Avicenna J Dent Res. 13(3):86-91.
doi: 10.34172/ajdr.2021.17
Original Article
Plaque Removal Efficacy of Chewing Apples and Tooth-Brushing: A Comparative Cross Over Clinical Study
Farzad Mojarad 1  , Niloufar Entezari Moghaddam 2, * , Maryam Farhadian 3 , Bahar Ahmadi 2 , Parviz Torkzaban 4
, Niloufar Entezari Moghaddam 2, * , Maryam Farhadian 3 , Bahar Ahmadi 2 , Parviz Torkzaban 4
Author information:
1DDS, Associated Professor of Pediatric Dentistry, Department of Pediatric Dentistry, Faculty of Dentistry, Hamadan University of Medial Sciences, Hamadan, Iran.
2DDS, Post Graduate Student of Pediatric Dentistry, Department of Pediatric Dentistry, Faculty of Dentistry, Hamadan University of Medial Sciences, Hamadan, Iran.
3Ph.D. in Biostatistics, Research Center for Health Sciences, Department of Biostatistics, School of Public Health, Hamadan University of Medical Sciences, Hamadan, Iran.
4DDS, Professor of Periodontology, Department of Periodontics, Faculty of Dentistry, Hamadan University of Medial Sciences, Hamadan, Iran.
Abstract
Background: The best and the most reliable methods to manage the dental plaque are still mechanical procedures. It has been traditionally recommended that a firm fruit such as an apple be eaten to minimize caries and control plaque at the end of a meal. However, several studies have reported contradictory findings about the microbial plaque function of the apples. Some studies, for instance, have found that apples contain sugar and, therefore, can cause plaque growth; some other researches, on the other hand, have shown that they have the potential to decrease plaque due to their mechanical plaque removal function. This study, therefore, aimed to compare the effects of apple-chewing method and that of tooth-brushing one on plaque removal.
Methods: The study group included 48 healthy dental students with good oral health status, who were randomly selected to participate in this comparative, crossover clinical study. First, they were asked to brush their teeth or eat an apple. After 2 weeks, the experiment was repeated with the order reversed. Plaque indexes (PIs) were determined as before brushing/apple eating (baseline, B), immediately afterward (A), and 24 hours afterward (24).
Results: Over time, there was a significant shift in the plaque index pattern between the groups (P value<0.001) but this discrepancy, in general, was not significant between the group using apple and the one using toothbrush (P value =0.495), as well as between the group using yellow apples, and the ones using red apples or the toothbrushes (P value =0.768).
Conclusions: Comparing the two plaque control methods, it was found they were extremely similar; however, chewing yellow apples was discovered to be more effective method in reducing dental plaque than chewing red apples or using toothbrushes.
Keywords: Dental plaque, Dietary fiber, Health education, Dental
Copyright and License Information
© 2021 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Citation: Mojarad F, Entezari Moghaddam N, Farhadian M, Ahmadi B, Torkzaban P. Plaque removal efficacy of chewing apples and tooth-brushing: a comparative cross over clinical study. Avicenna J Dent Res. 2021;13(3):86-91. doi: 10.34172/ajdr.2021.17.
Background
Highlights
Periodontal disease refers to a disease that afflicts the tissue holding the teeth in place. It is normally caused by improper brushing and flossing practices that facilitate the build-up of dental plaque and harden the sticky biofilm of bacteria on the teeth. Periodontal disease may cause some dental health problems such as sore and bleeding gums in advanced phases, painful difficulty with chewing, and even tooth loss. The mildest type of periodontal disease is gingivitis (1). Mechanical interventions such as tooth-brushing with toothpaste and interdental cleaners are still considered as the most effective and the least difficult methods for plaque control (2).Different products such as dental floss, interdental toothbrush and toothpick have been designed to access these areas but, presently, dental floss is the most popular one. Despite recent advancements in pharmacological therapies, mechanical plaque removal is still a primary method for plaque regulation. The combined use of toothbrushes and dental floss has been accepted as the safest way to prevent gingivitis and dental plaque (1,2).People have been traditionally recommended to use a firm fruit such as apple at the end of their meal in order for minimizing caries and controlling plaque. Chewing apples on a daily basis, therefore, is still widely used as a way of cleaning the teeth. After ingestion of carbohydrates, apples stimulate the flow of saliva and alkaline, which neutralizes the acid produced by dental plaque. Apples can induce plaque growth due to their sugar content. On the other hand they decrease plaque due to mechanical plaque removal (3). Since the important role of apples in maintaining general health as well as their phytochemical and anti-cancer content have already been acknowledged, their frequent use is generally recommended nowadays. Apples can also prevent the progression and worsening of periodontal disease due to their antioxidant properties (4).The potential of solid foods in plaque removal in gingival margins and interdental areas are as effective as tooth brushing however this effect is controversial in other areas (3). Generally, apples play an important role in health, especially in oral health, and as a popular saying goes, “an apple a day, keeps the doctor away” (5).So far, several studies have been conducted to examine the effects of apples on microbial plaque, which generated conflicting results. A study, for instance, has found that apples stimulate plaque growth due to their sugar content; whereas another research has discovered that they decrease plaque through mechanical removal of plaque (6).This study, therefore, aimed to compare the effects of chewing the apples and brushing the teeth on dental plaque, to examine the dental surfaces affected by plaque removal methods – especially in children – and determine the highest and lowest amount of plaque, and to use the study results for introducing preventive procedures for controlling dental plaque.
Materials and Methods
The present clinical trial was carried out after obtaining the approval from the Iranian Registry of Clinical Trials
Participants
A total of 48 healthy dental students (24 females and 24 males) aged 20-25 from Hamadan University of Medical Sciences were randomly selected after obtaining informed consent (See Figure 1); They all had good oral hygiene (plaque index below twenty percent) and at least twenty-four permanent teeth (excluding third molars) (7). Exclusion criteria of this study included: smoking, the presence of any orthodontic appliances, fixed or removable prosthesis, the use of antibiotics and antiseptic mouthwash during the past 3 months, and the presence of any systemic or saliva-reducing medications that could influence saliva development or composition.
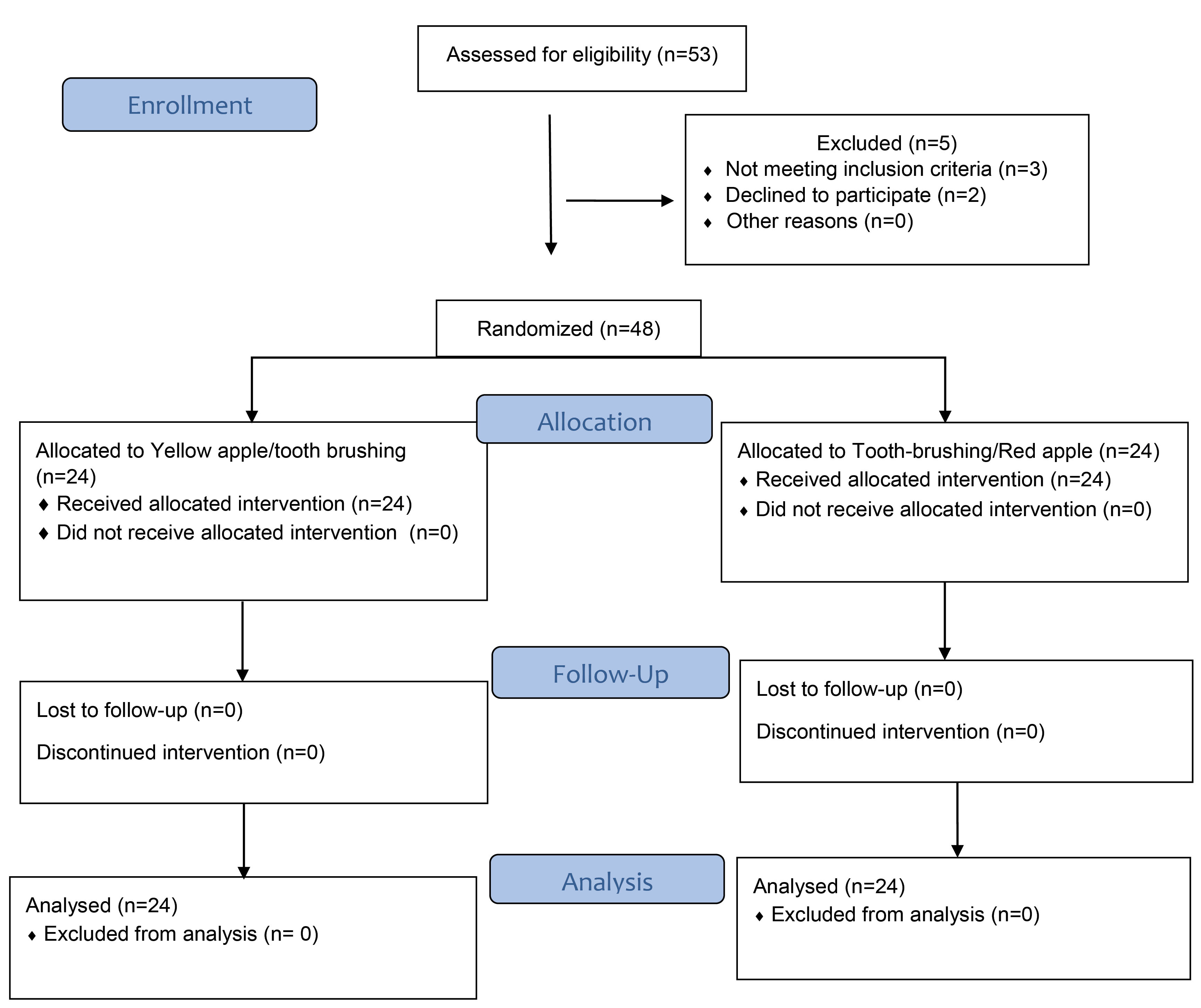
Figure 1.
Flowchart of the Study.
.
Flowchart of the Study.
Study Design
This clinical trial was designed to be open-label and, therefore, students and clinicians were aware of the treatment allocation. Before carrying out this cross-over study, professional prophylaxis was performed for all participants; then baseline plaque index was calculated (Figure 2A, B), and dental plaque was measured in the morning. Participants were not permitted to use routine health control procedures at each stage (only 24 hours after the start of each phase). Consuming alcohol or foods that could dissolve plaque mechanically were also prohibited but they could maintain their routine eating habits.
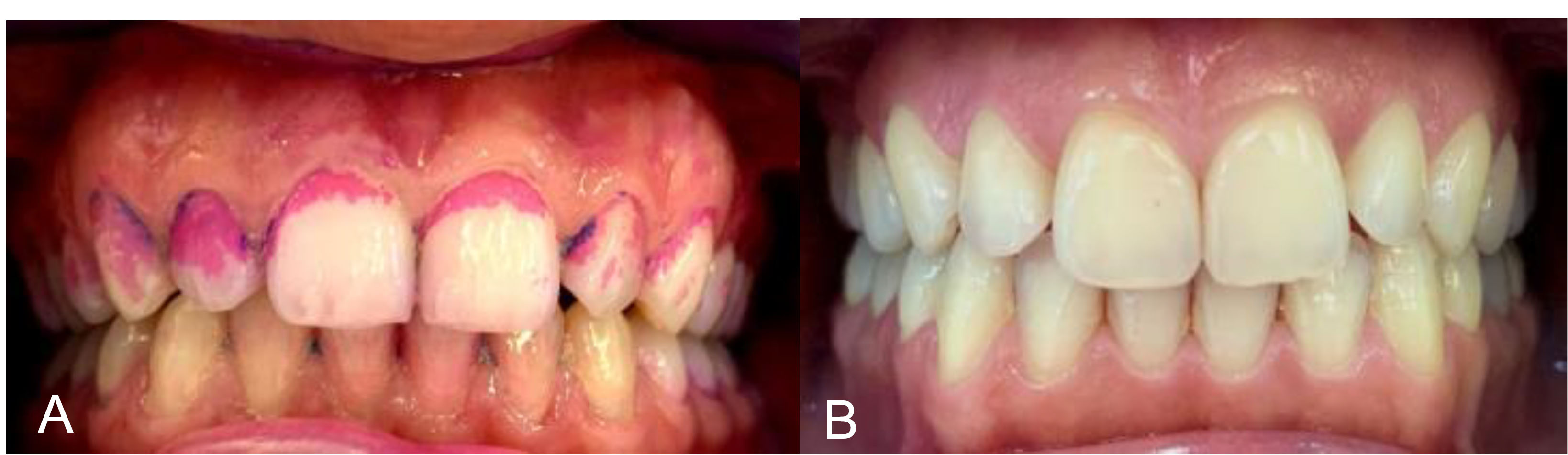
Figure 2.
(A) Plaque Index at Baseline, (B) Plaque Index After Professional Prophylaxis.
.
(A) Plaque Index at Baseline, (B) Plaque Index After Professional Prophylaxis.
To do the trial, a medium Oral-B 123 Classic Care® toothbrush was employed, and the tooth brushing was performed using the Bass technique and tap water with no toothpaste. The medium toothbrush was selected since the participants were dental students and were familiar with the proper brushing technique to avoid damage to the periodontal structure. The brushing time took about 2 minutes (each quarter is 30 seconds) (6). Apple chewing was performed without any constraints; that is, participants were allowed to eat the apples with skin using both sides of their mouth. Two kinds of apples (i.e., yellow and red apples) weighing around 160 g were randomly selected and eaten by participants.
The two study groups were labeled as group A whose members were asked to brush the teeth/chew red apple), and group B whose members were assigned to chew yellow apple/brush the teeth). The 48 participants were divided into two classes and randomly added to each one of the groups. The plaque index was calculated three times:
The plaque index was calculated three times: 1. Baseline 2. Immediately after plaque removal. 3. twenty-four hours after the removal.
The O’Leary index (8)and disclosing tablets were used to record dental plaque, and the participants were asked to hold TePe Plaqsearch® tablets in their mouth for 30 seconds so that the tablets could be mixed with saliva, and spread over the dental surfaces by the tongue.
The O’Leary index was calculated using follow the following formula:
In this study, the highest and the lowest tooth surfaces affected by plaque removal techniques were also documented. To this end, 11, 15, 31, 35 and 45 teeth were measured. Each tooth surface was divided into three vertical parts, namely mesiobuccal, mid-buccal, and distobuccal. Maximum and minimum numbers of plaque values (9) were recorded in the chart by comparing time 0 with 24 hours later observationally.
Statistical Analysis
First, the values required to determine the sample size were obtained from similar studies (6). The power of the study was kept at 0.80, and the confidence level was kept at 95%. Estimated sample size was 24 in each experimental group. Then data analyses were performed using SPSS software version 21. To analyze the data, descriptive statistical methods and statistical tests such as one-way analysis of variance and t-test were adopted. Significance level in all tests were equal to 0.05.
Results
Our study results showed that period and carryover effects were not statistically significant (P value=0.310); therefore, the one-way repeated measure analysis (RM-ANOVA) was adopted to compare the groups. The findings were as follows:
Over time, there was a significant trend of changes in the plaque index (P value <0.001) (Table 1); this difference, however, was not significant between the apple group and the tooth-brushing one (P value =0.495), or even between tooth-brushing group and the group whose members chewed yellow and red apples (P value =0. 768) (Table 2).
Table 1.
Plaque Indices at Baseline, Immediately After Manual Tooth-Brushing and After Chewing Red and Yellow Apple, and 24 Hours After the Activity
|
|
PI-Base line
|
PI-Immediately
|
PI-24h
|
P
Value*
|
| Red apple |
14.22±4.78 |
12.54±3.88 |
14.47±4.27 |
<0.001 |
| Yellow apple |
14.92±4.72 |
11.57±3.79 |
14.08±4.45 |
<0.001 |
| Tooth-brushing |
14.60±4.7 |
12.16±3.20 |
14.31±3.58 |
<0.001 |
Table 2.
Test of Between Subjects Effect
|
Between Group Comparison
|
P
Value
|
| Apples - tooth-brushing |
0.495 |
| Red apple - yellow apple - tooth-brushing |
0.768 |
Note. Each term in the model, plus the model as a whole are tested for its ability to account for variation in the dependent variable.
The amount of plaque indexes in the group which was measured immediately, was lower than other groups. The two methods were found to be extremely similar in removing dental plaque (Figure 3); however, chewing yellow apple in immediate time and 24 hours after the consumption slightly had less plaque index values compared to brushing teeth and chewing red apple (Figure 4).
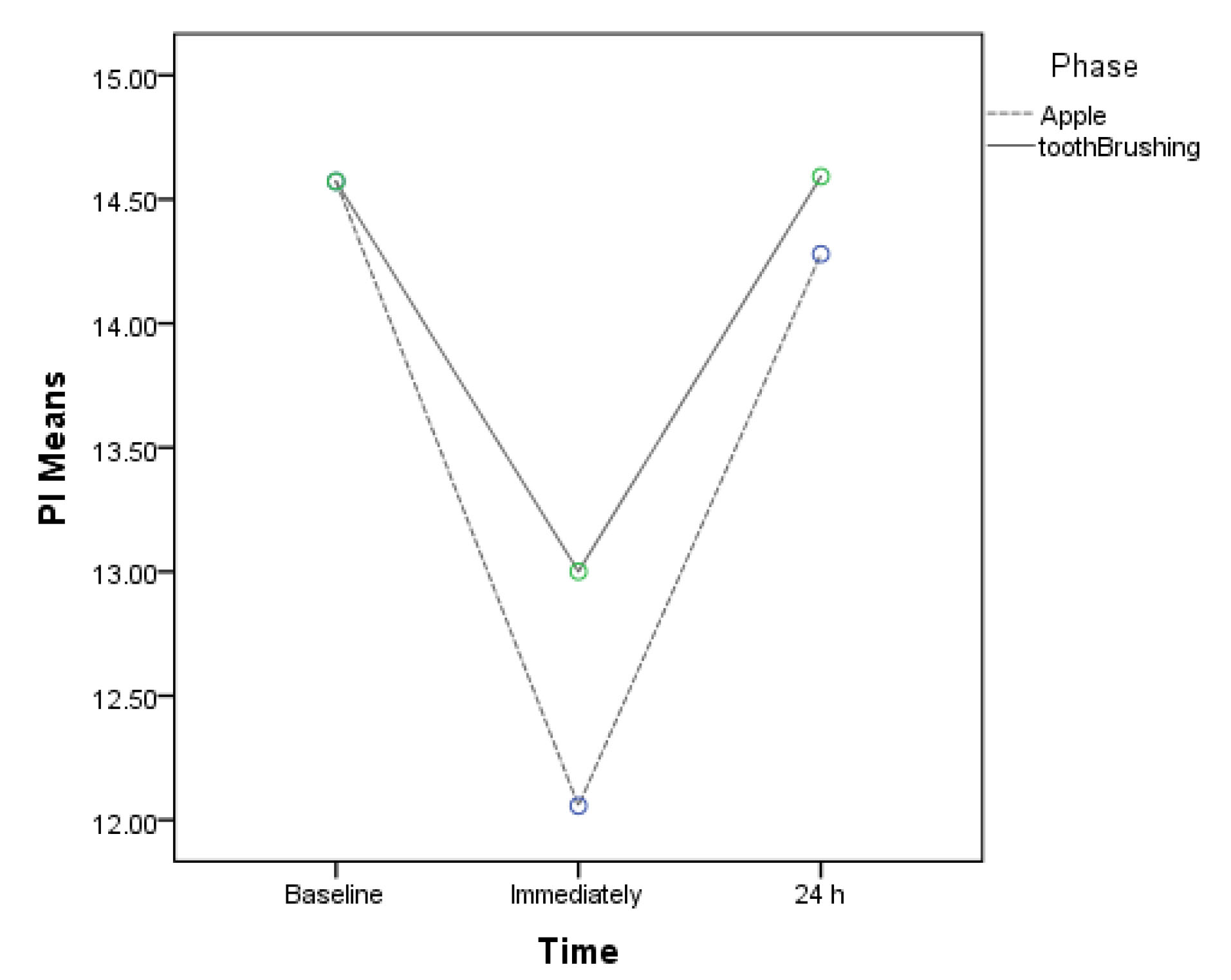
Figure 3.
Comparison Between Two Methods (Tooth-brushing-Apple Chewing).
.
Comparison Between Two Methods (Tooth-brushing-Apple Chewing).
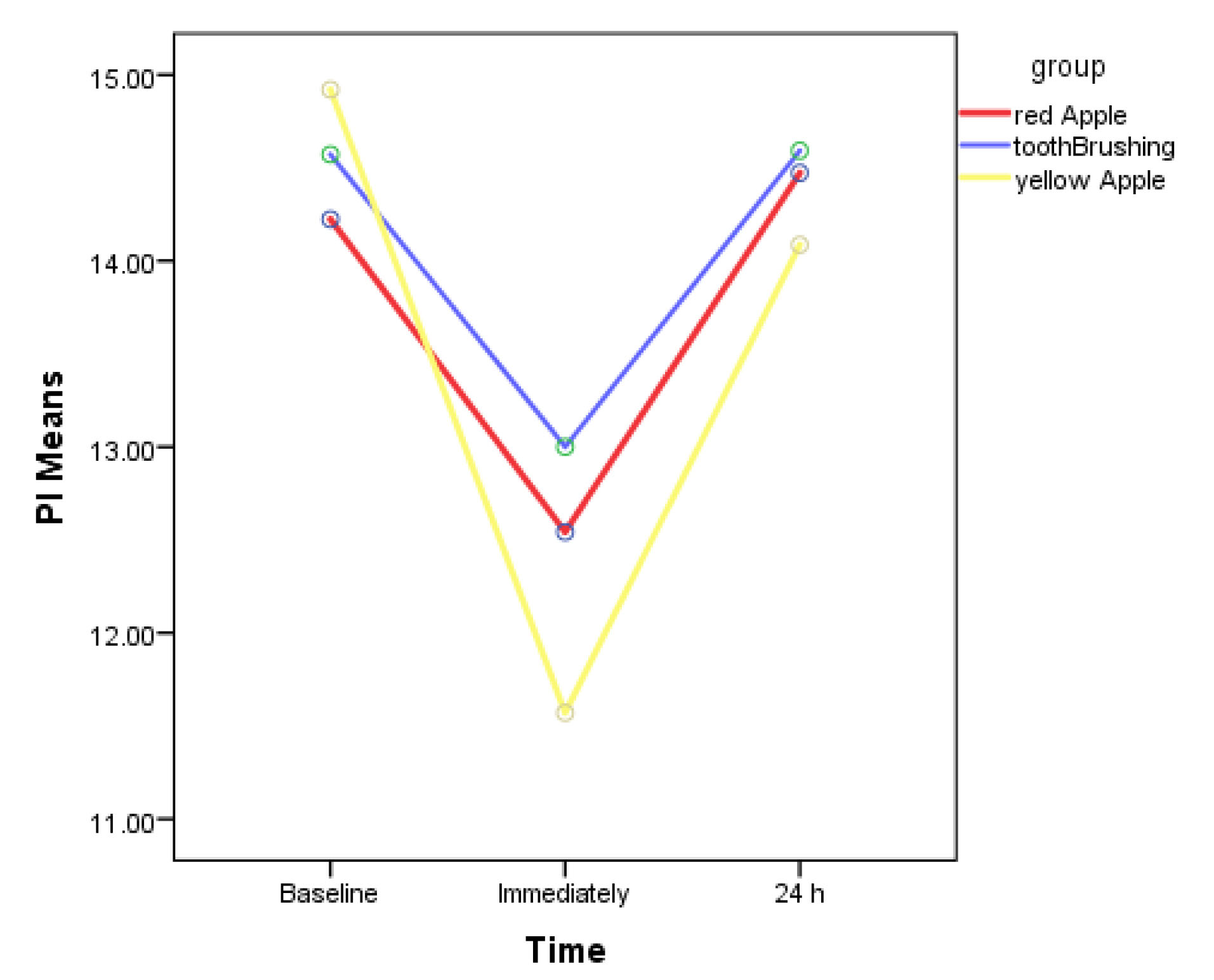
Figure 4.
Comparison Between Tooth-Brushing, Red and Yellow Apple.
.
Comparison Between Tooth-Brushing, Red and Yellow Apple.
Comparing the changes in plaque building up on three vertical zones showed that the maximum reduction occurred in the mesiobuccal surface (43.8% in apple and 54.2% in tooth-brushing) (Table 3), and the minimum reduction took place in the mid-buccal surface (72.9% in apple and 66.7% in tooth-brushing) in all selected teeth (Table 4).
Table 3.
Maximum Surface of Plaque Removal of Selected Teeth
|
Tooth Number
|
Apple
|
Tooth-Brushing
|
|
Distobuccal
|
Mesiobuccal
|
Mid Buccal
|
Distobuccal
|
Mesiobuccal
|
Mid Buccal
|
| 11 |
1 |
1 |
5 |
1 |
7 |
2 |
| 15 |
2 |
5 |
4 |
1 |
1 |
0 |
| 31 |
3 |
4 |
5 |
2 |
9 |
2 |
| 35 |
1 |
7 |
3 |
2 |
6 |
8 |
| 45 |
0 |
4 |
3 |
4 |
3 |
0 |
| Total |
7 |
21 |
20 |
10 |
26 |
12 |
| 14.5% |
43.8% |
41.7% |
20.8% |
54.2% |
25.0% |
Table 4.
Minimum Surface of Plaque Removal of Selected
|
Tooth Number
|
Apple
|
Tooth-Brushing
|
|
Distobuccal
|
Mesiobuccal
|
Mid Buccal
|
Distobuccal
|
Mesiobuccal
|
Mid Buccal
|
| 11 |
1 |
1 |
16 |
2 |
2 |
8 |
| 15 |
3 |
0 |
7 |
1 |
1 |
1 |
| 31 |
0 |
1 |
11 |
1 |
2 |
6 |
| 35 |
3 |
2 |
0 |
1 |
3 |
10 |
| 45 |
2 |
0 |
1 |
1 |
1 |
8 |
| Total |
9 |
4 |
35 |
6 |
9 |
33 |
| 18.8% |
8.3% |
72.9% |
12.5% |
18.8% |
66.7% |
Discussion
The present study aimed to determine whether the order of tooth-brushing and apple-chewing or the reverse order could affect dental plaque, to introduce the most effective method depending on the type of apple used (yellow or red), to investigate tooth surfaces affected by this method with the most or least plaque removal, and to examine the effectiveness of the apples in controlling plaque using a plaque control method for young children.
The most known cause of gingivitis is microbial plaque and, therefore, its removal from the tooth surface is one of the most effective measures to prevent and treat this disease. Plaque, if left untreated, may affect the supporting tooth structures such as gums, periodontal ligaments as well as alveolar bone, and ultimately cause tooth loss (10,11). The given situations exert adverse effects on the quality of life, speech, nutrition, and self-confidence. Gingivitis is regarded as the most common and mildest periodontal disease caused by plaque which is deposited on the surface of the tooth and surrounding tissue. The mechanical and chemical methods to eliminate microbial plaque and prevent its formation are one of the well-known methods for preserving oral health. Microbial plaque control is at the core of all dental therapies. Brushing is the most common and efficient mechanical plaque removal process that can prove effective in preventing periodontal disease and caries only if it is performed regularly (12). For majority of people, apples are “natural toothbrush” having been used for many years. Since apple has thick skin, is rich in fiber, and has suitable texture, it can function as a natural toothbrush to clean the teeth and remove the plaque that is placed on them (13). So far, several studies have yielded conflicting results on the effects of apples on microbial plaque; for example, a study has found that apples encourage plaque growth due to their sugar content; while another research has discovered that they decrease plaque through mechanical removal of plaque.
According to our first study finding, and after comparing the two methods for plaque control, it was found that both methods displayed extremely similarity in removing dental plaque over time; however, chewing yellow apples was discovered to be slightly more effective than tooth-brushing or chewing red apples in terms of plaque reduction potential. More beneficial effects produced by chewing yellow apple compared to red one could be attributed to the thicker skin of the yellow apple, which was in agreement with the results from the study by Homutová and Blažek where the skin thickness of different apples had been compared (14). The effects of apples on oral health and bacterial control have already been examined in several studies. However, our findings contradicted the results from the study by Rubido et al However, our findings contradicted the results of a study by Rubido et al (6), in which it was found that chewing apples fail to eliminate dental plaque and in fact helped to increase the plaque(6). Possible reason is that chewing apple induces saliva flow, and salivary protein pellicle on the enamel can be stained with erythrosine. This experiment demonstrated that apples must contain some component capable of adhering to the tooth surface that are stained with erythrosine. Differences in the results from various studies assessing the effects of mechanical plaque removal by chewing apples may be associated with several factors such as the age of subjects, the measured teeth, the type of apples used, the quantity of apples consumed, or the use of peeled or unpeeled apples.
In our study, the highest and lowest dental surfaces affected by plaque removal methods were also evaluated. To this end, each selected tooth surface was divided into three vertical areas and, then, the areas were examined. The highest dental plaque reduction was detected in mesiobuccal, whereas the lowest one was observed in the mid-buccal surface. Our findings in this regard were consistent with the results from a study by Kalsi et al in India (9). In the current research, both plaque removal techniques were discovered to be effective in reducing plaque count; and 24 hours later, the plaque index was observed to display a slight decrease for yellow-apple-chewing group compared to the group chewing red apple or the one using toothbrush. Our study faced some limitations requiring due consideration. For one thing, it was hard to generalize about our findings and apply them to other age groups or other populations with the same age range but with different socio-cultural backgrounds.
Conclusions
In conclusion, chewing apples was found to have mechanical plaque removal effect. In our evaluation of plaque reducing effects of apple-chewing and tooth-brushing methods, it was also demonstrated that both methods were capable of producing extremely similar favorable effects on plaque after a period of time when at least 24 hours was spent on implementing them.
Conflict of Interest Disclosures
The authors declare that they have no conflict of interests.
Ethical Statement
This study was registered at the Iranian Registry of Clinical Trials website (identifier: IRCT20191214045728N1).
Acknowledgments
The authors would like to thank all students who agreed to participate in this study.
References
- Torkzaban P, Arabi SR, Seyedzadeh Sabounchi S, Roshanaei G. The efficacy of brushing and flossing sequence on control of plaque and gingival inflammation. Oral Health Prev Dent 2015; 13(3):267-73. doi: 10.3290/j.ohpd.a32678 [Crossref] [ Google Scholar]
- Sälzer S, Slot DE, Van der Weijden FA, Dörfer CE. Efficacy of inter-dental mechanical plaque control in managing gingivitis--a meta-review. J Clin Periodontol 2015; 42 Suppl 16:S92-105. doi: 10.1111/jcpe.12363 [Crossref] [ Google Scholar]
- Jenkins GN. Enamel protective factors in food. J Dent Res 1970; 49(6):1318-26. doi: 10.1177/00220345700490062501 [Crossref] [ Google Scholar]
- Hyson DA. A comprehensive review of apples and apple components and their relationship to human health. Adv Nutr 2011; 2(5):408-20. doi: 10.3945/an.111.000513 [Crossref] [ Google Scholar]
- Soltani P. An apple a day keeps the dentist away: fact or fiction? (a brief review on effects of apple on oral health). Sch J Dent Sci 2015; 2(4):293-5. [ Google Scholar]
- Rubido S, García-Caballero L, Abeleira MT, Limeres J, García M, Diz P. Effect of chewing an apple on dental plaque removal and on salivary bacterial viability. PLoS One 2018; 13(7):e0199812. doi: 10.1371/journal.pone.0199812 [Crossref] [ Google Scholar]
- Lindhe J, Wicén P-O. The effects on the gingivae of chewing fibrous foods. J Periodontal Res 1969; 4(3):193-201. doi: 10.1111/j.1600-0765.1969.tb01966.x [Crossref] [ Google Scholar]
- Newman M, Takei H, Klokkevold P, Carranza F. Newman and Carranza’s Clinical Periodontology. Saunders; 2018.
- Kalsi DS, Sood A, Sharma V. Relative additional mechanical plaque removing effect of fibrous food (apple) on different sites of selected teeth. Indian J Dent Sci 2015; 7(2):9-12. [ Google Scholar]
- Chapple IL, Van der Weijden F, Doerfer C, Herrera D, Shapira L, Polak D. Primary prevention of periodontitis: managing gingivitis. J Clin Periodontol 2015; 42 Suppl 16:S71-6. doi: 10.1111/jcpe.12366 [Crossref] [ Google Scholar]
- Di Benedetto A, Gigante I, Colucci S, Grano M. Periodontal disease: linking the primary inflammation to bone loss. Clin Dev Immunol 2013; 2013:503754. doi: 10.1155/2013/503754 [Crossref] [ Google Scholar]
- Prabhuswamy B, Mallikarjun N, Nagaraj K, Simpi B. Comparative evaluation of anticariogenic activity of commercially available herbal dentifrices. SRM J Res Dent Sci 2018; 9(2):58-62. doi: 10.4103/srmjrds.srmjrds_31_17 [Crossref] [ Google Scholar]
- Apples and the teeth--”nature’s toothbrush” reappraised. Br Med J 1977;1(6069):1116. 10.1136/bmj.1.6069.1116.
- Homutová I, Blažek J. Differences in fruit skin thickness between selected apple (Malus domestica Borkh) cultivars assessed by histological and sensory methods. Hortic Sci 2006; 33(3):108-13. doi: 10.17221/3747-hortsci [Crossref] [ Google Scholar]