Avicenna J Dent Res. 13(1):6-12.
doi: 10.34172/ajdr.2021.02
Original Article
Comparative Evaluation of Microleakage in Class II Cavity in Primary Molars Restored With Glass Ionomer Cement, Zirconomer, and Cention N Using Stereomicroscope: An In Vitro Study
Harshali P Patil 1, Jasmin J Winnier 2, *
Author information:
1Postgraduate Student, Department of Pedodontics and Preventive Dentistry, D.Y Patil University, School of Dentistry, Nerul, Navi Mumbai, India.
2MDS, Associate Professor, Department of Pedodontics and Preventive Dentistry, D.Y Patil University, School of Dentistry, Nerul, Navi Mumbai, India.
Abstract
Background: Microleakage is defined as the passage of bacteria, fluid, molecules or ions between the cavity walls and restorative material. There are limited studies in the literature that have compared the microleakage of the newer restorative materials. Therefore, the aim of this study is to compare and evaluate microleakage in Class II cavity in primary molars restored with glass ionomer cement, zirconomer and cention N using stereomicroscope.
Method: Standardized Class II cavities were prepared on the extracted primary molars All the prepared samples were divided into 3 experimental groups and were restored as follows: Group I- GIC (GC Universal Restorative); Group II- Zirconomer (SHOFU Inc., Kyoto, Japan) and Group III- Cention-N (Ivoclar Vivadent). The restored teeth were thermocycled, immersed in methylene blue dye and sectioned along the mesiodistal direction. The dye penetration at the occlusal surface and cervical surface was evaluated and compared using a stereo-microscope. Data was analysed using Krushal-Wallis test (Non-parametric ANOVA).
Results: Among the three restorative materials, Cention N as compared to GIC and Zirconomer showed least microleakage at both the occlusal surface and cervical surface.
Conclusion: Cention N a newer restorative material displayed lesser microleakage as compared to GIC and Zirconomer.
Keywords: Class II restorations, primary molars, Cention N, Zirconomer, GIC, Microleakage
Copyright and License Information
© 2021 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Citation: Patil H, Winnier J. Comparative evaluation of microleakage in class II cavity in primary molars restored with glass ionomer cement, zirconomer, and cention n using stereomicroscope: an in vitro study. Avicenna J Dent Res. 2021;13(1):6- 12. doi: 10.34172/ajdr.2021.02.
Background
Highlights
-
None of the restorative materials used in the study were able to completely prevent microleakage at both the cervical and the occlusal surface.
-
Among the three restorative materials, Cention N significantly showed less microleakage as compared to GIC and Zirconomer at the occlusal and cervical surface.
Dental restorations or their replacement are the most common procedures performed by the dentists (1). Due to the differences in tooth morphology, restoration of primary teeth differs from the permanent teeth. The enamel and dentin in the primary teeth are thinner. They also have shorter crown height, which makes it very challenging to prepare a cavity on the proximal surface, and this affects the ability of primary teeth to adequately support and retain restorations (2).
Microleakage is defined as the passage of bacteria, fluid, molecules or ions between the cavity walls and restorative material. The main cause of microleakage is poor adaptation between the restorative material and the tooth structure. Volume change in the restorative material due to oral thermal changes is another secondary cause that forms a gap between the restorative material and tooth leading to microleakage and secondary caries (3). The advent of newer restorative materials like Cention N and Zirconomer with modified properties can help overcome this drawback and give a better result.
Cention N (Ivoclar Vivadent; Schaan, Liechtenstein) is a tooth-coloured, metal-free “alkasite” restorative basic filling material introduced in 2016. It was developed in response to the global initiative established by the United Nations Environment Programme (UNEP) to reduce the use of mercury. It includes special patented filler (Isofiller) acting as a shrinkage stress reliever, which reduces polymerization shrinkage and microleakage (4). Another new generation of GIC - Zirconomer (Shofu Inc., Japan) was introduced by incorporating particles of zirconia in order to achieve greater compressive and flexure strengths, as well as to attain less occlusal wear and fast setting reaction. GIC Fuji IX was used as reference material in the present study, because it is the most frequently used material in both the in vivo and in vitro studies, as well as its ability to release fluoride and to chemically bond to tooth structures with additional benefits of biocompatibility and antibacterial effects (5).
The aim of this study was to evaluate microleakage of GIC Type IX with two recently launched restorative materials (Zirconomer and Cention N) using stereomicroscope for class II restoration in extracted primary molars.
Materials and Methods
An in vitro study was conducted to evaluate and compare cervical and occlusal microleakage in class II cavity restored with Glass Ionomer Cement, Zirconomer, and Cention N using stereomicroscope. In the present study, 45 non-carious maxillary and mandibular first and second deciduous molars were included, which were part of serial extraction procedure or retained primary teeth extracted at the time of eruption of permanent teeth. Grossly carious teeth or teeth with hypoplastic defects were excluded. The sample size calculation was done using one-way ANOVA with Alpha error = 5%, power= 90%, and beta error = 66%. In addition, the minimum required sample size was calculated as 13.
Procedure
Each tooth underwent scaling and root planning with an ultrasonic device (6) to remove residual organic tissue. Then, the teeth were cleaned with pumice and stored in 0.1% thymol solution (7).
The teeth were randomly divided into one of the three groups:
-
Group 1 (15) Teeth restored with GIC (GC Universal Restorative)
-
Group 2 (15) Teeth restored with Zirconomer (SHOFU Inc., Kyoto, Japan)
-
Group 3 (15) Teeth restored with Cention-N (Ivoclar Vivadent)
Five teeth in each group were mounted on a single wax sheet for placement of Tofflemire matrix, which allowed building up of the proximal wall. A standardized class II cavity preparation was made involving the proximal and occlusal surfaces using number 245 tungsten carbide bur (8,9) in a highspeed air motor handpiece with water spray.On the occlusal surface, the width of the isthmus was kept to approximately one-third of the buccal and the lingual cusp and the pulpal floor was flat and placed 0.5 mm into the dentin (10). After the cavity was cleaned and dried by compressed air, a matrix band and retainer was placed on the tooth (3).
Group I: GIC was dispensed as powder and liquid onto the mixing pad with the standard powder to liquid ratio of 1 level scoop of powder to 1 drop of liquid. Using a plastic spatula, the powder was divided into 2 equal parts (11). The first portion was mixed with all the liquid for 10 seconds. The remaining portion was incorporated and mixed for 15-20 seconds, and GIC was mixed and introduced using the plastic filling instrument (11). After losing the glossy appearance of the material, moisture protection was done using cocoa butter.
Group II: One scoop of dispensed Zirconomer powder was divided into 2 equal portions; the first half was mixed in liquid for 5-10 seconds with the plastic spatula provided (12). Then, the remaining half was mixed until it reached a thick putty-like consistency. Mixing was completed within a total of 30 seconds. Zirconomer was then filled, condensed into the cavity, and polished with abrasive discs and stones after 7 minutes (12).
Group III: Cention N was mixed with 1 measuring scoop of powder and 1 drop of liquid on a mixing pad until a homogeneous consistency was achieved. It was then restored and condensed into cavity.
The restored teeth were stored for 1 week in distilled water at 37°C, and then subjected to 500 cycles of thermocycling between 5°C and 55°C with a dwell time of 30 seconds in each bath (Figure 1) (13). After thermocycling, all the tooth surfaces, except the restoration and 1 mm zone adjacent to the restoration’s margins, were covered with two coats of nail varnish and allowed to air dry (Figure 2). The coated teeth were then immersed in 2% methylene blue dye solution for 24 hours at 37°C (7). The teeth were sectioned mesiodistally through the center of each restoration using diamond disc. The dye penetration at the occlusal and gingival margins of each section were evaluated using a stereo-microscope at a magnification of ×22.5 (Figures 3, 4, and 5) based on the following criteria (6):
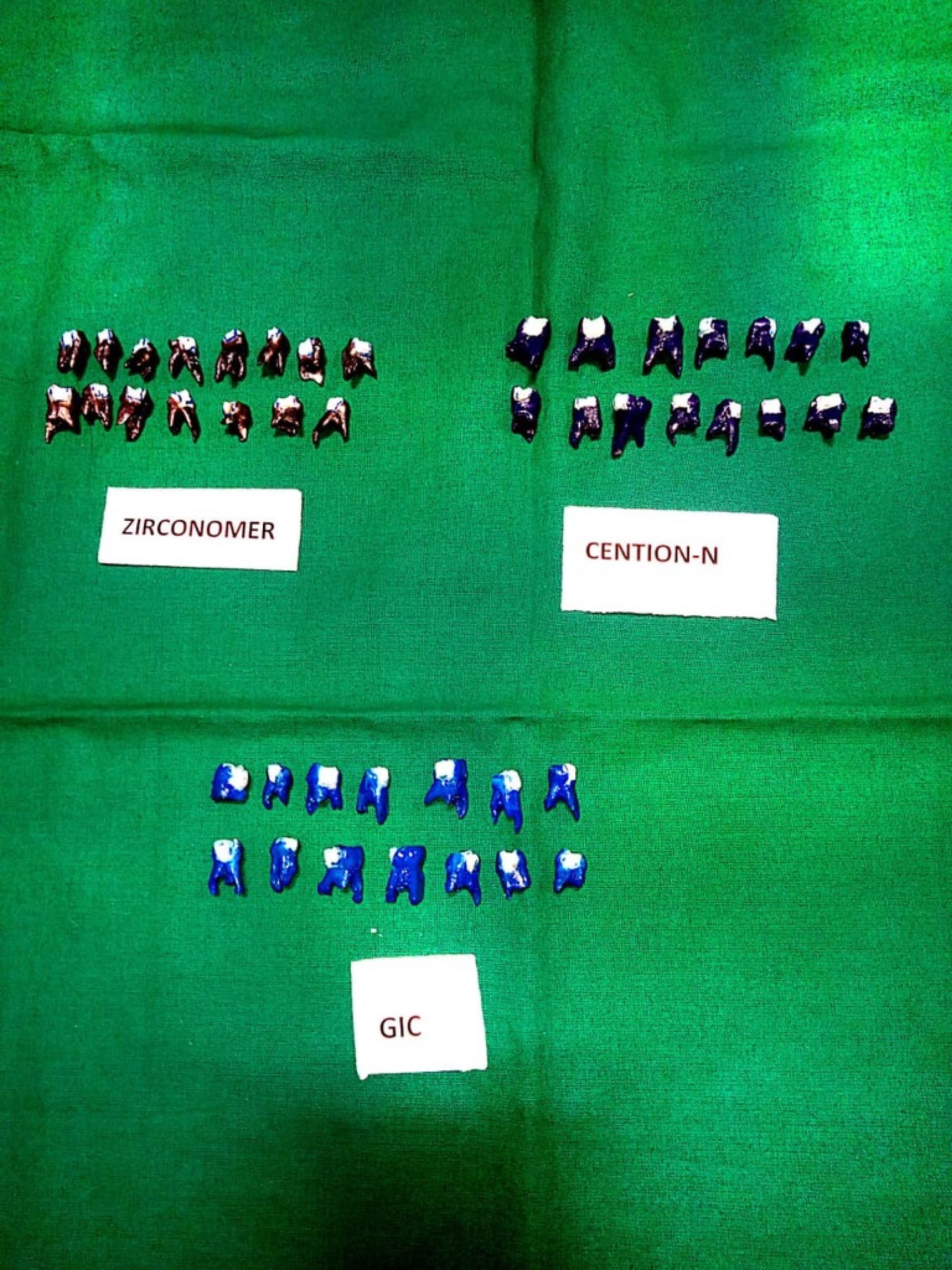
Figure 2.
Tooth Coated With Nail Varnish.
.
Tooth Coated With Nail Varnish.
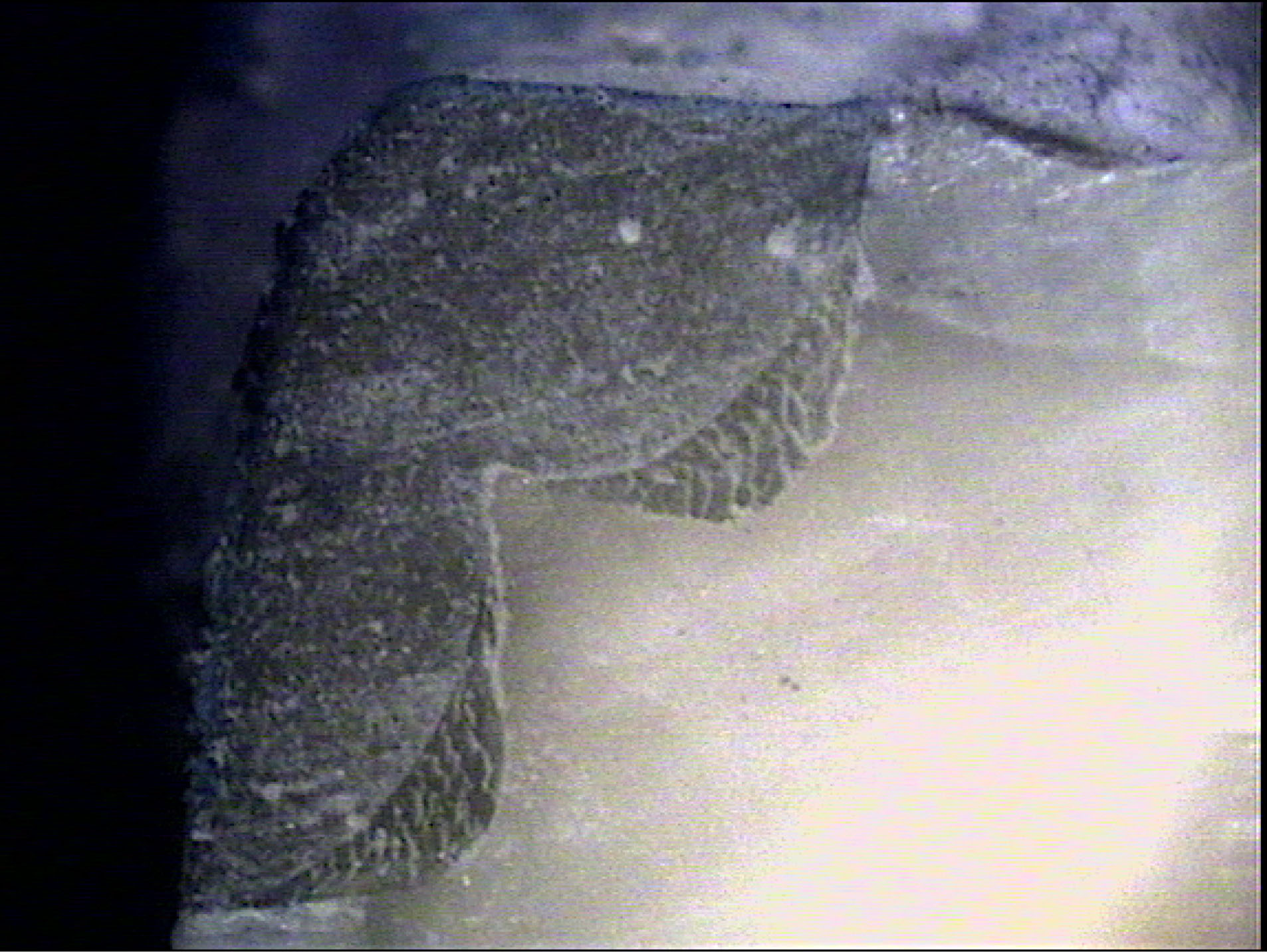
Figure 3.
No Dye Penetration (Magnification ×22.5).
.
No Dye Penetration (Magnification ×22.5).
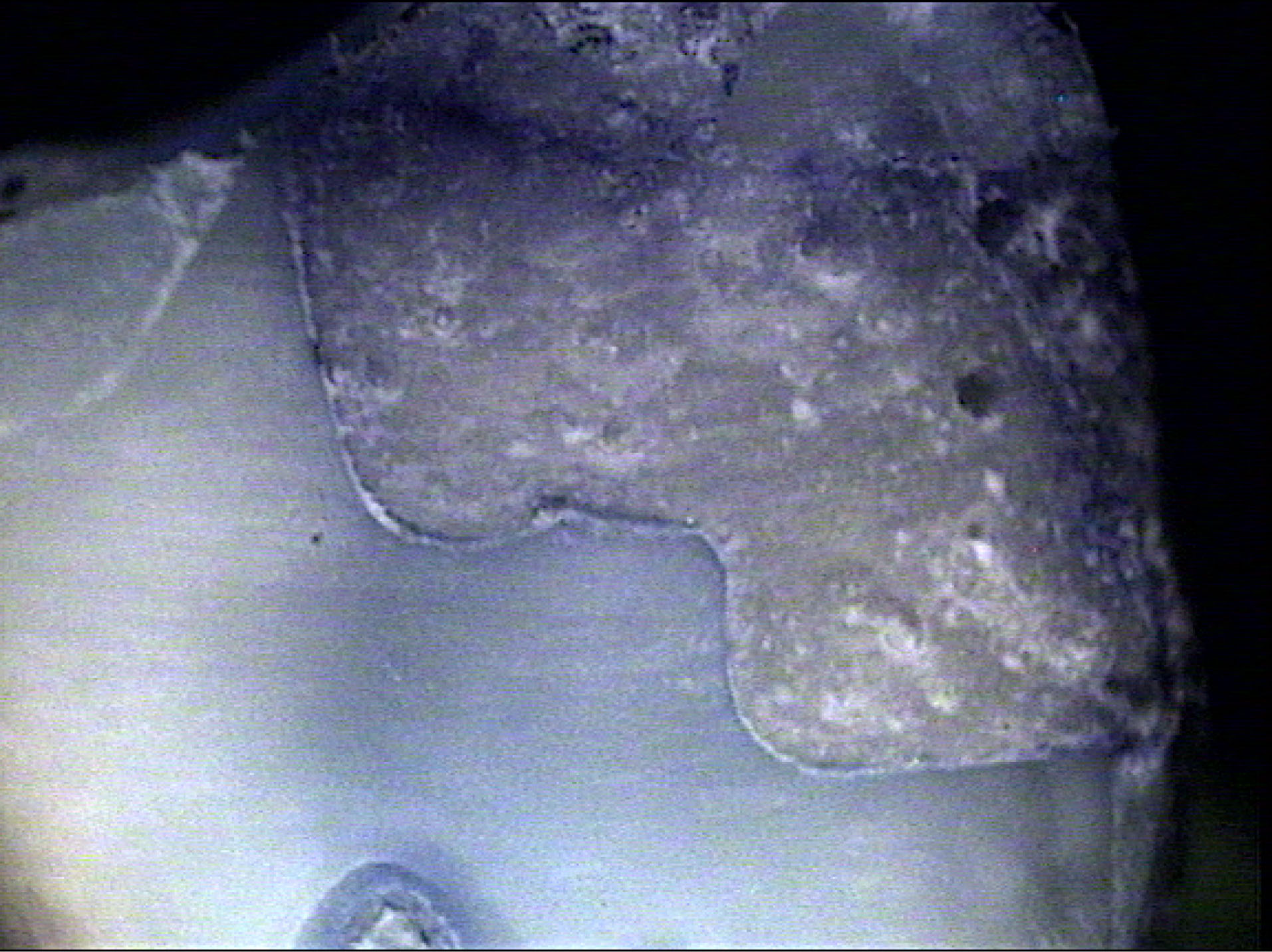
Figure 4.
Dye Penetration into the Dentine Including the Pulpal Wall (Magnification ×22.5).
.
Dye Penetration into the Dentine Including the Pulpal Wall (Magnification ×22.5).
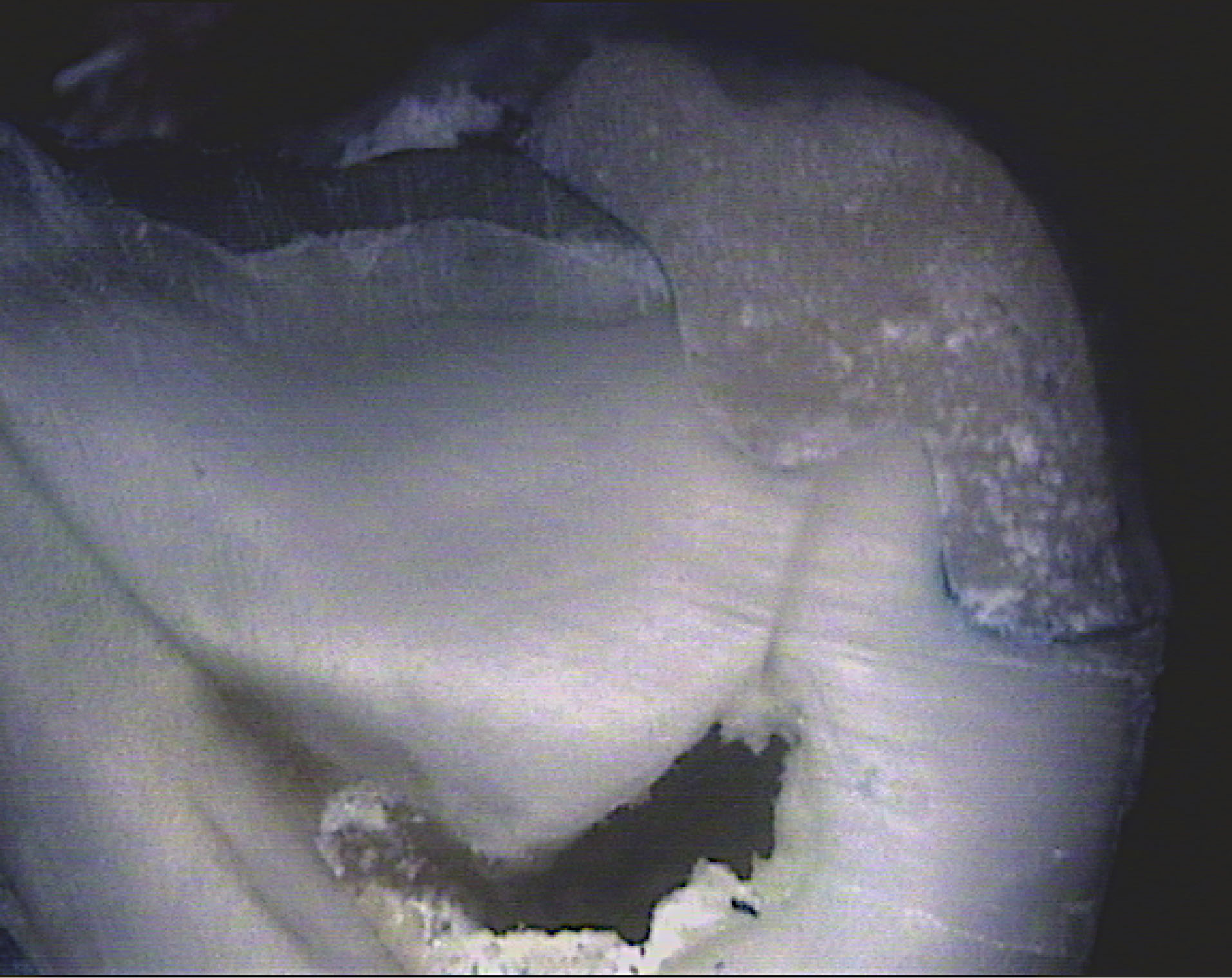
Figure 5.
Dye Penetration into the Cervical and Axial Wall (Magnification ×22.5).
.
Dye Penetration into the Cervical and Axial Wall (Magnification ×22.5).
Occlusal Margin
Score 0 = No dye penetration
Score 1 = Dye penetration into the enamel
Score 2 = Dye penetration into the dentin, not including the pulpal wall
Score 3 = Dye penetration into the dentin including the pulpal wall
Cervical Margin
Score 0 = No dye penetration
Score 1 = Dye penetration into 1⁄2 of the cervical wall
Score 2 = Dye penetration into the entire length of cervical wall
Score 3 = Dye penetration into the cervical and axial wall
All the data was subjected to statistical analysis to compare the microleakage between three groups.
Results
Microleakage at the Occlusal Surface in the Three Groups
The mean microleakage scores at the occlusal surface comparing three groups using Kruskal-Wallis test (non-parametric ANOVA) are presented in Table 1 and Figure 6. The results revealed that the mean microleakage score of Zirconomer was the highest score (2.43) followed by GIC (2.20) and Cention N (1.43)
Table 1.
The Mean Microleakage Scores at the Occlusal Level Comparing the Three Groups (Zirconomer, GIC, and Cention N) Using Kruskal-Wallis Test (Non-parametric ANOVA)
|
Group
|
N
|
Mean
|
SD
|
Median
|
Rank
|
P
Value
|
| Zirconomer |
14 |
2.43 |
1.09 |
3 |
29.29 |
0.0010 |
| GIC |
15 |
2.20 |
0.86 |
2 |
25.47 |
|
| Cention N |
15 |
1.13 |
0.83 |
1 |
13.20 |
|
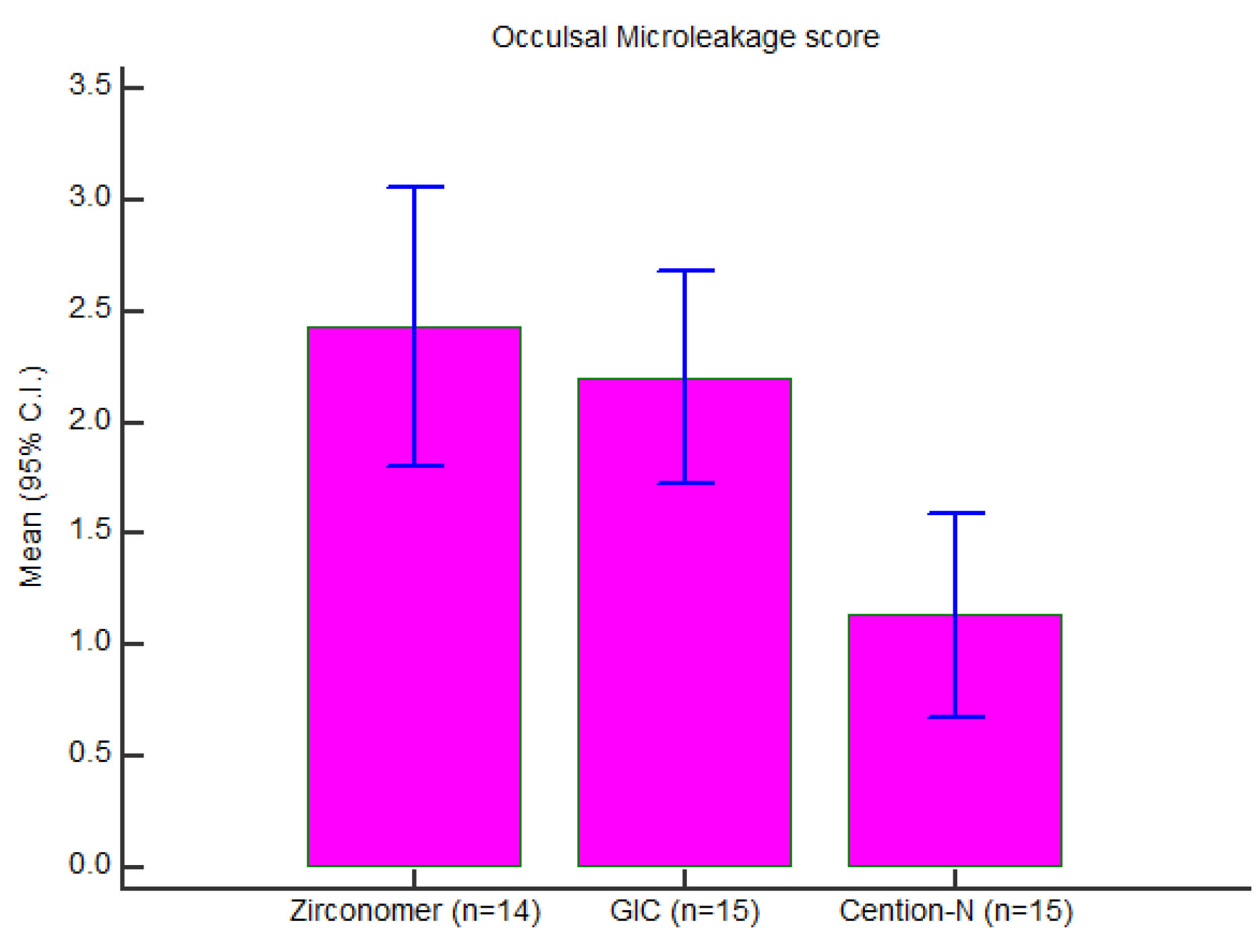
Figure 6.
Graphical Presentation of Occlusal Microleakage Scores (Mean) in Three Groups.
.
Graphical Presentation of Occlusal Microleakage Scores (Mean) in Three Groups.
Post-hoc individual pairwise comparisons were done between the three groups using Mann-Whitney ‘U’ test (Table 2), which showed statistically significant difference in the mean microleakage scores between group 1 and group 3, as well as group 2 and group 3. However, there was no significant difference between group 1 and group 2.
Table 2.
Post Hoc Individual Pairwise Comparisons Between the Three Groups Using Mann-Whitney U Test
|
Pairwise Comparisons
|
Z
|
P
Value
|
| Zirconomer Vs GIC |
1.056 |
0.2909 |
| Zirconomer Vs Cention N |
3.270 |
0.0011 |
| GIC Vs Cention N |
2.836 |
0.0046 |
The mean difference is significant at the P < 0.05 level.
Microleakage at the Cervical Surface in the Three Groups
The mean microleakage scores at the cervical region were compared between the three groups using Kruskal-Wallis test (non-parametric ANOVA) (Table 3 and Figure 7). According to the results, Zirconomer had the highest mean score (2.14) followed by GIC (1.93) and Cention N (0.40)
Table 3.
The Mean Microleakage Scores at the Cervical Level in the Three Groups (Zirconomer, GIC, and Cention N) Using Kruskal-Wallis Test (Non-parametric ANOVA)
|
Group
|
N
|
Mean
|
SD
|
Median
|
Rank
|
P
Value
|
| Cervical |
|
|
|
|
|
|
| Zirconomer |
14 |
2.14 |
1.23 |
3 |
29.11 |
0.0001 |
| GIC |
15 |
1.93 |
0.96 |
2 |
27.23 |
|
| Cention N |
15 |
0.40 |
0.51 |
0 |
11.60 |
|
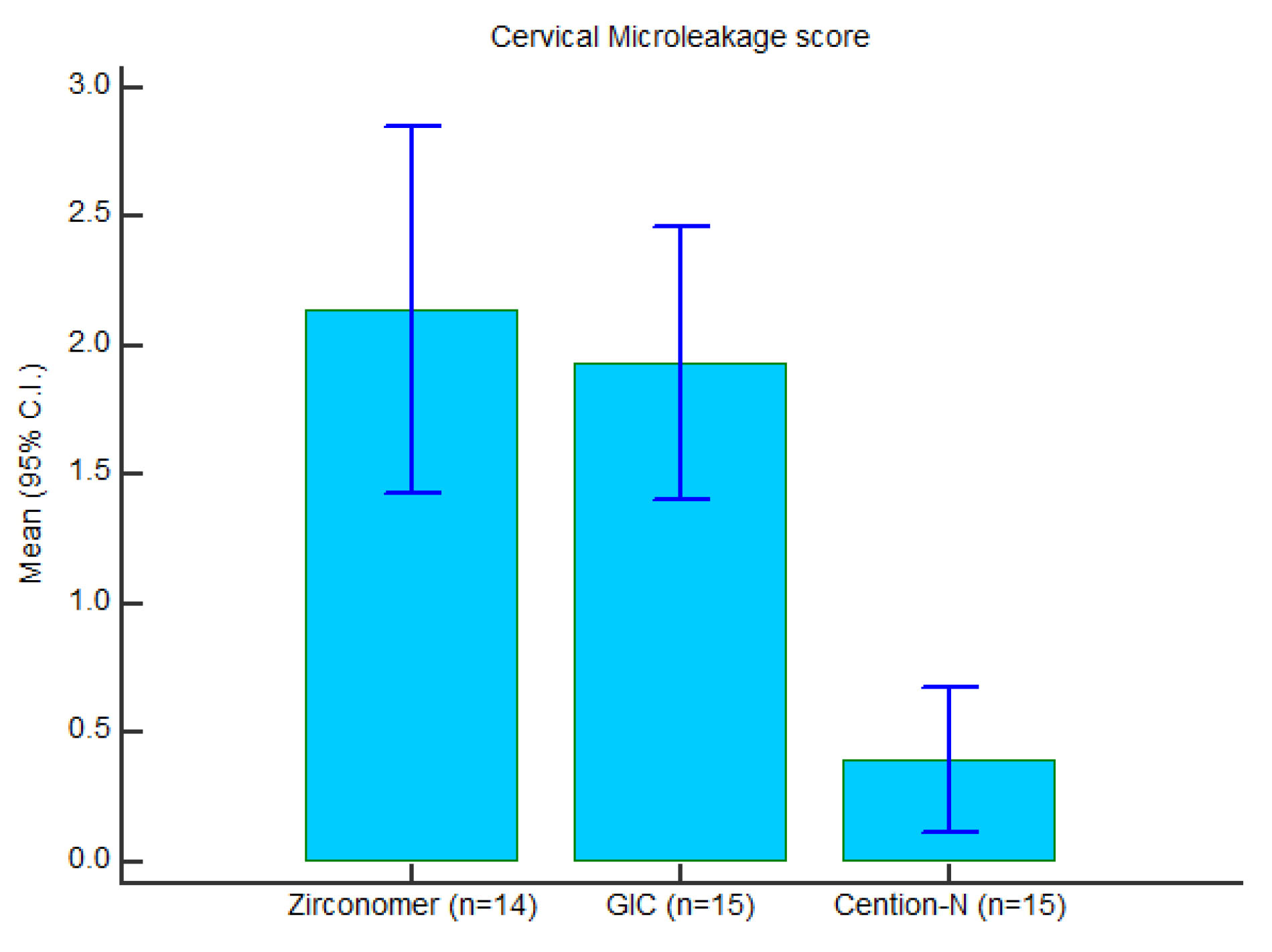
Figure 7.
Graphical Presentation of Cervical (Gingival) Microleakage Scores (Mean) in Three Groups.
.
Graphical Presentation of Cervical (Gingival) Microleakage Scores (Mean) in Three Groups.
Post-hoc individual pairwise comparisons were done between the three groups using Mann-Whitney ‘U’ test (Table 4), which showed statistically significant difference in the mean microleakage scores between group 1 and group 3, as well as group 2 and group 3. However, there was no significant difference between group 1 and group 2.
Table 4.
Post Hoc Individual Pairwise Comparisons Between the Three Groups Using Mann-Whitney U Test
|
Pairwise Comparisons
|
Z
|
P
Value
|
| Zirconomer Vs GIC |
0.867 |
0.3857 |
| Zirconomer Vs Cention N |
3.332 |
0.0009 |
| GIC Vs Cention N |
3.846 |
0.0001 |
The mean difference is significant at the P < 0.05 level.
Discussion
The reported global failure rate of restoration is 12.5% with more failures associated with class II (14.7%) as compared with class I (7%) (14). The predominating factors for failure in class II cavities are fracture and loss of retention of restorative material (15). Evaluation of clinical performance of restorative material revealed secondary caries to be the major factor for failure of class II restoration (16) and microleakage is considered as one of the primary reasons for development of secondary caries (8). Thus, the present study evaluated microleakage in class II cavity restored with GIC, Zirconomer, and Cention N.
Glass-ionomers were introduced by Wilson and Kent in 1972 (17). It has a coefficient of thermal expansion very similar to that of the tooth structure with low setting shrinkage, providing good marginal seal, having the capacity of fluoride release and storage, good adhesion to tooth structure, and is biocompatible (18). Not only the biocompatibility of GIC is useful for pulp tissues, but also it is useful for periodontal tissues, because it has the potential to reduce subgingival biofilm, causing no irritation to the tissues (19). Zirconomer, a new generation GIC, has superior mechanical properties with remarkable edge strength, excellent marginal adaptation, and excellent resistance to abrasion and erosion; in addition, it has tooth-like coefficient of thermal expansion, sustained fluoride protection, higher translucency to match natural tooth, and is considered to be an ideal restorative material for class I and II cavities in deciduous teeth (20). Cention N is a tooth-coloured material which is stronger than glass ionomer cement, has better esthetics than amalgam, and is indicated in the restoration of deciduous teeth.
Various authors have conducted in vitro studies on class V cavities in permanent teeth. Walia et al stated that that the microleakage score was maximum in Giomer followed by Zirconomer and Ceram-x, and the least was in Ketac Molar (21). Similar results were reported by Asafarlal, in which Ketac molar was compared with Zirconomer and Fuji IX Extra GC (22). Salman et al reported maximum microleakage in Giomer followed by Zirconomer, resin-modified glass ionomer, and the least was seen in nano-ionomer (23). Naz et al concluded that Cention N had the least microleakage followed by Zirconomer improved and GIC type IX (24). Similarly, Sujith et al reported that the mean microleakage score for Cention N was the lowest score as compared to GIC and composite restorative materials (25).
Punathil et al concluded that nano-filled resin-modified glass-ionomer had the least microleakage followed by Ceniton N and nano-composites in primary molars with class II cavities (26). In contrast, Mazumdar et al reported that Cention N displayed minimum microleakage as compared to amalgam and GIC for class II cavities; however, the authors did not mention whether they evaluated primary or permanent teeth (8).
Kini et al reported that teeth restored with Cention N after application of adhesive presented the least microleakage, followed by teeth restored with Cention N without adhesive followed by type IX glass ionomer cement (Fuji) and posterior composite in premolars with class I cavities (27). There is limited literature on microleakage in class II cavities in primary teeth using these materials.
In the present study, 45 non-carious primary molars were collected based on the inclusion and exclusion criteria and stored in 0.1% thymol. It was reported that microleakage scores of teeth stored in 0.1% thymol were not different from the microleakage scores of freshly extracted teeth, thus making it an appropriate medium for storage (13). After preparation and restoration of the class II cavity with the respective material, the restored teeth were subjected to thermocycling. Thermocycling was done at 5°C for 30 seconds and 55°C for 30 seconds with the dwell time of 3-4 seconds for 500 cycles. This was considered as the ideal temperature, which is extremely close to the oral conditions and the increase in the numbers of cycles had no correlation with increase in microleakage (28).
Dyes, radioactive isotopes, air pressure, bacteria, neutron activation analysis, and artificial caries techniques are used to study microleakage at the interface between tooth and restorations. Dye leakage methodology remains the most popular tool till date. Although dyes like basic fuchsin, methylene blue, and silver nitrate (29) can be used, the particle size of the methylene blue is less than the internal diameter of the dentinal tubule, and therefore, it shows a better dentin permeability. Thus, in this study, 2% methylene blue was used. It is simple, cheap, and does not require any complex lab procedures; in addition, it provides easy visualization and easy reference point for scoring.
This is the first study that evaluated and compared the microleakage in class II cavity in primary molars using Zirconomer, GIC, and Cention N. Cention N exhibited significantly less microleakage at both the occlusal and gingival surface compared to GIC and Zirconomer. This is similar to some previous studies, in which Cention N showed less microleakage compared to amalgam and GIC in class II cavity (6), and compared to composite and GIC in class V cavity in permanent molars (4).The possible reason for this could be because Cention N includes a special Isofiller, which acts as a shrinkage stress reliver that prevents shrinkage of the material and helps to reduce Microleakage (4).
It was noted that Zirconomer had the highest mean microleakage followed by GIC and Cention N in both regions. This is comparable to previous studies that reported Zirconomer showing higher microleakage scores as compared to composite and amalgam in class I cavities of non-carious permanent molars (30). Another study reported that Zirconomer had a higher microleakage as compared to nano-ionomer in class V cavities of non-carious premolars (22).
GIC exhibited less microleakage as compared to Zirconomer in this study. This could be due to its high dimensional stability, lower thermal conductibility, and chemical adhesion to dentin.
Conclusions
Within the limitations of the present study, the following conclusions may be made:
-
None of the restorative materials used in the study were able to completely prevent microleakage.
-
Among the three restorative materials, Cention N exhibited the least microleakage followed by GIC and Zirconomer.
Conflict of Interest Disclosures
The authors declare that they have no conflict of interests.
Ethical Statement
The present study was approved by Institutional research and ethical board of D Y Patil University- School of Dentistry. (IREB Reference Number: IREB/ 2020/ PEDO / 02)
Authors’ Contribution
HP: Concepts, design, definition of intellectual content, Literature search, clinical studies, experimental studies, data acquisition, data analysis, statistical analysis, and manuscript preparation, manuscript editing, manuscript review; JW: Concepts, design, clinical studies, experimental studies, manuscript editing, manuscript review; and a guarantor. All authors read and approved the manuscript.
Funding
None.
References
- Blum IR, Özcan M. Reparative dentistry: possibilities and limitations. Curr Oral Health Rep 2018; 5(4):264-9. doi: 10.1007/s40496-018-0191-1 [Crossref] [ Google Scholar]
- Council on Clinical Affairs. Guideline on Pediatric Restorative Dentistry. American Academy of Pediatric Dentistry (AAPD); 1991.
- Shih WY. Microleakage in different primary tooth restorations. J Chin Med Assoc 2016; 79(4):228-34. doi: 10.1016/j.jcma.2015.10.007 [Crossref] [ Google Scholar]
- Samanta S, Das UK, Mitra A. Comparison of microleakage in class V cavity restored with flowable composite resin, glass ionomer cement and cention N. Imp J Interdiscip Res 2017; 3(8):180-3. [ Google Scholar]
- Salas CF, Guglielmi CA, Raggio DP, Mendes FM. Mineral loss on adjacent enamel glass ionomer cements restorations after cariogenic and erosive challenges. Arch Oral Biol 2011; 56(10):1014-9. doi: 10.1016/j.archoralbio.2011.03.005 [Crossref] [ Google Scholar]
- Radhika M, Sajjan GS, Kumaraswamy BN, Mittal N. Effect of different placement techniques on marginal microleakage of deep class-II cavities restored with two composite resin formulations. J Conserv Dent 2010; 13(1):9-15. doi: 10.4103/0972-0707.62633 [Crossref] [ Google Scholar]
- Ziskind D, Adell I, Teperovich E, Peretz B. The effect of an intermediate layer of flowable composite resin on microleakage in packable composite restorations. Int J Paediatr Dent 2005; 15(5):349-54. doi: 10.1111/j.1365-263X.2005.00663.x [Crossref] [ Google Scholar]
- Mazumdar P, Das A, Das UK. Comparative evaluation of microleakage of three different direct restorative materials (silver amalgam, glass ionomer cement, cention N), in Class II restorations using stereomicroscope: an in vitro study. Indian J Dent Res 2019; 30(2):277-81. doi: 10.4103/ijdr.IJDR_481_17 [Crossref] [ Google Scholar]
- McDonald RD, Avery DR, Dean JA. Dentistry for the Child and Adolescent. 8th ed. Missouri: Mosby; 2004.
- Finn SB. Clinical Paedodontics. 4th ed. WB Saunders Company; 1973.
- Instructions for use- GC Amrica. Available from: https://www.gcamerica.com/products/operatory/GC_Fuji_IX_GP/GC_Fuji_IX_GP-PL_10IFU_2014.pdf.
- Zirconomer Improved- Shofu. Instructions for use. Available form: https://www.shofu.com.sg/wp-content/uploads/2020/02/Zirconomer-Improved-IFU.pdf.
- Amaireh AI, Al-Jundi SH, Alshraideh HA. In vitro evaluation of microleakage in primary teeth restored with three adhesive materials: ACTIVATM, composite resin, and resin-modified glass ionomer. Eur Arch Paediatr Dent 2019; 20(4):359-67. doi: 10.1007/s40368-019-00428-6 [Crossref] [ Google Scholar]
- Chisini LA, Collares K, Cademartori MG, de Oliveira LJC, Conde MCM, Demarco FF. Restorations in primary teeth: a systematic review on survival and reasons for failures. Int J Paediatr Dent 2018; 28(2):123-39. doi: 10.1111/ipd.12346 [Crossref] [ Google Scholar]
- Qvist V, Laurberg L, Poulsen A, Teglers PT. Class II restorations in primary teeth: 7-year study on three resin-modified glass ionomer cements and a compomer. Eur J Oral Sci 2004; 112(2):188-96. doi: 10.1111/j.1600-0722.2004.00117.x [Crossref] [ Google Scholar]
- Dias AGA, Magno MB, Delbem ACB, Cunha RF, Maia LC, Pessan JP. Clinical performance of glass ionomer cement and composite resin in Class II restorations in primary teeth: a systematic review and meta-analysis. J Dent 2018; 73:1-13. doi: 10.1016/j.jdent.2018.04.004 [Crossref] [ Google Scholar]
- Nicholson JW. Chemistry of glass-ionomer cements: a review. Biomaterials 1998; 19(6):485-94. doi: 10.1016/s0142-9612(97)00128-2 [Crossref] [ Google Scholar]
- Rizzante FAP, Cunali RS, Bombonatti JFS, Correr GM, Gonzaga CC, Furuse AY. Indications and restorative techniques for glass ionomer cement. RSBO Revista Sul-Brasileira de Odontologia 2015; 12(1):79-87. doi: 10.21726/rsbo.v12i1.183 [Crossref] [ Google Scholar]
- Modena KC, Casas-Apayco LC, Atta MT, Costa CA, Hebling J, Sipert CR. Cytotoxicity and biocompatibility of direct and indirect pulp capping materials. J Appl Oral Sci 2009; 17(6):544-54. doi: 10.1590/s1678-77572009000600002 [Crossref] [ Google Scholar]
- Abdulsamee M, Elkhadem AH. “Zirconomer and Zirconomer improved (white amalgams): restorative materials for the future” Review. EC Dent Sci 2017; 15(4):134-50. [ Google Scholar]
- Walia R, Jasuja P, Verma KG, Juneja S, Mathur A, Ahuja L. A comparative evaluation of microleakage and compressive strength of Ketac Molar, Giomer, Zirconomer, and Ceram-x: an in vitro study. J Indian Soc Pedod Prev Dent 2016; 34(3):280-4. doi: 10.4103/0970-4388.186746 [Crossref] [ Google Scholar]
- Asafarlal S. Comparative Evaluation of Microleakage, Surface Roughness and Hardness of Three Glass Ionomer Cements–Zirconomer, Fujii IX Extra GC and Ketac Molar: An In Vitro Study. Dentistry 2017; 7(5):427. doi: 10.4172/2161-1122.1000427 [Crossref] [ Google Scholar]
- Salman K, Naik S, Kumar N, Merwade S, Brigit B, Jalan R. Comparative evaluation of microleakage in Class V cavities restored with Giomer, resin-modified glass ionomer, Zirconomer and nano-ionomer: an in vitro study. J Int Clin Dent Res Organ 2019; 11(1):20-5. doi: 10.4103/jicdro.jicdro_2_19 [Crossref] [ Google Scholar]
- Naz T, Singh DJ, Somani R, Jaidka S. Comparative evaluation of microleakage and compressive strength of glass ionomer cement type IX, Zirconomer improved and cention N-an in vitro study. Int J Adv Res 2019; 7(9):921-31. doi: 10.21474/ijar01/9738 [Crossref] [ Google Scholar]
- Sujith R, Yadav TG, Pitalia D, Babaji P, Apoorva K, Sharma A. Comparative evaluation of mechanical and microleakage properties of Cention-N, composite, and glass ionomer cement restorative materials. J Contemp Dent Pract 2020; 21(6):691-5. [ Google Scholar]
- Punathil S, Almalki SA, AlJameel AH, Gowdar IM, Mc VA, Chinnari K. Assessment of microleakage using dye penetration method in primary teeth restored with tooth-colored materials: an in vitro study. J Contemp Dent Pract 2019; 20(7):778-82. [ Google Scholar]
- Kini A, Shetty S, Bhat R, Shetty P. Microleakage evaluation of an alkasite restorative material: an in vitro dye penetration study. J Contemp Dent Pract 2019; 20(11):1315-8. [ Google Scholar]
- Pazinatto FB, Campos BB, Costa LC, Atta MT. Effect of the number of thermocycles on microleakage of resin composite restorations. Pesqui Odontol Bras 2003; 17(4):337-41. doi: 10.1590/s1517-74912003000400008 [Crossref] [ Google Scholar]
- AlHabdan AA. Review of microleakage evaluation tools. J Int Oral Health 2017; 9(4):141-5. doi: 10.4103/jioh.jioh_160_17 [Crossref] [ Google Scholar]
- Patel MU, Punia SK, Bhat S, Singh G, Bhargava R, Goyal P. An in vitro evaluation of microleakage of posterior teeth restored with amalgam, composite and zirconomer-a stereomicroscopic study. J Clin Diagn Res 2015; 9(7):ZC65-7. doi: 10.7860/jcdr/2015/13024.6225 [Crossref] [ Google Scholar]