing of the maxillary arch and a deep palate result from nasal septum deviation, and if the palate is already deep, its severity increases, thus exacerbating an increase in the severity of the existing deviation in the nasal septum (1). The concomitant occurrence of concha bullosa and nasal septum deviation affects the depth and curvature of the palatal bone (24). Nasal septum deviation affects the form and symmetry of the facial skeleton by changing the growth pattern (25). A study by Kawalski and Spiewak on the etiologic factors for nasal septum deformities in children revealed greater deviation in the anterior region of the septum compared to its posterior region (3).
There are differences in the designs of previous studies, and there is a limited number of studies on the comparison of the dimensions of the palate in individuals with and without nasal septum deviation on CBCT images. Accordingly, the present study was designed with a larger sample size to evaluate the dimensions of the palate in subjects with and without nasal septum deviation in terms of age and gender in an Iranian population.
Materials and Methods
Study Type and Population
In the present cross-sectional study, 214 subjects (107 subjects with nasal septum deviation and 107 subjects without septum deviation) were selected from those referring to the Department of Oral and Maxillofacial Radiology, Faculty of Dentistry, Tabriz University of Medical Sciences (2017) for CBCT examinations for different reasons. All the radiographic examinations were performed for other diagnostic purposes such as implant placement. The inclusion criteria consisted of no history of surgery in the nasal and palatal area, no trauma to the face, no history of chronic sinusitis, absence of lesions within the maxillary sinuses, absence of osseous lesions, and no jaw deformities. On the other hand, subjects < 18 years of age and completely edentulous individuals were excluded from the study.
Procedural Steps
The demographic data of the subjects were recorded, and written informed consent was obtained from all of them.
The CBCT images of the subjects were taken using a NewTom VGi Cone Beam CT (Verona/Italy) machine in the Department of Oral and Maxillofacial Radiology, Faculty of Dentistry, Tabriz University of Medical Sciences. This machine delivers a cone-shaped X-ray beam and has a flat panel detector, 1536×1920 pixels, a pixel size of 127×127 μm2, a pixel depth of 14 bits, a rotation of 360°, a scan time of 18 s, a kVp of 110, FOV of HRes Zoom (high-resolution zoom 15×15) and mA of 1-20. NNT Viewer software program (version 2.17) was applied for the initial and final reconstruction of images. The exposure conditions were adjusted automatically. Data from the CBCT examinations were registered in the NNT viewer software program, and the images were viewed on a 32-bit 19-inch PHILPS LCD monitor (19OB) with a resolution of 1024×1208 pixels in a dimly lit room by an oral and maxillofacial radiologist. Axial cross-sections with a thickness of 0.5 mm were used to prepare CBCT images. In addition, 1-mm-thick coronal cross-sections underwent evaluation.
The presence or absence of the nasal septum deviation was determined by coronal views. In the case of deviation, the middle nasal septum was divided into three equal parts in the superior-inferior dimension, and the location of deviation was determined in one of these thirds based on maximum convexity. In the medio-lateral dimension, the nasal cavity with the maximum septal convexity was also classified into three equal parts from the septum to the external wall (the internal third, the middle third, and the external third). The location of the deviation was defined in one of these thirds based on maximum convexity. Then, the deviated septal length (DSL) was determined by measuring the perpendicular line drawn from the most convex point of the deviated septum to the hypothetical location of the septum at the middle of the nasal cavity. In both groups, the distance from the bone crest next to the middle of the maxillary first molar tooth on one side to the other side was measured on the coronal view as the palatal interalveolar length (PIL) and recorded on the relevant checklist.
To measure palatal arch depth (PAD) in all samples on the coronal view, a perpendicular line was drawn from the crista galli to the palatal bone, and the contact point was designated point ‘P’. Next, the perpendicular line drawn from point ‘P’ to the line connecting the bone crest next to the middle of the maxillary first molar tooth on one side to the other side was determined as the PAD and recorded in the relevant checklist. Measurements in relation to the severity of nasal septum deviation and palatal dimensions were performed using lines and points that are described as follows (Figure 1):
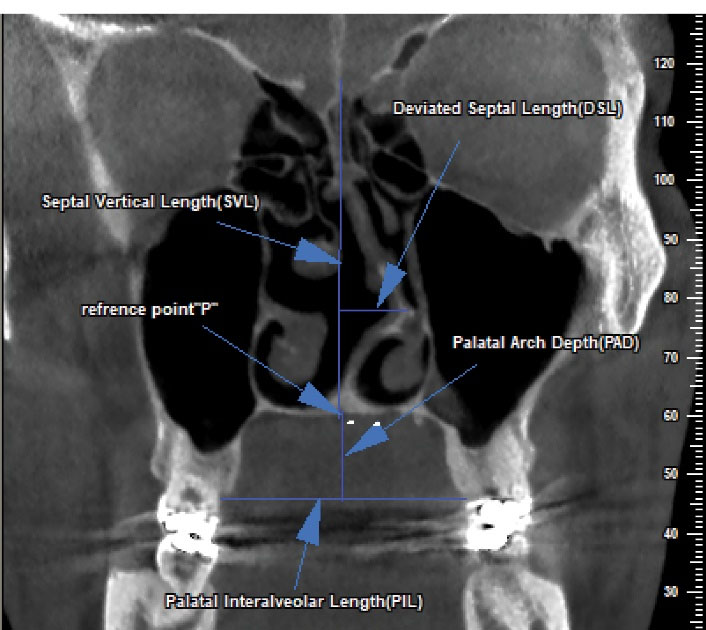
Figure 1.
Measuring the Depth and Width of the Palate and the Severity of Septal Deviation by Determining Relevant Points and Lines in Coronal CBCT Image. Note. CBCT: Cone-beam computed tomography.
.
Measuring the Depth and Width of the Palate and the Severity of Septal Deviation by Determining Relevant Points and Lines in Coronal CBCT Image. Note. CBCT: Cone-beam computed tomography.
Point ‘P’: In the coronal view, a vertical line was drawn from the crista galli to the palatal bone to achieve point ‘P’.
PAD: The palatal depth was defined as the length of the line drawn from point ‘P’ to the line connecting the crest of the bone on the mid-lateral aspect of the first maxillary molar on one side to that on the opposite side.
PIL: On the coronal view, the distance between the crest of the bone on the mid-lateral aspect of the maxillary first molar on one side to that on the opposite side was considered the width of the palate.
DSL: It represents the length of the line drawn from the maximum convexity of the deviated septum to the hypothetical line indicating the location of a non-deviated septum.
The presence or absence of deviation was diagnosed on the coronal view, and when there was a septal deviation, the septum was divided into three equal parts in the superior-inferior dimension, and the location of deviation was determined in one of these parts in terms of the maximum convexity of the deviation. Regarding the mediolateral dimension, the nasal cavity with the maximum septal convexity was grouped into three equal parts from the septum to the external wall (internal third, middle third, and external third), and the location of the septal deviation was defined in one of these parts based on the location of the maximum convexity of deviation. Then, the DSL was determined by measuring the perpendicular line extending from the maximum curved point of the septum to the hypothetical point of the septum in the middle of the nasal cavity.
In both groups, on the coronal view, the distance between the crest of the bone on the mid-lateral aspect of the maxillary first molar on one side and that on the other side was measured as the PIL, and the value was recorded in the checklist.
To measure PAD in all samples, on the coronal view, first, a vertical line was drawn from the crista galli to the palatal bone, and the intersection was dubbed as point ‘P’. Next, the length of a perpendicular line from this point to the line connecting the crest of bone at the mid-lateral aspect of the maxillary first molar on one side to that on the other side was recorded in the checklist as the depth of the palate. PAD/PIL (palatal angle size) was used to compare the depth of the palate and its changes in the presence of nasal septum deviation.
Independent samples t test was employed to compare PAD and PIL in terms of age. Chi-squared and Mann-Whiney U tests were used to compare the two genders and the PAD/PIL ratios between the two groups, respectively. All the statistical analyses were performed with SPSS 17, and statistical significance was set at P < 0.05.
Results
In the present study, of all the individuals with and without no nasal septum deviation, 65 (60.7%) and 42 (39.3%), as well as 47 (439%) and 60 (56.1%) cases were females and males, respectively. In addition, the mean age of the subjects in the group with and without deviation was 43.39 ± 11.93 and 45.2 ± 11.76 years, respectively. Table 1 presents the descriptive statistics of palatal dimension measurements.
Table 1.
Descriptive Statistics of Palatal Dimension Measurements
|
|
Group Without Nasal Septum Deviation
Mean±SD (mm)
|
Group With Nasal Septum Deviation
Mean±SD (mm)
|
P Value
|
| PAD |
14.94 ± 2.86 |
14.96 ± 3.30 |
0.967 |
| PIL |
38.98 ± 3.62 |
38.27 ± 4.79 |
0.223 |
| PAD/PIL |
0.38 ± 0.08 |
0.41 ± 0.25 |
0.644 |
| DSL |
0 |
4.18 ± 1.41 |
|
Note. SD: Standard deviation; PAD: Palatal arch depth; PIL: Palatal interalveolar length; DSL: Deviation septal length.
Based on the comparison of age, PAD, PIL, and PAD/PIL ratios, no significant differences were observed in the means of these parameters between the two groups (P = 0.277, P = 0.967, P = 0.223, and P = 0.644 for age, PAD, PIL, and PAD/PIL, respectively).
In addition, PAD and PIL were compared between male and female subjects, the results of which are provided in Table 2. The results demonstrated significant differences in PAD (P < 0.001) and PIL (P = 9.005) between male and female subjects.
Table 2.
Comparison of Parameters Between Male and Female Subjects
|
|
|
Mean±SD (mm)
|
P value
|
| PAD |
Female |
14.03 ± 2.67 |
< 0.001 |
| male |
15.97 ± 3.20 |
| PIL |
Female |
37.85 ± 4.75 |
0.005 |
| Male |
39.49 ± 3.45 |
Note. SD: Standard deviation; PAD: Palatal arch depth; PIL: Palatal interalveolar length.
Discussion
The deviation of the nasal septum might lead to deformity by disrupting the order and integrity of nasal septum components. The resultant changes might affect the morphology of adjacent structures. It is possible to use CBCT images to evaluate these deviations and their effect on facial appearance. In the present study, palatal dimensions were evaluated and compared between individuals with and without nasal septum deviation. In this study, there was no significant relationship between gender and nasal septum deviation, which is consistent with the results of Akbay (1), Dalili Kajan et al (24), and Bahemmat and Hadian (26). Furthermore, Bahemmat and Hadian reported no significant relationship between age and nasal septum deviation.
Although the difference was not significant, the frequency of nasal septum deviation was higher in males compared to females in the present study, which is in line with the results of studies by Akbay et al (1) and Dalili Kajan et al (24).
Based on the results of the study by Akbay et al, there was a direct relationship between nasal septum deviation and the depth of the palatal arch, which contradicts the results of the present study. Such a discrepancy between the results might be attributed to the small sample size and a different study design in the study by Akbay et al, evaluating three groups (n = 50). In the study by Dalili Kajan et al, no significant relationship was found between nasal septum deviation and an increase in the depth of the palate.
In the present study, consistent with the study by Akbay et al, there was no significant relationship between nasal septum deviation and PIL. Akbay et al reported that an increase in the depth of the palate, in association with its depth, resulted in a decrease in the maxillopalatal curve angle. Similarly, Dalli reported no significant differences in PIL between samples with and without nasal septum deviation.
The PAD/PIL ratio in subjects with nasal septum deviation in the subjects evaluated by Akbay et al was higher than that in subjects without nasal septum deviation; due to almost equal PIL in all three groups, it might be concluded that the palate was deeper in the group with deviation.
In addition, in the study by Dalili Kajan et al, there was a positive relationship between DSL and the PAD/PIL ratio in subjects with concomitant nasal septum deviation and concha bullosa; therefore, the results of the two above-mentioned studies are different from those of the present study. This contradiction between the results might be attributed to differences in the grouping of the subjects, differences in sample sizes, and the difference in the imaging machine.
In the present study, PAD and PIL values were compared between male and female subjects. The results revealed that PAD and PIL values were higher in males compared to females, which corroborates the result of a study by Al-Zubair (27). Such a difference in dimension between males and females might be due to the smaller size of the alveolar ridge and weaker muscles in women compared to men. These findings differ from those reported by Akbay et al in relation to the effect of gender on the dimensions of the palate, while in the majority of animals and human beings, males have a larger body size compared to females (24). In a study by Nourbakhsh et al, the greatest difference in the dimensions of the skull between male and female subjects was related to maxillary sinus dimensions (21).
Dalili Kajan et al did not report any significant differences in PAD, PIL, ad PAD/PIL variables between subjects with and without nasal septum deviation, which is in conformity with the results of the current study. In the present study, no significant relationship was found between nasal septum deviation and palate-related parameters in the study groups and different mean ages, which is consistent with the findings of Dalili Kajan et al. The similarity between the results of these two studies might be because both studies were conducted on subjects > 18 years of age.
Conclusions
Overall, there were no significant differences in the palatal dimensions (depth and width) and their ratios between subjects with and without nasal septum deviation. The results demonstrated statistically significant differences in the dimensions (depth and width) of the palate between male and female subjects.
Author Contributions
Conceptualization: Sedigheh Razi, Tahmineh Razi.
Data curation: Fatemehe Nasereslami.
Formal Analysis: Sedigheh Razi, Tahmineh Razi, Parya Emamverdizadeh.
Investigation: Fatemehe Nasereslami, Sedigheh Razi, Tahmineh Razi, Parya Emamverdizadeh, Elham Banakar.
Methodology: Sedigheh Razi, Tahmineh Razi.
Project administration: Sedigheh Razi.
Supervision: Sedigheh Razi,Tahmineh Razi, Parya Emamverdizadeh.
Validation: Sedigheh Razi, Tahmineh Razi, Parya Emamverdizadeh, Elham Banakar.
Visualization: Sedigheh Razi, Tahmineh Razi.
Writing-original draft: Fatemehe Nasereslami- Elham Banakar.
Writing-review & editing: Elham Banakar.
Conflict of Interest Disclosures
The authors declare that they have no conflict of interests.
Ethical Statement
The present study was approved by the Ethics Committee of the Tabriz University of Medical Sciences (Ethics No. IR.TBZMED.REC.1396.1272).
References
- Akbay E, Cokkeser Y, Yilmaz O, Cevik C. The relationship between posterior septum deviation and depth of maxillopalatal arch. Auris Nasus Larynx 2013; 40(3):286-90. doi: 10.1016/j.anl.2012.07.016 [Crossref] [ Google Scholar]
- Lebowitz RA, Galli SKD, Holliday RA, Jacobs JB. Nasal septal deviation: a comparison of clinical and radiological evaluation. Oper Tech Otolayngol Head Neck Surg 2001; 12(2):104-6. doi: 10.1053/otot.2001.24766 [Crossref] [ Google Scholar]
- Kawalski H, Spiewak P. How septum deformations in newborns occur. Int J Pediatr Otorhinolaryngol 1998; 44(1):23-30. doi: 10.1016/s0165-5876(98)00036-6 [Crossref] [ Google Scholar]
- Podoshin L, Gertner R, Fradis M, Berger A. Incidence and treatment of deviation of nasal septum in newborns. Ear Nose Throat J 1991; 70(8):485-7. [ Google Scholar]
- Cashman EC, Farrell T, Shandilya M. Nasal birth trauma: a review of appropriate treatment. Int J Otolaryngol 2010; 2010:752974. doi: 10.1155/2010/752974 [Crossref] [ Google Scholar]
- Higuera S, Lee EI, Cole P, Hollier LH Jr, Stal S. Nasal trauma and the deviated nose. Plast Reconstr Surg 2007; 120(7 Suppl 2):64S-75S. doi: 10.1097/01.prs.0000260722.91183.50 [Crossref] [ Google Scholar]
- Moghadas H, Abouali O, Faramarzi A, Ahmadi G. Numerical investigation of septal deviation effect on deposition of nano/microparticles in human nasal passage. Respir Physiol Neurobiol 2011; 177(1):9-18. doi: 10.1016/j.resp.2011.02.011 [Crossref] [ Google Scholar]
- Farid M, Metwalli N. Computed tomographic evaluation of mouth breathers among paediatric patients. Dentomaxillofac Radiol 2010; 39(1):1-10. doi: 10.1259/dmfr/80778956 [Crossref] [ Google Scholar]
- Grutzenmacher S, Robinson DM, Grafe K, Lang C, Mlynski G. First findings concerning airflow in noses with septal deviation and compensatory turbinate hypertrophy--a model study. ORL J Otorhinolaryngol Relat Spec 2006; 68(4):199-205. doi: 10.1159/000091473 [Crossref] [ Google Scholar]
- Proffit WR, Fields HW Jr, Sarver DM. Contemporary Orthodontics. 4th ed. St. Louis: Mosby; 2013. p. 141.
- Stallman JS, Lobo JN, Som PM. The incidence of concha bullosa and its relationship to nasal septal deviation and paranasal sinus disease. AJNR Am J Neuroradiol 2004; 25(9):1613-8. [ Google Scholar]
- Reitzen SD, Chung W, Shah AR. Nasal septal deviation in the pediatric and adult populations. Ear Nose Throat J 2011; 90(3):112-5. doi: 10.1177/014556131109000308 [Crossref] [ Google Scholar]
- Salihoglu M, Cekin E, Altundag A, Cesmeci E. Examination versus subjective nasal obstruction in the evaluation of the nasal septal deviation. Rhinology 2014; 52(2):122-6. doi: 10.4193/Rhino13.057 [Crossref] [ Google Scholar]
- Mladina R, Cujić E, Subarić M, Vuković K. Nasal septal deformities in ear, nose, and throat patients: an international study. Am J Otolaryngol 2008; 29(2):75-82. doi: 10.1016/j.amjoto.2007.02.002 [Crossref] [ Google Scholar]
- White SC, Pharoah MJ. Oral Radiology: Principles and Interpretation. 7th ed. St. Louis: Mosby; 2014. p. 197-8.
- Chindasombatjaroen J, Kakimoto N, Murakami S, Maeda Y, Furukawa S. Quantitative analysis of metallic artifacts caused by dental metals: comparison of cone-beam and multi-detector row CT scanners. Oral Radiol 2011; 27(2):114-20. doi: 10.1007/s11282-011-0071-z [Crossref] [ Google Scholar]
- Mah P, Reeves TE, McDavid WD. Deriving Hounsfield units using grey levels in cone beam computed tomography. Dentomaxillofac Radiol 2010; 39(6):323-35. doi: 10.1259/dmfr/19603304 [Crossref] [ Google Scholar]
- McNamara JA. Influence of respiratory pattern on craniofacial growth. Angle Orthod 1981; 51(4):269-300. doi: 10.1043/0003-3219(1981)051<0269:iorpoc>2.0.co;2 [Crossref] [ Google Scholar]
- Ricketts RM. Respiratory obstruction syndrome. Am J Orthod 1968; 54(7):495-507. doi: 10.1016/0002-9416(68)90218-2 [Crossref] [ Google Scholar]
- O’Ryan FS, Gallagher DM, LaBanc JP, Epker BN. The relation between nasorespiratory function and dentofacial morphology: a review. Am J Orthod 1982; 82(5):403-10. doi: 10.1016/0002-9416(82)90189-0 [Crossref] [ Google Scholar]
- Nourbakhsh R, Razi S, Razi T. Evaluation of relation of dimensional measurement of different anatomic skull structures to determine sexual dimorphism in cone beam CT images of an Iranian population. J Res Med Dent Sci 2018; 6(3):33-8. doi: 10.5455/jrmds.2018636 [Crossref] [ Google Scholar]
- Mamikoglu B, Houser S, Akbar I, Ng B, Corey JP. Acoustic rhinometry and computed tomography scans for the diagnosis of nasal septal deviation, with clinical correlation. Otolaryngol Head Neck Surg 2000; 123(1 Pt 1):61-8. doi: 10.1067/mhn.2000.105255 [Crossref] [ Google Scholar]
- Cummings CW, Fredrickson JM, Harker LA, Krause CJ, Richardson MA, Schuller DE. Otolaryngology, Head and Neck Surgery. St. Louis: Mosby; 2015. p. 658.
- Dalili Kajan Z, Khademi J, Nemati S, Niksolat E. The effects of septal deviation, concha bullosa, and their combination on the depth of posterior palatal arch in cone-beam computed tomography. J Dent (Shiraz) 2016; 17(1):26-31. [ Google Scholar]
- Goergen MJ. Nasal Septal Deviation and Nasofacial Skeletal Form: A Cross-Sectional Study of a 7-18 Year-old Cohort. J Anat 2016; 299(3):295-306. [ Google Scholar]
- Bahemmat N, Hadian H. The frequency of nasal septal deviation and concha bullosa and their relationship with maxillary sinusitis based on CBCT finding. Int J Med Res Health Sci 2016; 5(11):152-6. [ Google Scholar]
- Al-Zubair NM. Determinant factors of Yemeni maxillary arch dimensions. Saudi Dent J 2015; 27(1):50-4. doi: 10.1016/j.sdentj.2014.08.005 [Crossref] [ Google Scholar]