Avicenna J Dent Res. 13(4):130-134.
doi: 10.34172/ajdr.2021.25
Original Article
The Effect of Oral Ketorolac Compared to Ibuprofen on Edema, Trismus, and Pain After Mandibular Third Molar Surgery
Mostafa Govahi 1  , Hamidreza Ajami 2, Vahid Khalili 3 , Ayda Paydar 4, *, Gooya Kabir 5
, Hamidreza Ajami 2, Vahid Khalili 3 , Ayda Paydar 4, *, Gooya Kabir 5
Author information:
1Oral and Maxillofacial Surgeon, School of Dentistry, Shahid Sadoughi University of Medical Science, Yazd, Iran.
2Oral and Maxillofacial Surgeon, Dental School, Ardabil University of Medical Science, Ardabil, Iran.
3Dentist in Private Office, Dental School, Ardabil University of Medical Science, Ardabil, Iran.
4School of Dentistry, Shahid Sadoughi University of Medical Science, Yazd, Iran.
5Shahid Sadoughi university of medical scinces,Yazd,Iran.
Abstract
Background: Latent third molar extraction is the most common surgery in dentistry. Common complications of this surgery include pain, swelling, and trismus. To control these side effects, several drugs have been developed and evaluated in various studies. However, the present study is the first one to compare the effects of ibuprofen and ketorolac on pain, swelling, and trismus after molar surgery.
Methods: This study was a split-mouth clinical trial. To conduct the trial, 20 candidates were selected from among patients referring to Surgery Department of the Dentistry School at Yazd Shahid Sadoughi University of Medical Sciences for mandibular third molar removal surgery. The patients were divided into two groups after the surgery: one group received ibuprofen, and the other one received ketorolac. Pain, swelling, and trismus were evaluated prior to the surgical procedure, 24 hours later, and one week after the surgery. Data were analyzed by SPSS software version 22 by using Wilcoxon statistical tests and paired t test.
Results: Ibuprofen and ketorolac had similar effects on pain relief (P value>0.05). Studying the two groups produced similar results regarding improvement in mouth opening (P value>0.05). Improvement pace of the postoperative swelling was significantly faster in the group receiving ketorolac compared to the one receiving ibuprofen (P value <0.05).
Conclusions: It was concluded that ibuprofen and ketorolac had positive and almost similar effects on pain control, edema, and trismus after molar surgery. However, ketorolac was more effective in controlling edema after surgery.
Keywords: Molar surgery, Ketorolac, Ibuprofen
Copyright and License Information
© 2021 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Citation: Govahi M, Ajami H, Khalili V, Paydar A, Kabir G. The Effect of Oral Ketorolac Compared to Ibuprofen on Edema, Trismus, and Pain After Mandibular Third Molar Surgery. Avicenna J Dent Res. 2021;13(4):130-134. doi: 10.34172/ ajdr.2021.25.
Background
Highlights
Latent third molar extraction is the most common surgery in dentistry, which includes soft tissue flap and bone graft removal. The postoperative inflammation causes severe pain, edema, and limited mouth opening in most cases. Surgical trauma symptoms caused after extraction of the latent third molar represent an excellent clinical model for studying acute pain and evaluating therapeutic effectiveness of the common prescribed medications (1,2).
Acute pain is often associated with physical symptoms originating from the sympathetic branch of the autonomic nervous system, which manifests itself as tachycardia, increased blood pressure, sweating, dilated pupils, and paleness (3). In addition to anesthetics, steroidal and non-steroidal anti-inflammatory drugs (NSAIDs) are commonly prescribed to relieve moderate pain caused by inflammatory conditions and soft tissue trauma. The mechanism of action of NSAIDs prevents the release of cyclooxygenase (COX) which is an enzyme responsible for the production of prostaglandins (PGs) with three isoforms of COX1, COX2, COX3 (4).
Ibuprofen is a type of NSAID with anti-inflammatory and antipyretic properties, mainly used in the clinic due to its proved efficacy and reliability compared to similar drugs. It belongs to the group of propionic acid derivatives, which in addition to its other activities, reduces the biosynthesis of PGs and inhibits the migration of leukocytes to the area (5). In the classification of anti-inflammatory drugs, ibuprofen belongs to the group of non-selective COX1 (an enzyme involved in protecting gastric mucosa and kidney tissue) and COX2 (an enzyme involved in the process of inflammation) inhibitors (6,7).
Ketorolac is a potent NSAID with moderate anti-inflammatory properties (8). It is a non-selective cox inhibitor that blocks the production of PGs. Clinical studies have shown that a single-dose of this drug has more curative effects compared to morphine and pethidine in moderate-to-severe postoperative pain with fewer side effects. In standard animal studies, the analgesic activity of ketorolac is 800 times higher than that of aspirin. In all evaluations, ketorolac is more effective than indomethacin and naproxen (9).
This study aimed to compare the effects of ketorolac and ibuprofen on pain, edema, and mouth opening restriction in adolescent and adult patients who had undergone bilateral surgical removal of lower third molar teeth in School of Dentistry, Yazd Shahid Sadoughi University of Medical Sciences.
Materials and Methods
This clinical trial was conducted using split-mouth method. Random selection method was applied and 20 candidates were selected for mandibular third molar removal via surgery. The patients were 16 to 35 years old and had referred to the Surgery Department at School of Dentistry, Yazd Shahid Sadoughi University of Medical Sciences. Considering several factors such as the significance level of 5% and the test power of 8%, the results from the previous study, and the amount of standard deviation of trismus size S = 9, 18 people were needed to achieve a significant difference of at least 6 mm in the two groups. With 10% loss, however, 20 people entered the study. The sample size was determined by strength test on the website www.lee.dante.br, which showed the sample size of 9 patients in each group to reach 0.8 strength. Also, two surgeries were performed by one surgeon for each patient. The side undergoing surgery first and the drug used were randomly selected using the integrated flow chart at www.randomization.com (7).
Inclusion criteria for this study were: the absence of systemic diseases; the age range of 16 to 35 years; the absence of any systemic condition affecting body organs such as anemia, epilepsy, diabetes, addiction, and alcohol consumption, which could jeopardize surgery, prevent prescription of the desired drug, or complicate repair of the surgical area; the presence of local lesions, including cysts or adenogenic tumors (dependent or independent on the third molar); the strikes on the area, any signs of inflammation (pericoronitis) or infection; non-use of any medication, especially anti-inflammatory drugs 3 days before the surgery; no history of allergy to NSAIDs (ibuprofen or ketorolac); non-existence of conditions reducing the patient’s immune system (including a history of chemotherapy in recent year, or consumption of immunosuppressive drugs); as well as the lack of pregnancy or lactation at the time of surgery. On the other hand, patients with diabetes, bony metabolic diseases, and immunodeficiency problems, those having removed the tooth from one side of their mouth and not referring for the surgery of the other side, as well as patients not taking their medications as prescribed were all excluded from the study.
After identifying the study participants, they were randomly classified into two groups and underwent the surgery to remove a lower left or right third molar. The same surgeon performed all surgeries under local anesthesia (lidocaine + epinephrine) in the morning sessions. Anesthesia technique (i.e., lower alveolar nerve trunk block) was implemented by using 2% lidocaine with 1: 100 000 epinephrine and by inserting an aspiration-capable dental syringe into a 27 mm long needle. Surgical blade No. 15 was used to create the flap. The selected flap was a standard envelope flap, and the incision was sulcular which started from the mesial of first molar and up to the distal area of the second molar, where it ended as a hocky stick incision towards the buccal. Then mucoperiosteal flap elevated by the alveolar periosteum whitout traumatizing. Up to the bone surface of the third molar was exposed and the flap was removed by Minnesota Retractor. The occlusal, buccal, and distal bones of the third molar were removed by direct surgical handpiece (JAPAN NSK-EX-6B) mounted on a 702-carbide fissure mill. When necessary, the tooth was sectioned and removed. The area was washed with normal saline and the incision was sutured with 3.5 Vicryl suture thread (Supa Iran), and the patient was given the necessary instructions for routine oral health care after surgery.
After the surgery, two types of drugs, including ibuprofen 200 mg and ketorolac 10 mg were prepared (Caspian Pharmaceutical Company) in similar capsules to blind the participants and researchers. Patients were provided with the required number of capsules and advised to take one capsule (from the onset of pain after the surgery) every 6 hours for 2 days. They were also recommended to take acetaminophen 500 mg as rescue dose if pain occurred during the interval between drug administrations. Considering the fact that the interval between the supplementary and main doses was not less than 1 hour, the number of supplementary doses was recorded by the patient. Furthermore, when the dentist prescribed antibiotics, the patients were treated with antibiotics and provided with the necessary advice. Patients were examined on the day of surgery, 48 hours (2 days) later, and 168 hours (7 days) after the surgery and their trismus condition, pain level, and facial swelling were evaluated.
According to the previous studies, patients who experienced molar surgery and did not receive painkillers reported the pain visual analogue scale (VAS) of 8, where 0 represented no pain and 10 suggested the worst imaginable pain on the VAS scale (10). Since pain management was essential for patient in ours study, placebo was not used for the control group. The rate of pain for patients of the two groups was assessed using the 11-point numerical pain rating scale (VAS), and they were asked to pay attention to the percentage and degree of pain in 6, 12, and 24 hours after the surgery. In order to evaluate edema in patients, facial contour of each patient was measured from the mouth corner to the mandibular angle in mm 48 and 168 hours after the surgery. In addition, the patients’ mouth opening was evaluated by measuring the maximum distance between incisal edge of maxillary central incisor to the incisal edge of mandibular central incisor 48 hours and 168 hours after the surgery.
Finally, the obtained data were analyzed by SPSS version 22 using Wilcoxon and paired t-test statistical tests.
Results
Out of our 20 study participants, 11 were male (55%) and 9 were female (45%). Participants were within the age range of 18-35 years with a mean of 25.25±4.71.
Table 1 shows the mean mouth opening value (in mm) before the surgery, 2 days later, and 7 days after the surgery for those patients who received ketorolac and ibuprofen. According to the results from the Wilcoxon test, no significant statistical difference was observed between the two groups in terms of the mouth opening values at any of the studied times (P< 0.05). Considering the ketorolac group, the mean mouth opening values were significantly different in the three measured times (P> 0.05), but in the ibuprofen group, no statistically significant difference was found between days 2 and 7 after the surgery (P= 0.207).
Table 1.
Comparison Between Ketorolac and Ibuprofen Groups With Regard to Mouth Opening (mm) at the Studied Time Intervals
|
Drug
|
Time
|
|
Prior to the Surgery (Mean ± SD)
|
48 h After the surgery (Mean ± SD)
|
168 h After the Surgery (Mean ± SD)
|
| Ketorolac |
45.85±6.04 |
23.16±7.12 |
30.58±9.81 |
| Ibuprofen |
45.3±6.63 |
26.42±18.19 |
31.79±7.85 |
|
P value |
0.41 |
0.3 |
0.44 |
Following the results from Wilcoxon test, no statistically significant difference was detected between the two groups regarding the mean edema (distance from the mouth corner to the mandibular angle) prior to and 2 days after the surgery (P < 0.05). However, mean edema was significantly different between the two groups one week after the surgery (P= 0.019) (Table 2). According to the results of t test, the mean edema values measured at three time intervals were significantly different in the ketorolac group (P > 0.05). However, no significant difference was observed between the mean edema values measured on days 2 and 7 after the surgery in the ibuprofen group (P= 0.267).
Table 2.
Comparison Between Ketorolac and Ibuprofen Groups With Regard to the Distance From the Mouth Corner to the Mandibular Angle (Degrees) at the Studied Time Intervals
|
Drug
|
Time
|
|
Prior to the Surgery (Mean ± SD)
|
48 h After the surgery (Mean ± SD)
|
168 h After the Surgery (Mean ± SD)
|
| Ketorolac |
86.4±18.18 |
105.35±6.45 |
104.4±6.62 |
| Ibuprofen |
88.15±13.52 |
106.2±6.04 |
106.05±6.26 |
|
P value |
0.72 |
0.17 |
0.02 |
The mean edema was also measured using the distance between the tragus point and the mouth corner point after surgery. The findings of Wilcoxon test revealed no significant difference between the two groups in terms of edema at the studied time intervals (P< 0.05) (Figure 1). The results of t-test showed that the mean edema values were significantly different in 3 studied days in both groups (P >0.
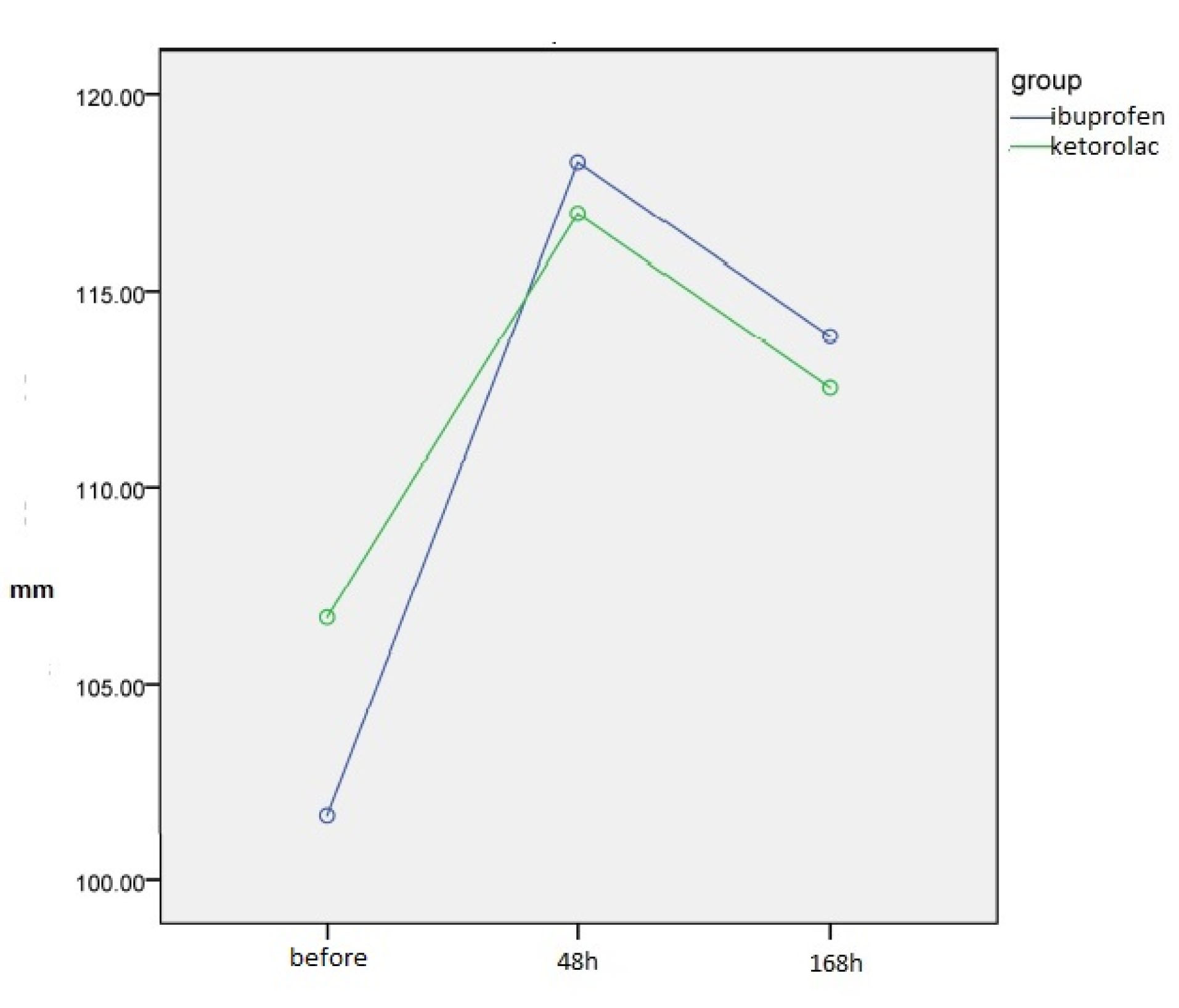
Figure 1.
Comparison of Mean Edema Score (mm) Between Ketorolac and Ibuprofen Groups at the Examined Time Intervals.
.
Comparison of Mean Edema Score (mm) Between Ketorolac and Ibuprofen Groups at the Examined Time Intervals.
Table 3 shows the average pain score (according to the VAS scale) after surgery in patients who took ketorolac and ibuprofen on the day of surgery, 2 days later, and 1 week after the surgery. According to the results from the Wilcoxon test, no statistically significant difference was found between the two groups in terms of pain scores at any of the studied time intervals (P< 0.05) (Figure 2). The results of t-test showed a significant difference between the two study groups with regard to average pain score in the three studied time intervals (P= 0.000).
Table 3.
Comparison Between Ketorolac and Ibuprofen Groups With Regard to Pain at the Studied Time Intervals (VAS scale)
|
Drug
|
Time
|
Prior to the surgery
(Mean ± Standard deviation)
|
48 hours after the surgery (Mean ± Standard deviation)
|
168 hours after the surgery (Mean ± Standard deviation)
|
| Ketrolac |
7.62±0.45 |
5.75±0.77 |
3.97±0.69 |
| Ibuprofen |
7.47±0.59 |
5.87±0.91 |
4±0.81 |
|
P value |
0.911 |
0.313 |
0.317 |
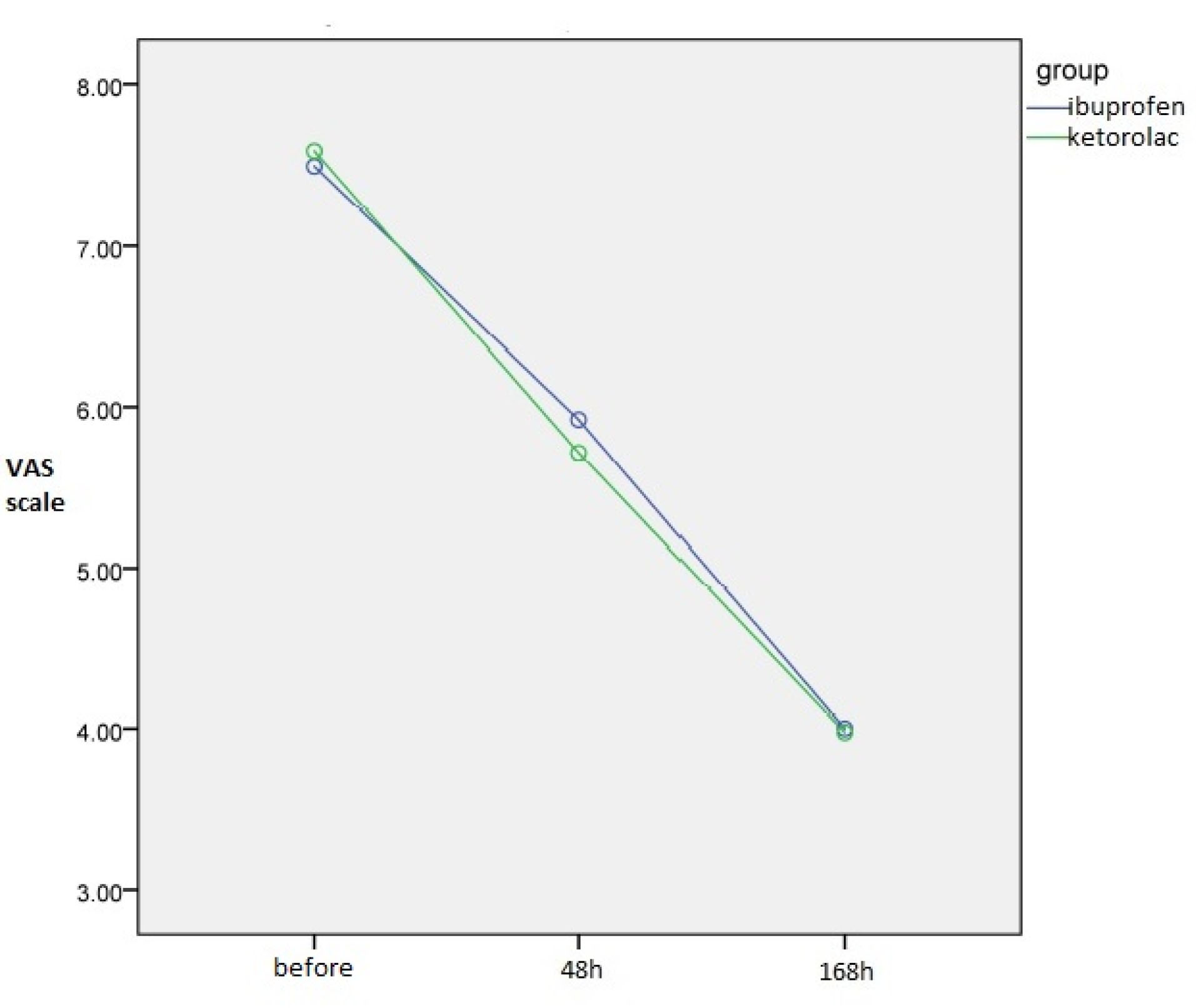
Figure 2.
Comparison of Mean Pain Score Between Ketorolac and Ibuprofen Groups at the Examined Time Intervals (VAS Scale).
.
Comparison of Mean Pain Score Between Ketorolac and Ibuprofen Groups at the Examined Time Intervals (VAS Scale).
Discussion
Latent third molar extraction is the most common surgery in dentistry throughout the world. Common complications of this surgery include pain, swelling, and trismus. To control these side effects, several drugs have been introduced and evaluated in various studies. Numerous studies have evaluated the effect of different NSAIDs on postoperative complications. For example, de Oliveira et al compared the effects of ketorolac and ibuprofen and reported that ketorolac had a more positive effect on swelling, pain, and trisomy than ibuprofen (1).
As previously mentioned, postoperative pain is one of the main complications of molar surgery. Our study generated similar results concerning improvement of pain intensity in both groups. Gazal et al administered ibuprofen, acetaminophen, and diclofenac to patients who underwent molar surgery and assessed their pain scores immediately, 2, 4, and 6 hours after the surgery (11). Jain et al prescribed ibuprofen and aceclofenac to the patients and compared their postoperative pain scores 24 hours after drug use (12). Walton et al evaluated and compared the patients’ postoperative pain 1, 2, and 3 hours after administration of ketorolac and diclofenac (13). All these studies showed positive effects of ibuprofen and ketorolac on improvement of molar postoperative pain, which was in line with our study results.
Another side effect of the molar extraction surgery is the restriction on mouth opening. Different studies have evaluated the distance between upper and lower incisors before and after the surgery to measure trismus (6,14,15). In the present study, the rate of mouth opening was measured before, two days after the operation, and one week after the operation in mm for both groups. On the second day after the surgery, mouth opening was limited in all patients. After administration of the drugs, an increase was observed in the rate of mouth opening in both groups. Trindade et al also reported an increased postoperative trismus after administration of ketorolac (8), which was confirmed in a study by Carlsen and Alexandersen on ibuprofen (16).
Postoperative facial edema is another unwanted complication of third molar removal, which was evaluated using two linear measurements: 1) the distance between mouth corner to the mandibular angle and 2) distance between the tragus point and the mouth corner point. According to the results from our study, high inflammation was observed in all patients on the second day after surgery. This inflammation decreased in both groups after one week, but inflammation was significantly lower in the group receiving ketorolac rather than ibuprofen. Therefore, ketorolac is preferred over ibuprofen in terms of inflammation because it accelerates the return to normal oral function for the patients. The distance between the tragus point and the mouth corner point was also measured using the similar method. Inflammation decreased after one week of drug use in both groups and no significant difference was found between the two study groups in this regard. In the same vein, de Oliveira et al measured edema, that is, the distance from chin to the bottom of the ear. They found that edema peaked at 48 hours postoperatively and was well-controlled after one week of ibuprofen administration (1). In this regard, their results were consistent with our findings. Troullos et al measured facial edema in patients using a type of face-bow and evaluated the distance between pins. They reported that the administration of ibuprofen reduced edema significantly (6). Moreover, Olmedo et al evaluated edema by a visual index and demonstrated that ketorolac was effective in reducing edema after molar surgery (17).
Conclusions
This study revealed that ibuprofen and ketorolac had positive and almost similar effect on pain control, edema, and trismus after third molar extraction. Although the effects of these two drugs were almost the same, ketorolac was found to be more effective in controlling edema after surgery.
Conflict of Interest Disclosures
The authors declare that they have no conflict of interests.
Ethical Statement
The present study was approved by the Research and Medical Ethics Committee of Shahid sadoughi yazd University of Medical Sciences (ethics code: IR.Ssu.REC.1398.091).
Authors’ Contribution
MG: Conceptualization, Methodology. HA: Conceptualization, Project administration. VKH: Data Curation, Investigation. AK: Writing - original draft; Writing - review & Editing. GK: Validation.
References
- de Oliveira JC, de Oliveira GA, Bassi AP. Comparative assessment of the effect of ibuprofen and etodolac on edema, trismus, and pain in lower third molar surgery: a randomized clinical trial. J Oral Maxillofac Surg 2016; 74(8):1524-30. doi: 10.1016/j.joms.2016.04.003 [Crossref] [ Google Scholar]
- Moore AR, Straube S, Paine J, Derry S, McQuay HJ. Minimum efficacy criteria for comparisons between treatments using individual patient meta-analysis of acute pain trials: examples of etoricoxib, paracetamol, ibuprofen, and ibuprofen/paracetamol combinations after third molar extraction. Pain 2011; 152(5):982-9. doi: 10.1016/j.pain.2010.11.030 [Crossref] [ Google Scholar]
- de Sousa Santos JA, da Silva LC, de Santana Santos T, Menezes Júnior LR, de Assunção Oliveira AC, Brandão JR. Comparative study of tramadol combined with dexamethasone and diclofenac sodium in third-molar surgery. J Craniomaxillofac Surg 2012; 40(8):694-700. doi: 10.1016/j.jcms.2012.01.001 [Crossref] [ Google Scholar]
- Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison of six methods. Pain 1986; 27(1):117-26. doi: 10.1016/0304-3959(86)90228-9 [Crossref] [ Google Scholar]
- Moore PA, Hersh EV. Combining ibuprofen and acetaminophen for acute pain management after third-molar extractions: translating clinical research to dental practice. J Am Dent Assoc 2013; 144(8):898-908. doi: 10.14219/jada.archive.2013.0207 [Crossref] [ Google Scholar]
- Troullos ES, Hargreaves KM, Butler DP, Dionne RA. Comparison of nonsteroidal anti-inflammatory drugs, ibuprofen and flurbiprofen, with methylprednisolone and placebo for acute pain, swelling, and trismus. J Oral Maxillofac Surg 1990; 48(9):945-52. doi: 10.1016/0278-2391(90)90007-o [Crossref] [ Google Scholar]
- Daniels SE, Goulder MA, Aspley S, Reader S. A randomised, five-parallel-group, placebo-controlled trial comparing the efficacy and tolerability of analgesic combinations including a novel single-tablet combination of ibuprofen/paracetamol for postoperative dental pain. Pain 2011; 152(3):632-42. doi: 10.1016/j.pain.2010.12.012 [Crossref] [ Google Scholar]
- Trindade PA, Giglio FP, Colombini-Ishikiriama BL, Calvo AM, Modena KC, Ribeiro DA. Sublingual ketorolac and sublingual piroxicam are equally effective for postoperative pain, trismus, and swelling management in lower third molar removal. Oral Surg Oral Med Oral Pathol Oral Radiol 2012; 114(1):27-34. doi: 10.1016/j.tripleo.2011.05.027 [Crossref] [ Google Scholar]
- Gillis JC, Brogden RN. Ketorolac A reappraisal of its pharmacodynamic and pharmacokinetic properties and therapeutic use in pain management. Drugs 1997; 53(1):139-88. doi: 10.2165/00003495-199753010-00012 [Crossref] [ Google Scholar]
- Nørholt SE. Treatment of acute pain following removal of mandibular third molars Use of the dental pain model in pharmacological research and development of a comparable animal model. Int J Oral Maxillofac Surg 1998; 27 Suppl 1:1-41. doi: 10.1016/s0901-5027(98)80001-5 [Crossref] [ Google Scholar]
- Gazal G, Al-Samadani KH. Comparison of paracetamol, ibuprofen, and diclofenac potassium for pain relief following dental extractions and deep cavity preparations. Saudi Med J 2017; 38(3):284-91. doi: 10.15537/smj.2017.3.16023 [Crossref] [ Google Scholar]
- Jain N, Maria A. Randomized double blind comparative study on the efficacy of Ibuprofen and aceclofenac in controlling post-operative sequelae after third molar surgery. J Maxillofac Oral Surg 2011 Jun; 10(2):118-22. doi: 10.1007/s12663-011-0198-9 [Crossref] [ Google Scholar]
- Walton GM, Rood JP, Snowdon AT, Rickwood D. Ketorolac and diclofenac for postoperative pain relief following oral surgery. Br J Oral Maxillofac Surg 1993; 31(3):158-60. doi: 10.1016/0266-4356(93)90115-d [Crossref] [ Google Scholar]
- Antunes AA, Avelar RL, Martins Neto EC, Frota R, Dias E. Effect of two routes of administration of dexamethasone on pain, edema, and trismus in impacted lower third molar surgery. Oral Maxillofac Surg 2011; 15(4):217-23. doi: 10.1007/s10006-011-0290-9 [Crossref] [ Google Scholar]
- Alcântara CE, Falci SG, Oliveira-Ferreira F, Santos CR, Pinheiro ML. Pre-emptive effect of dexamethasone and methylprednisolone on pain, swelling, and trismus after third molar surgery: a split-mouth randomized triple-blind clinical trial. Int J Oral Maxillofac Surg 2014; 43(1):93-8. doi: 10.1016/j.ijom.2013.05.016 [Crossref] [ Google Scholar]
- Carlsen O, Alexandersen V. Radix entomolaris: identification and morphology. Scand J Dent Res 1990; 98(5):363-73. doi: 10.1111/j.1600-0722.1990.tb00986.x [Crossref] [ Google Scholar]
- Olmedo MV, Gálvez R, Vallecillo M. Double-blind parallel comparison of multiple doses of ketorolac, ketoprofen and placebo administered orally to patients with postoperative dental pain. Pain 2001; 90(1-2):135-41. doi: 10.1016/s0304-3959(00)00396-1 [Crossref] [ Google Scholar]