Avicenna J Dent Res. 13(1):23-27.
doi: 10.34172/ajdr.2021.05
Original Article
Evaluation of Stylohyoid Complex Patterns on Digital Panoramic Radiographs in the Local Population in Ilam, Iran
Vida Arzani 1, *  , Pardis Ahmadi 2
, Pardis Ahmadi 2
Author information:
1Assistant Professor, Iran University of Medical Sciences, Tehran, Iran
2Dentist
*
Correspondence to Vida Arzani, Assistant Professor, Iran University of Medical Sciences, Tehran, Iran Tell: +982166915454; Email:
vidaarzani@yahoo.com
Abstract
Background: Stylohyoid ligament ossification is a complication that is repeatedly and accidentally observed on panoramic radiographs and may be the cause of some symptoms. Accordingly, awareness of this incidence enables the clinicians in the accurate diagnosis of head and neck pains while avoiding unneeded therapy.
Methods: This was a descriptive cross-sectional study. The number of samples was 196 people who referred to an oral and maxillofacial radiology center in Ilam in 2020. Information was completed by a checklist which consisted of two parts, including a questionnaire (age, gender, history of maxillofacial trauma, history of maxillofacial surgery, and pregnancy) and a second part (including the ossification of the stylohyoid complex, its length, involved side, and the process category according to Langlais classification). Differences between the groups were compared by Student’s t test, Welch’s t test, or chi-square test (P<0.05).
Results: The results revealed the influence of age on the calcification and elongation patterns of the styloid process while no significant association was found between gender and elongation and calcification patterns. The ossification of the stylohyoid complex was unilateral and bilateral in 24 (40.6%) and 35)59.3%) patients. Finally, the ossification of the stylohyoid complex was bilateral in 17 patients (48.6%) aged 40-59 years.
Conclusions: The evaluation of stylohyoid complex patterns using panoramic radiography is essential, especially in patients with related symptoms. Further studies are needed to completely understand the underlying mechanism of the ossification of the styloid process and to assess different types of the styloid process and the relation between them in patients.
Keywords: Stylohyoid patterns, Panoramic, Radiography
Copyright and License Information
© 2021 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Citation: Arzani V, Ahmadi P. Evaluation of stylohyoid complex patterns on digital panoramic radiographs in the local population in Ilam, Iran. Avicenna J Dent Res. 2021;13(1):23-27. doi: 10.34172/ajdr.2021.05.
Background
Highlights
The styloid process is a thin, sharp protrusion of temporal bone. The elongation and ossification of this process and its surrounding ligaments result in pressure on the surrounding neurovascular bundle, causing symptoms such as severe pain and limited neck movement, and dysphagia. All these symptoms can be associated with a syndrome called Eagle, a term first coined in 1937 by Watt. W. Eagle. In this context, it is important for anthropologists and anatomists to be able to decipher the morphometry of the styloid process (1).
In Eagle syndrome, which is primarily driven by recurrent pain in the face and oropharynx, part of the stylohyoid ligament is associated with an increase in the length of this process of mineralization, which puts pressure on carotid arteries and cranial nerves. Thus, awareness of this syndrome will enable the clinicians in the accurate diagnosis of head and neck pains while avoiding unneeded therapy (2,3). Either physical or radiographical examination is used for diagnosing Eagle syndrome. In particular, the panoramic radiograph is most commonly employed for identifying the styloid process elongation. Several hypotheses are suggested to explain this bizarre syndrome although the precise etiology underlying the elongation/calcification of the styloid process requires thorough elucidation. In addition, the recognition of size changes in this structure can be used as an indicator for predicting bone density and high serum calcium concentrations, which are effective in the physical health of aged people (4).
The main cause of the ossification of this ligament has not been well understood. The hypotheses put forward to explain this condition include the inheritance-based model of an increase in the length of the styloid process due to the persistence of Reichert’s cartilage (a component of the styloid process in the fetus), calcification of the styloid process for unknown reasons, and the growth of the bone tissue at the ligament junction with the styloid process (5).
It is also argued that surgical trauma, chronic local stimulation, the presence of mesenchymal components, endocrine disorders during menopause in women, and trauma and mechanical stress during development lead to bone hyperplasia in the stylohyoid complex. A previous study suggested a link between the process length and age attributing to the enhancement of serum-calcium concentrations (6).
Although some argue that it is caused by ligament degeneration and deposition of calcium salts in fibrous tissues, others claim that malformations are due to the direct ossification of cartilage cells that reside in the ligaments of adults (5,6).
The length of the styloid process typically ranges between 0.5 and 2.5 cm (7). On the other hand, ligament ossification occasionally appears on the panoramic radiographs of asymptomatic patients. In one study, the prevalence of styloid ossification with a length of more than 30 mm was equal to 18% and the prevalence of styloid elongation was up to 28% (8). In the study by Shaik et al (9), the prevalence of styloid elongation was estimated to be 18.2%, of which 93% were bilateral.
Stylohyoid ligament ossification is commonly found on panoramic radiographs, and the stylohyoid ligament may be somewhat calcified in different people of all ages (10).
According to Langlais classification (11), the types of elongation and the pattern of process calcification on each side are as follows:
-
Classification based on the type of elongation: Types 1 (elongated), 2 (pseudoarticulated), and 3 (segmented);
-
Classification based on the pattern of calcification: Patterns A (marginal calcification), B (partial calcification), C (nodular calcification), and D (complete calcification).
Considering that typically panoramic radiography is the technique of choice for most dental treatments because of its low dose of radiation, cost-effectiveness, and the rapidity of the examination of the jaw and teeth, this technique is widely used by dentists as the gold standard despite the criticism that caution should be exercised when asserting normal and abnormal findings in the radiograph that occasionally needs to be studied and followed up (12). To accurately diagnose and avoid misdiagnosis or faulty treatment plans, it is crucial to assess the prevalence of the elongated styloid process and/or the ossification of the stylohyoid ligament in the local population. The aim of the present study was to evaluate the patterns of the stylohyoid complex through panoramic radiography using morphology and calcification types in both genders with different ages in Ilam, Iran.
Materials and Methods
This descriptive cross-sectional study was performed in a dental clinic for oral and maxillofacial radiology in Ilam. The statistical population consisted of 196 randomly selected men and women who came to the clinic. The applied criteria for selecting participants included no pregnancy in women, no cosmetic or reconstructive facial surgery, the age range of over 20 years, no history of head and face trauma, and no maxillofacial developmental disorders. The evaluation of variables was performed after the exclusion of incomplete data, belonging to patients with either defect in the file or failure for meeting any of the inclusion conditions. Panoramic radiographs presenting no perceptible stylohyoid process from the base of the skull were excluded as well.
A checklist was prepared based on available literature. This checklist consisted of a questionnaire (including age, gender, history of maxillofacial trauma, history of maxillofacial surgery, and pregnancy) and a second part (including the ossification of the stylohyoid complex, its length, the involved side, and the process category according to Langlais classification). After performing panoramic radiography, patients were reported with or without the ossification of the stylohyoid complex. The Planmeca ProMax Digital Panoramic X-ray unit (Planmeca Inc., Helsinki, Finland) and Planmeca Romexis software were used to assess the images. The linear measurement tool of Romexis software was applied to conduct the measurements. Each of the observations and measurements was done by a dental student and a board certified oral and maxillofacial radiologists for more reliability.
In this study, cases were recorded as the ossification of the stylohyoid ligament when the length of the styloid process from the base of the skull to the tip of the process was more than 25 mm (12). The method of measuring the length of this ligament is shown in Figures 1 and 2.
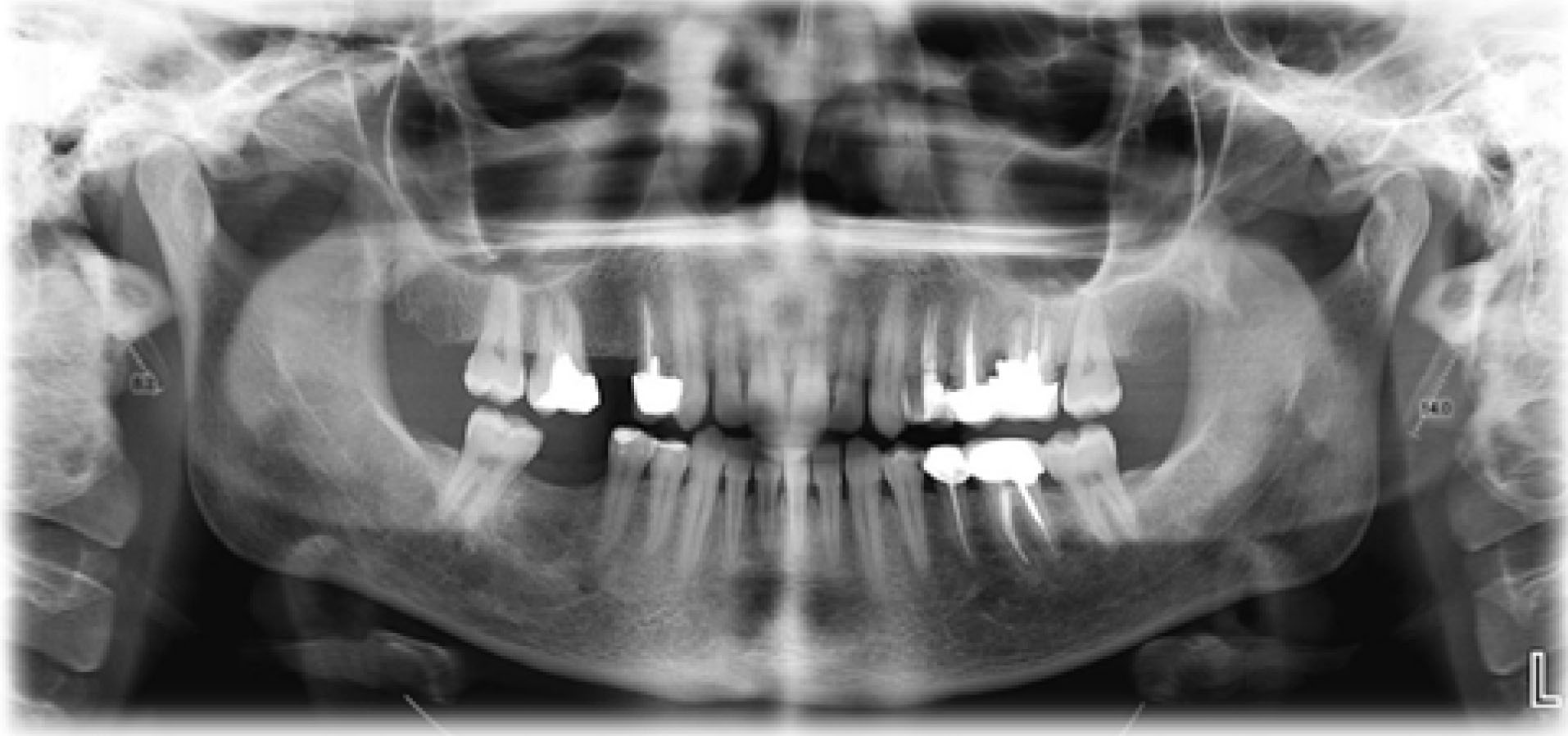
Figure 1.
The length of styloid process is measured according to the image from the base of the skull to the tip of the process.
.
The length of styloid process is measured according to the image from the base of the skull to the tip of the process.
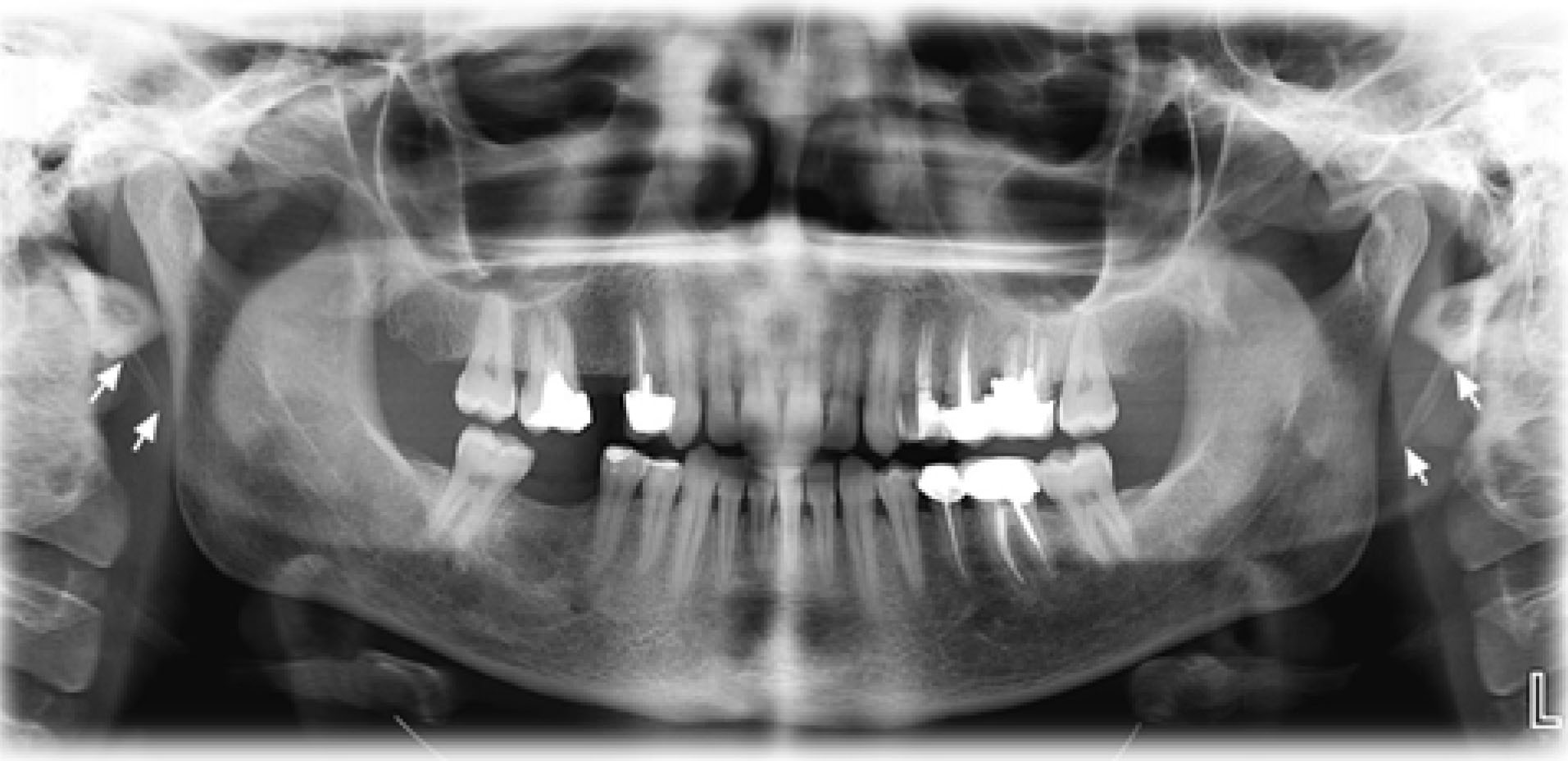
Figure 2.
The tips of the arrows show the beginning and end of the process.
.
The tips of the arrows show the beginning and end of the process.
In quantitative variables, the mean was used to describe the average value of the data, and the standard deviation (SD) was employed to describe the dispersion or closeness of the item to the mean. Kolmogorov-Smirnov test was used for normal data distribution and chi-square and t test were applied to compare quantitative variables. In qualitative variables, distribution and frequency were utilized to describe data. Welch’s t test, which is insensitive to the equality of variances regardless of whether the sample sizes are similar, was used to compare two groups. The Student t-test was applied for statistically comparing the differences between the means of paired variables. The analysis of data was performed using SPSS 22 software (Statistical Package for the Social Sciences, version 22) at a significance level of 0.05.
Results
Based on data in Table 1, the gender ratio of the studied population was 1.3:0.7 with a preponderance of males (111 male individuals, 56.6%: 85 female individuals, 43.4%). The ossification of the stylohyoid complex was found in 59 patients (30.1%), of which 34 (57.6%) and 25 (42.4%) cases were males and females, respectively. There was no significant relationship between gender and the incidence of the ossification of the stylohyoid complex (P > 0.05).
Table 1.
Frequency of Stylohyoid Complex Ossification (SCO) in the population (n 196) studied relative to gender
Ossification
Gender
|
Incidence of ossification of stylohyoid ossification
|
Total
|
Yes
Frequency (Percentage)
|
No
Frequency (Percentage)
|
| Male |
34 (57.6) |
77 (56.2) |
111 (56.6) |
| Female |
25 (42.4) |
60 (43.8) |
85 (43.4) |
| Total |
59 (30.1) |
137 (69.9) |
196 (100) |
|
P=0.854 |
Table 2 presents the frequency distribution of the studied population with 91 (46.4%) subjects in the age range of 40-59 years old, of which 31 cases (34%) had the ossification of the stylohyoid complex. The ossification of the stylohyoid complex was observed in 59 patients (30.1%), of which 12 (20.3%), 31 (52.5%), and 16 (27.1%) cases were under 40 years old, in the age range of 40-59 years old, and more than 60 years old, respectively. The results revealed a significant relationship between age and the incidence of the ossification of the stylohyoid complex (P < 0.05).
Table 2.
Frequency distribution of stylohyoid complex ossification (SCO) in the population (n 196) discriminated by age groups
Ossification
age
|
Incidence of ossification of stylohyoid ossification
|
Total
|
Yes
Frequency (Percentage)
|
No
Frequency (Percentage)
|
| Less than 40 years |
12 (20.3) |
53 (38.7) |
65 (33.2) |
| Between 40 and 59 years |
31 (52.5) |
60 (43.8) |
91 (46.4) |
| More than 60 years |
16 (27.1) |
24 (17.5) |
40 (20.4) |
| Total |
59 (30.1) |
137 (69.9) |
196 (100) |
|
P=0.035 |
Based on the results of ligament length in Table 3, the means of ligament length was 27.15 ± 1.44 mm and 27.02 ± 0.89 mm, in men and women, respectively. No significant relationship was found between gender and the length of the stylohyoid ligament (P > 0.05).
Table 3.
Means of stylohyoid ligament length discriminated by gender
Length
Gender
|
Stylohyoid ligament length
|
|
Yes
|
No
|
|
Mean±Standard deviation
|
Mean±Standard deviation
|
| Male |
15.27±44.1 |
43.22±45.1 |
| Female |
02.27±89.0 |
69.22±36.1 |
|
P=0.243 |
Table 4 presents the mean ± SD of stylohyoid ligament length in different age groups, showing 26.84 ± 1.72 mm, 27.03 ± 1.09 mm, and 27.59 ± 0.59 for individuals under 40, 40-59, and over 60 years old, respectively. Based on the findings, there was a significant relationship between age and the length of the stylohyoid ligament (P < 0.05).
Table 4.
Means of stylohyoid ligament length discriminated by age
Length
Age
|
Stylohyoid Ligament Length
|
|
Yes
|
No
|
|
Mean±Standard deviation
|
Mean±Standard deviation
|
| Less than 40 years |
84.26±72.1 |
49.22±42.1 |
| Between 40 and 59 years |
03.27±09.1 |
73.22±46.1 |
| More than 60 years |
59.27±59.0 |
20.22±25.1 |
|
P=0.035 |
The ossification of the stylohyoid complex was unilateral in 24 patients (40.6%) and bilateral in 35 patients (59.3%). Accordingly, no significant relationship was observed between gender and the unilateral/bilateral involved process (P > 0.05).
On the other hand, the ossification of the stylohyoid complex was bilateral in 17 patients (48.6%) aged 40-59 years. There was a significant relationship between age and the unilateral/bilateral involved process (P < 0.05). According to data in Table 5, the type of elongation was elongated in 41 patients (20.9%) and the pattern of calcification was marginal in 31 patients (15.8%). No significant relationship was detected between gender and type of elongation (P > 0.05). There was also no significant relationship between gender and the calcification pattern (P > 0.05).
Table 5.
Frequency of Stylohyoid Complex Ossification (SCO) in the population (n 196) studied, based on Langlais classification relative to gender
|
Langlais Classification
|
|
Gender
|
Total
|
Significance level
|
|
Male
|
Female
|
|
Frequency (Percentage)
|
Frequency (Percentage)
|
| Type of elongation |
Elongated |
23 (7.20) |
18 (2.21) |
41(9.20) |
498.0 |
| Pseudoarticulated |
3 (7.2) |
0 |
3 (5.1) |
| Segmented |
8 (2.7) |
7 (2.8) |
15 (7.7) |
| Pattern of elongation |
Marginal |
19 (1.17) |
12 (1.14) |
31 (8.15) |
913.0 |
| Partial |
6 (4.5) |
7 (2.8) |
13 (6.6) |
| Nodular |
5 (5.4) |
3 (5.3) |
8 (1.4) |
| Complete |
4 (6.3) |
3 (5.3) |
7 (6.3) |
Based on the obtained data in Table 6, the type of elongation was elongated in 21 patients (23.1%) in the age range of 40-59 years old and the pattern of calcification was marginal in 16 patients (17.6%) of the same age range. Thus, there was no significant relationship between age and type of elongation (P > 0.05). Additionally, no significant relationship was found between age and the calcification pattern (P > 0.05).
Table 6.
Frequency of Stylohyoid Complex Ossification (SCO) in the population (n 196) studied, based on Langlais classification relative to age
|
Langlais Classification
|
|
Age
|
Significance Level
|
|
Less than 40 years
|
Between 40 and 59 years
|
More than 60 years
|
|
Frequency (Percentage)
|
Frequency (Percentage)
|
Frequency (Percentage)
|
| Type of elongation |
Elongated |
9 (8.13) |
21 (1.23) |
11 (5.27) |
115.0 |
| Pseudoarticulated |
0 |
1 (1.1) |
2 (5) |
| Segmented |
3 (6.4) |
9 (9.9) |
3 (5.7) |
| Pattern of elongation |
Marginal |
6 (2.9) |
16 (6.17) |
9 (5.22) |
088.0 |
| Partial |
2 (1.3) |
9 (9.9) |
2 (5) |
| Nodular |
4 (2.6) |
2 (2.2) |
2 (5) |
| Complete |
0 |
4 (4.4) |
3 (5.7) |
Discussion
Genetic and epigenetic variation is a fundamental contributing element in human diversity. From demographic and clinical perspectives, anatomical variation in the length of the styloid process and its stylohyoid chain poses significant diagnostic challenges. There are various elongated styloid processes, comprising the length of the process and the degree of calcification, as well as, the thickness of segments and direction and angle of deviation. These factors are used to determine the elongation and calcification type in each styloid and would be required to report the radiographic appearance accordingly (12,13).
In the current study, the panoramic radiographs of the patients were used to detect the elongated styloid process, which is similar to the process followed in other studies by Sudhakara Reddy et al (12), Imanimoghaddam et al (13), and Erol (14). The results of the current study revealed an overall average of around 27 mm for ligament length with the significant effect of age and the non-significant effect of gender. The association of the styloid process and age was consistent with that of Ezoddini Ardakani (5), representing the similar influence of age progression. The results of our study showed an extremely higher number of patients with the elongated styloid process when compared with those of Sudhakara Reddy et al (12). Various reasons may be put forward for explaining this discrepancy. Among these, it can be argued that there are differences between these two studies in the measuring tools, the type of software, software accuracy, and personal experience with the assessment procedure. Although the underlying mechanism of this ossification has not been fully elucidated, the stylohyoid ligament holds some parts of cartilage within ossification leading to various grades of elongation, and the ossification of the stylohyoid chain is suggested as the possible cause. The elongated styloid process normally follows an asymptomatic elongation of the styloid process (15). Likewise, only a portion of patients had a slight symptomatic elongation of the styloid process in our study, even though either bilateral or unilateral elongated styloid process was found among the patients.
The results of the current study revealed the influence of age on the calcification and elongation patterns of the styloid process while no significant association was found between gender and elongation and calcification patterns. Our results are consistent, in one aspect, with the findings of Balcioglu et al (16) and Sudhakara Reddy et al (12), demonstrating that these demographic factors (age and gender) significantly affect these patterns.
Conclusions
Based on the data of the current study and that in the literature, there is a potential association between the styloid elongation process and age progression. To the best of our knowledge, this is the first study to assess styloid process calcification and elongation patterns in the Ilam region. Further studies are still needed to assess different types of the styloid process and the relation between them in patients.
Conflict of Interest Disclosures
The authors declare no conflict of interests.
Acknowledgements
The authors are grateful to anonymous patients who participated in this study. We would also like to thank the anonymous referees who provided us with many insightful comments and suggestions on the previous version of this paper.
Ethical Statement
The necessary ethical approval for this study was obtained from the Ethical Committee of the Ilam University of Medical Sciences. Procedures on human subjects were conducted in accordance with the ethical standards of the Institutional and National Research Committee and the Helsinki Declaration of 1964 and its later amendments. Informed consent was signed by all the individuals who participated in the study.
Authors’ Contribution
VA conceived and designed the study. PA collected and analyzed the data. VA wrote the manuscript.
References
- Saccomanno S, Greco F, E DEC, Lucidi D, Deli R, D’Addona A. Eagle’s syndrome, from clinical presentation to diagnosis and surgical treatment: a case report. Acta Otorhinolaryngol Ital 2018; 38(2):166-9. doi: 10.14639/0392-100x-1479 [Crossref] [ Google Scholar]
- Bokhari MR, Graham C, Mohseni M. Eagle syndrome. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2020.
- Elimairi I, Baur DA, Altay MA, Quereshy FA, Minisandram A. Eagle’s syndrome. Head Neck Pathol 2015; 9(4):492-5. doi: 10.1007/s12105-014-0599-4 [Crossref] [ Google Scholar]
- Vadgaonkar R, Murlimanju BV, Prabhu LV, Rai R, Pai MM, Tonse M. Morphological study of styloid process of the temporal bone and its clinical implications. Anat Cell Biol 2015; 48(3):195-200. doi: 10.5115/acb.2015.48.3.195 [Crossref] [ Google Scholar]
- Ezoddini Ardakani F, Khayam E, Zangouei Booshehri M, Reihani Mohammadi A. The evaluation of the relationship between serum calcium level and stylohyoid length in adults. Acta Med Iran 2011; 49(11):742-7. [ Google Scholar]
- Sridevi K, Mahesh N, Krishnaveni B, Deepika ADN, Thejasri V, Leninson BHD. Evaluation of styloid process and its anatomical variations: a digital panoramic study with systematic review. J Int Soc Prev Community Dent 2019; 9(3):256-62. doi: 10.4103/jispcd.JISPCD_8_19 [Crossref] [ Google Scholar]
- Shayganfar A, Golbidi D, Yahay M, Nouri S, Sirus S. Radiological evaluation of the styloid process length using 64-row multidetector computed tomography scan. Adv Biomed Res 2018; 7:85. doi: 10.4103/2277-9175.233479 [Crossref] [ Google Scholar]
- Bruno G, De Stefani A, Balasso P, Mazzoleni S, Gracco A. Elongated styloid process: an epidemiological study on digital panoramic radiographs. J Clin Exp Dent 2017; 9(12):e1446-e52. doi: 10.4317/jced.54370 [Crossref] [ Google Scholar]
- Shaik MA, Kaleem SM, Wahab A, Hameed S. Prevalence of elongated styloid process in Saudi population of Aseer region. Eur J Dent 2013; 7(4):449-54. doi: 10.4103/1305-7456.120687 [Crossref] [ Google Scholar]
- Scavone G, Caltabiano DC, Raciti MV, Calcagno MC, Pennisi M, Musumeci AG. Eagle’s syndrome: a case report and CT pictorial review. Radiol Case Rep 2019; 14(2):141-5. doi: 10.1016/j.radcr.2018.10.008 [Crossref] [ Google Scholar]
- Langlais RP, Miles DA, Van Dis ML. Elongated and mineralized stylohyoid ligament complex: a proposed classification and report of a case of Eagle’s syndrome. Oral Surg Oral Med Oral Pathol 1986; 61(5):527-32. doi: 10.1016/0030-4220(86)90400-7 [Crossref] [ Google Scholar]
- Sudhakara Reddy R, Sai Kiran C, Sai Madhavi N, Raghavendra MN, Satish A. Prevalence of elongation and calcification patterns of elongated styloid process in south India. J Clin Exp Dent 2013; 5(1):e30-5. doi: 10.4317/jced.50981 [Crossref] [ Google Scholar]
- Imanimoghaddam M, Javadzadeh Bluori A, Ahmadian Yazdi A, Daneshvar F. A one year prevalence study on soft tissue opacities in panorarnic radiography in patients referred to radiology department of Mashhad dental school. J Mashhad Dent Sch 2010; 34(4):271-80. doi: 10.22038/jmds.2010.1177 [Crossref] [ Google Scholar]
- Erol B. Radiological assessment of elongated styloid process and ossified stylohyoid ligament. J Marmara Univ Dent Fac 1996; 2(2-3):554-6. [ Google Scholar]
- Politi M, Toro C, Tenani G. A rare cause for cervical pain: Eagle’s syndrome. Int J Dent 2009; 2009:781297. doi: 10.1155/2009/781297 [Crossref] [ Google Scholar]
- Balcioglu HA, Kilic C, Akyol M, Ozan H, Kokten G. Length of the styloid process and anatomical implications for Eagle’s syndrome. Folia Morphol (Warsz) 2009; 68(4):265-70. [ Google Scholar]