Avicenna J Dent Res. 13(1):1-5.
doi: 10.34172/ajdr.2021.01
Original Article
Accuracy of CBCT Linear Measurements to Determine the Height of Alveolar Crest to the Mental Foramen
Mahnaz Sheikhi 1, Seyed Ali Saleh Gholami 2, *  , Maryam Ghazizadeh 3
, Maryam Ghazizadeh 3
Author information:
1Torabinejad Dental Research Center, Department of Oral and Maxillofacial Radiology, School of Dentistry, Isfahan University of Medical Sciences, Isfahan, Iran.
2Department of Oral and Maxillofacial Radiology, School of Dentistry, Yasuj University of Medical Sciences, Yasuj, Iran.
3Department of Oral and Maxillofacial Radiology, School of Dentistry, Kermanshah University of Medical Sciences, Kermanshah, Iran.
Abstract
Background: Detailed knowledge of the three-dimensional (3D) anatomical structures in precise treatment planning prior to implant placement is necessary. The choice of imaging techniques plays an important role in achieving the required information to measure exact dimensions. Cone beam computed tomography (CBCT) has increasingly been used for diagnosis and treatment in the fields of periodontology, endodontic, and orthodontics. It is also used as the preoperative evaluation of patients who are candidates for dental implant treatment. Dental implant placement is an important application of CBCT in dentistry. One of the features of CBCT is the possibility of changing the slice thickness while reviewing images. In this study, we examined the linear measurement accuracy of CBCT for determining the height of alveolar crest to the mental foramen in cross-sectional view with different slice thicknesses and in tangential view.
Methods: We used five dry human mandibles in this study. Then the distance from the highest tip of alveolar crest to the upper border of mental foramen was measured by digital caliper (as gold standard) and on CBCT images in cross sectional view with 1, 3, 5, 7 and 9 mm slice thicknesses and in tangential view. Data were analyzed using IBM SPSS Statistics software version 22, paired t test, and inter class correlation.
Results: Data were collected by evaluation of 5 dry mandible and 240 measurements. There were significant differences only in tangential view and 1 mm slice thickness option in cross-sectional view with the gold standard (P=0.003 and P=0.018 respectively). The results did not show any differences between the observers (P<0.001).
Conclusions: Our results indicated that cross-sectional view is more accurate than tangential view, and 3 and 5 mm slice thicknesses are preferred for measurement.
Keywords: CBCT, Mental foramen, Slice thickness
Copyright and License Information
© 2021 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Citation: Sheikhi M, Saleh Gholami SA, Ghazizadeh M. Accuracy of cbct linear measurements to determine the height of alveolar crest to the mental foramen. Avicenna J Dent Res. 2021;13(1):1-5. doi: 10.34172/ajdr.2021.01.
Background
Highlights
-
Dental implant placement is an important application of CBCT in dentistry.
-
in this article, the linear measurement accuracy of CBCT for determining the height of alveolar crest to the mental foramen in cross-sectional view with different slice thickness and in tangential view is evaluated.
-
results showed that cross-sectional view is more accurate than tangential view, and 3 and 5 mm slice thickness are preferred for measurement.
The surgical procedures, such as implant placement, third molar surgery, and fractures repair of the mandible require exact knowledge of anatomical structures (1). Using dental implants in edentulous patients is rapidly increasing. Implant treatment requires different radiographic examination to assess height and buccolingual width of the implant placement site (2-4). Intraoral and panoramic images cannot provide three-dimensional (3D) information (5,6). Panoramic images have several limitations, such as non-uniform magnification, distortion, and the superimposition of anatomical structures (7-9). Therefore, selecting the type of imaging techniques plays an important role in achieving the necessary information and best measurement accuracy (10). Cone beam computed tomography (CBCT) is increasingly used for the diagnosis and treatment in the fields of periodontology, endodontic, orthodontics, and patients who are candidates for dental implant treatment (11,12). The advantages of this method include high resolution, lower radiation dose, and lower cost compared to CT (2).
Several studies examined the accuracy of CBCT measurement. In a study, Shokri et al measured the height and width of alveolar bone with CBCT machine in 0.5, 1, 2, 3, 5, and 10 mm slice thicknesses. It was shown that the highest measurement accuracy was observed at 4 mm slices for bone width and 5 mm slice thickness for bone height (2). Sheikhi et al reported that the accuracy of measurements in CBCT machine varies when the position of the skull deviates from ideal; however, the differences are not clinically significant (13). Stratemann et al compared accurate images from two New Tom (CBCT) and Hitachi Mercury machines, and showed that the errors of two machines were too small compared to the actual size. The errors were 0.07 ± 0.41 for New Tom and 0.00 ± 0.22 for Hitachi Mercury (14).
The software programs of CBCT make it possible to change the slice thickness. It happens many times that implantologists and surgeons demand CBCT or CT with different slice thicknesses for implant placement. In addition, the mandibular premolars site is one of the critical sites due to the presence of mental foramen.
In this study, we evaluate the accuracy of linear measurement in cross-sectional view with different slice thicknesses and in tangential view without slice thickness, because in tangential view, it is not related to different slice thicknesses but rather related to CBCT inherent accuracy of measurement
Materials and Methods
In this experimental study, we used 5 dry human mandibles with no gender priority. The exclusion criteria were severe resorption of alveolar crest and fracture. The distance between the highest tip of alveolar crest to the upper border of mental foramen was measured by digital caliper (± 0.01 mm) (Absolute- 1103, Insize, Germany). For more reliability, measurements were performed by two observers. The means of the physical measurements were calculated as the gold standard. Dry mandibles were placed in a plastic box of water with dimensions of 15 × 15 × 19 cm for the soft tissue simulation (Figure 1). The samples were placed on a tripod with adjustable heights. To ensure appropriate position of samples, the light localizer, which displays the midsagittal line, was used. The CBCT imaging was carried out by GALILEOS Comfort 3D imaging system (Sirona Dental System Inc., Bensheim, Germany) at 85kvp, 7 mA (42 mAs), with 14 seconds scan time. Next, the images were reconstructed by Sidex 3D software (Figure 2). Bilaterally, the distance between the highest tip of alveolar crest and special ruler of software measured upper border of mental foramen in cross-sectional view with 1, 3, 5, 7 and 9 mm slice thicknesses and tangential view (Figures 3 and 4). The exact location of selected cross-section view is where the mental nerve exits the mental foramen. Tangential is the Galileo’s term for a longitudinal view through the bone or tooth, parallel to the mesiodistal dimensions of the structures.
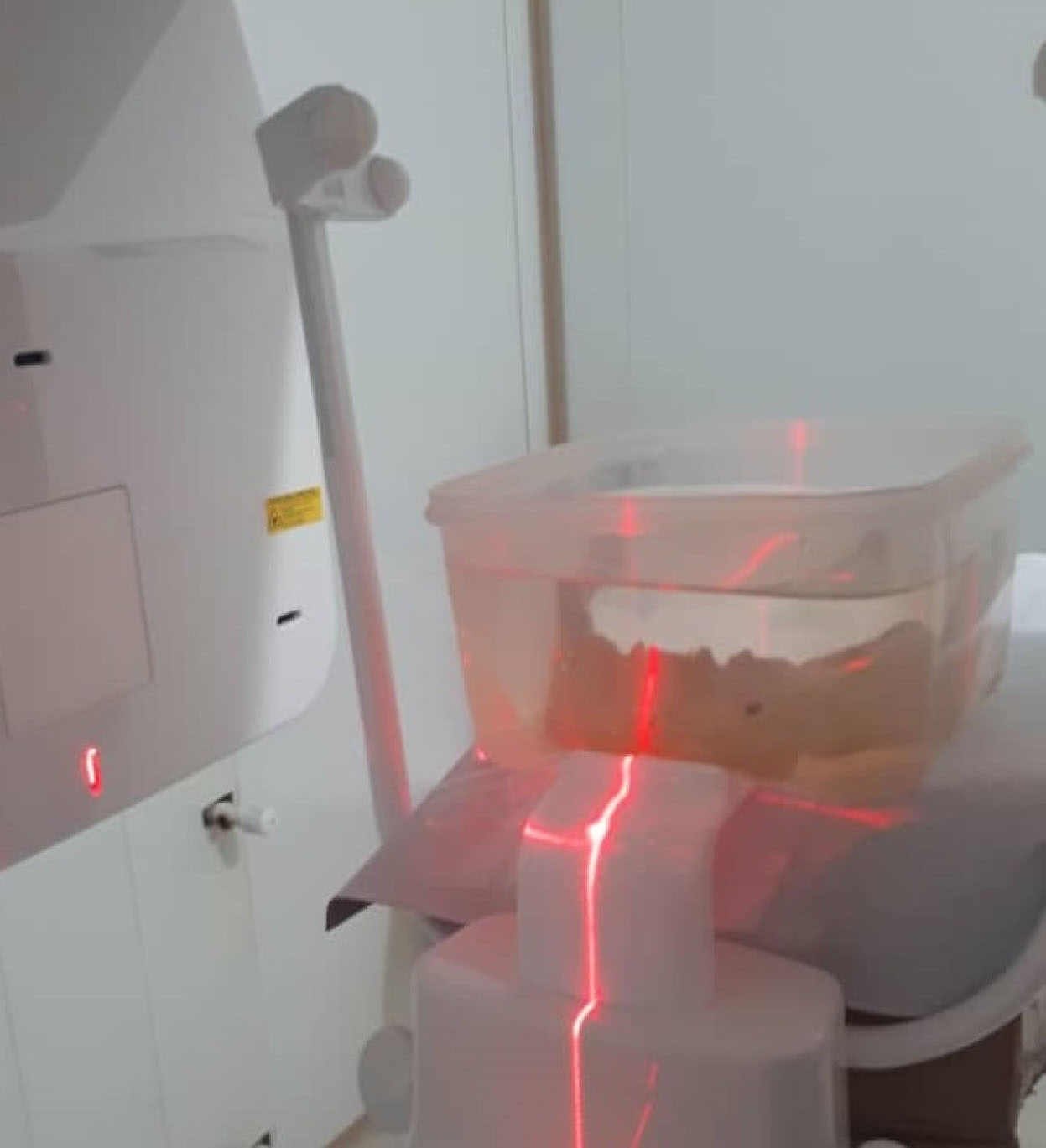
Figure 1.
Dry Mandible in Water Box Mounted for CBCT Imaging.
.
Dry Mandible in Water Box Mounted for CBCT Imaging.
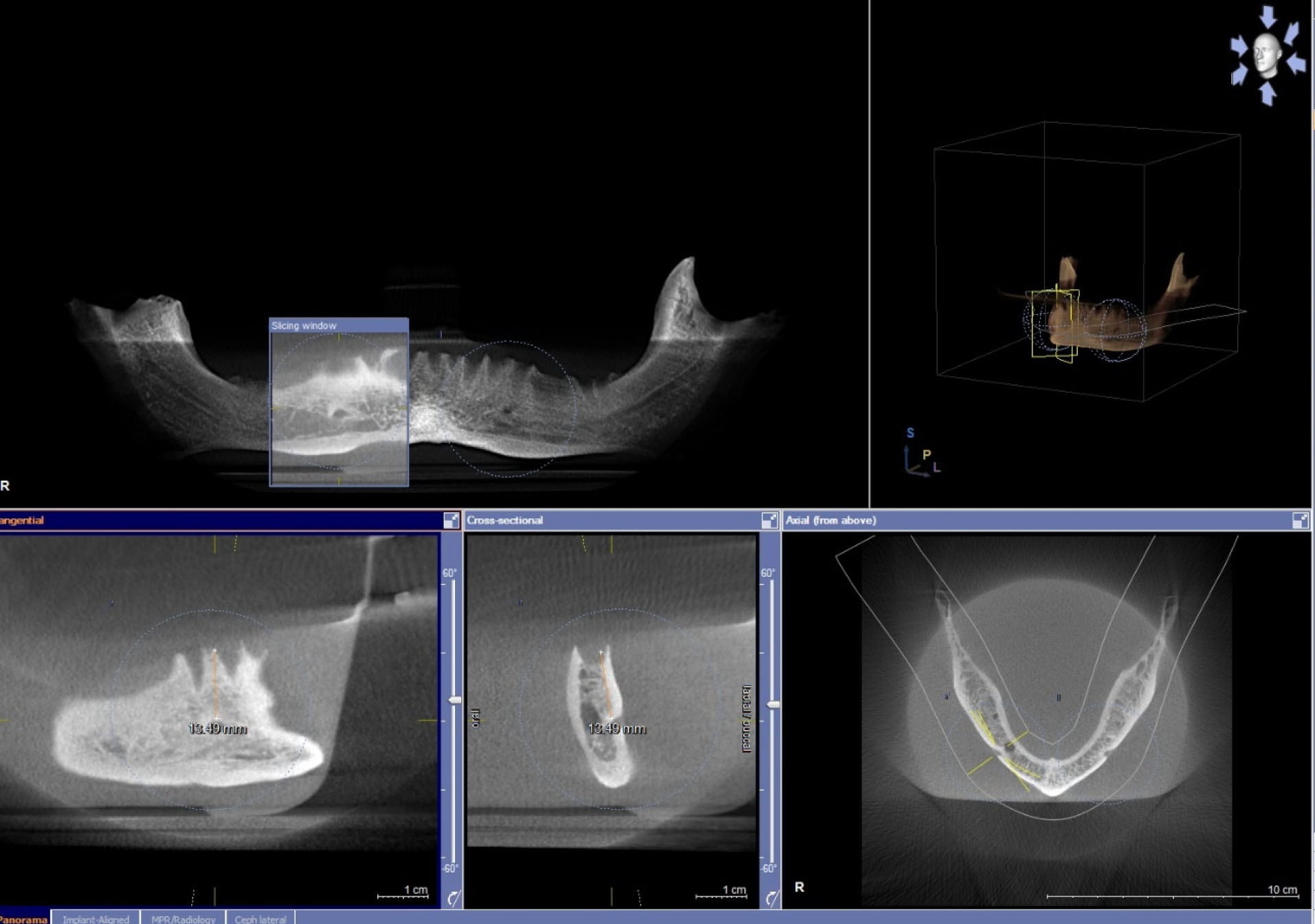
Figure 2.
The Radiographic Image of the Mandible Produced by the CBCT System.
.
The Radiographic Image of the Mandible Produced by the CBCT System.
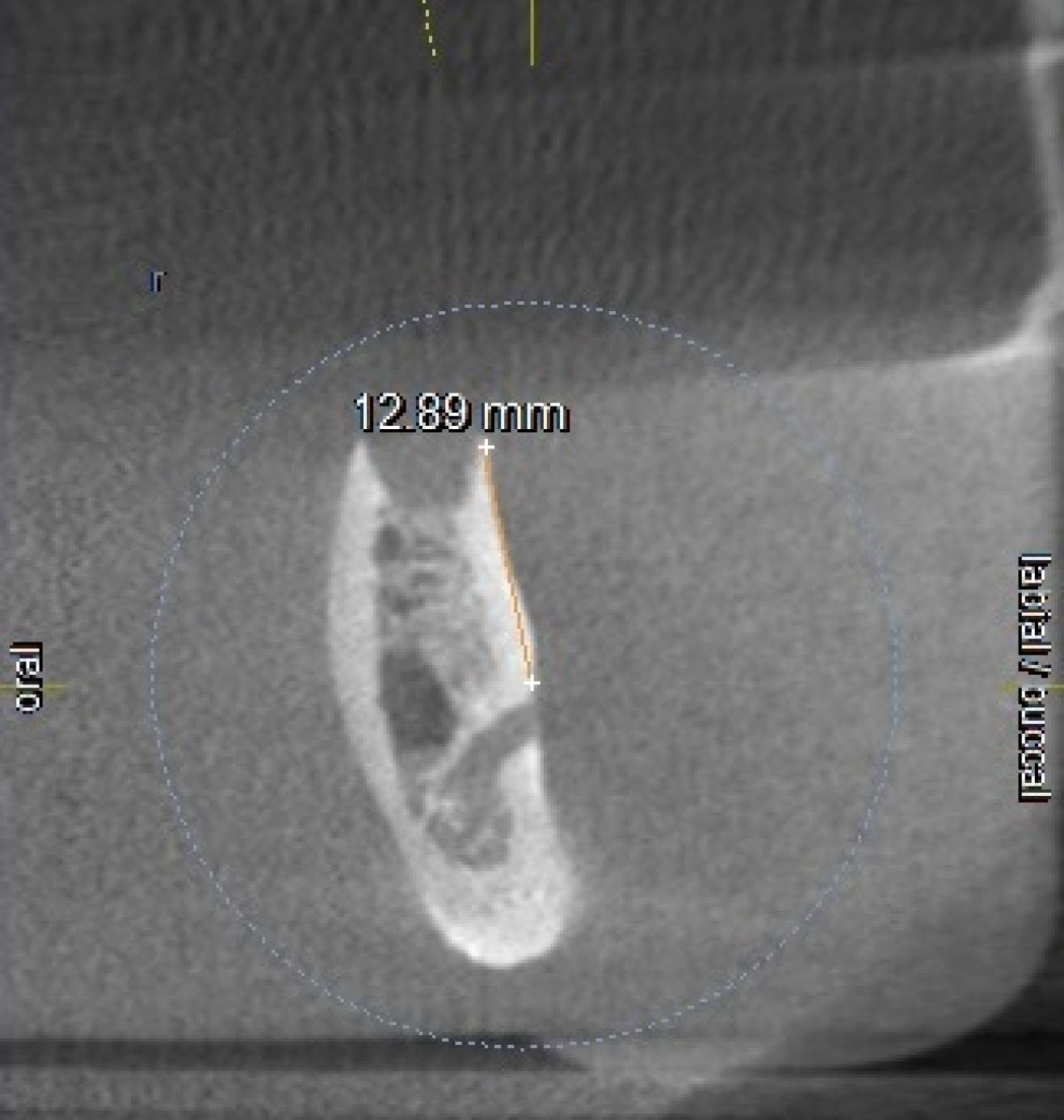
Figure 3.
Cross-sectional View of the Mandible and Linear Measurement from Highest Tip of Alveolar Crest to Mental Foramen.
.
Cross-sectional View of the Mandible and Linear Measurement from Highest Tip of Alveolar Crest to Mental Foramen.
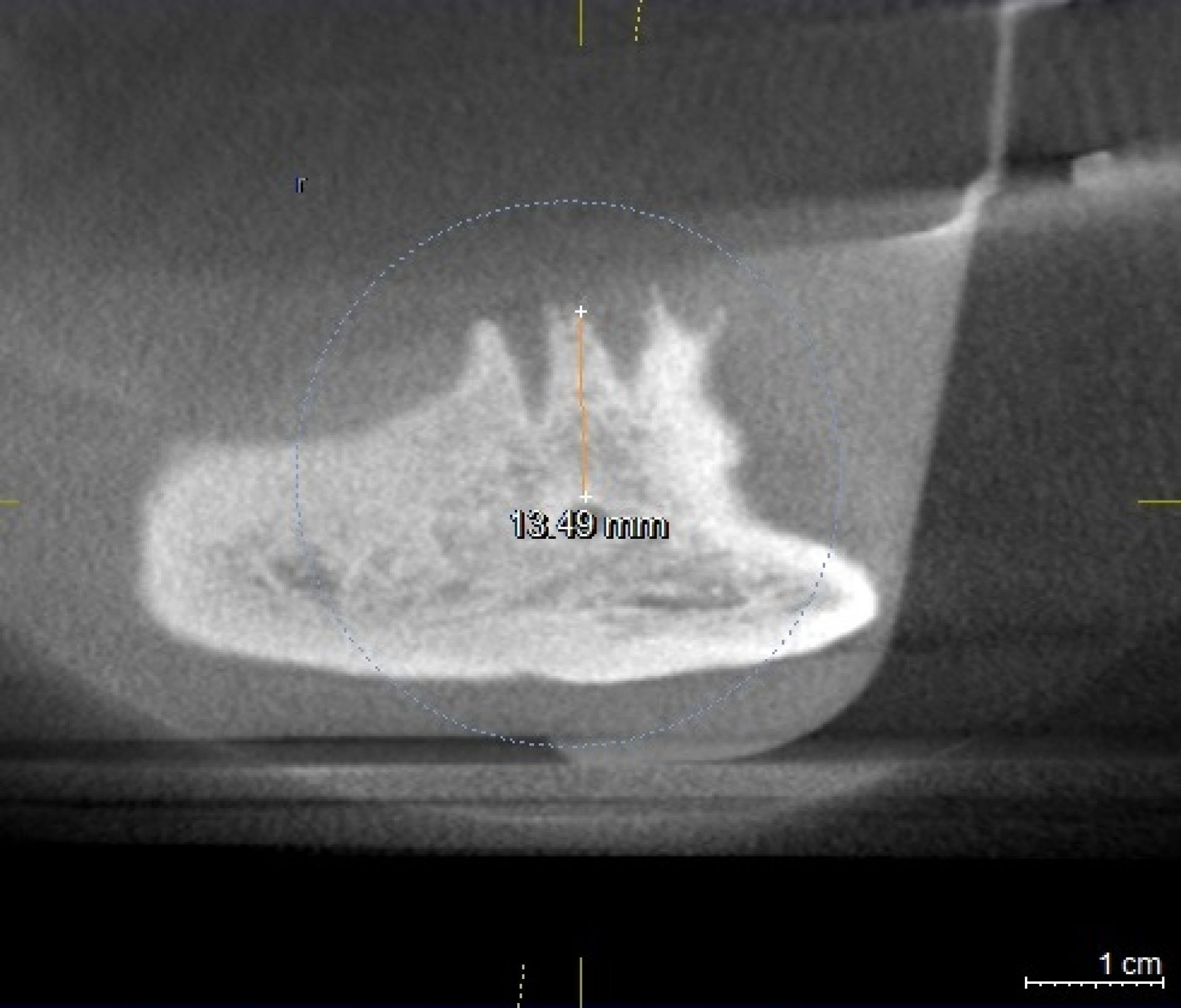
Figure 4.
Tangential View of the Mandible and Linear Measurement from Highest Tip of Alveolar Crest to Mental Foramen.
.
Tangential View of the Mandible and Linear Measurement from Highest Tip of Alveolar Crest to Mental Foramen.
Two observers, an oral and maxillofacial radiologist and a postgraduate student of oral and maxillofacial radiology, twice with an interval of 2 weeks, evaluated all the images. The collected data were analyzed by IBM SPSS Statistics version 22. The interclass correlation coefficient (ICC) was used to analyze intra-observer and inter-observer reliability measurements. Paired t test was used to compare the means of the measurements made with the gold standard. The statistical tests were carried out at significance level of 0.05.
Results
Totally, two observers made 240 measurements using CBCT machine at 1, 3, 5, 7, and 9 mm slice thicknesses in cross-sectional view and in tangential view. According to the ICC values, the inter-observer correlation was 0.926 (P < 0.001) and the intra-observer correlation was 0.945 (P < 0.001).
According to Table 1, the differences were significant only in the 1 mm option in cross-sectional view of the CBCT machine (P = 0.018) and in tangential view (P = 0.003). The differences between the mean value collected from the CBCT machine and the gold standard were not significant in other cases (P > 0.05).
Table 1.
Comparison of the Mean Bone Height Measured by Digital Caliper and CBCT Machine in Cross-sectional View at 1, 3, 5, 7, and 9 mm Options and in Tangential View
|
|
Mean (STD)
|
P
value
|
| Gold Standard |
14.7240 mm (1.59402) |
|
| 1 mm |
14.3210 mm (1.37796) |
0.018* |
| 3 mm |
14.3925 mm (1.37109) |
0.083 |
| 5 mm |
14.5660 mm (1.26777) |
0.383 |
| 7 mm |
14.6300 mm (1.29703) |
0.632 |
| 9 mm |
14.8665 mm (1.26169) |
0.359 |
| Tangential |
16.2040 mm (1.143118) |
0.003* |
Discussion
A precise measurement of bone at implant placement site is the key of success in implant surgeries (15). The CT and CBCT images are used to evaluate the height, width, and bone morphology in implant treatments (16). Due to the advantages of CBCT, such as lower radiation and lower cost, CBCT is preferred compared to the CT (17,18). CBCT measures the distance between alveolar crest and inferior alveolar nerve accurately, so the damage to the inferior alveolar nerve is reduced (17,19). Many clinicians tend to use the linear measurement capability of CBCT. However, the measurement errors lead to treatment failures (20,21).
In previous studies, CBCT was compared with CT, panoramic and digital radiography (17,18). The factor that differentiates this study from previous ones is that it compares the cross-sectional and tangential views, and evaluates the effect of different slice thicknesses on the measurement accuracy. In the current study, two observers carried out the measurements to increase the accuracy of measurement; statistical analysis showed no significant differences between two observers, and there was a high degree of matching between them. The accuracy of CBCT is evaluated in cross-sectional view with different slice thicknesses, and in tangential view. Comparing our results with the gold standard shows that the differences between the mean measurements made on CBCT images and the gold standard are significant only at 1 mm slices and tangential view. The differences between the mean measurements on the CBCT images and the gold standard are not significant in the other cases. The results show that, in slice thicknesses of less than 7 mm, the measurements are inclined toward underestimation. It is possible that some part of each voxel is not measured, since each voxel has a specific volume and the software measures the distance between the midpoints of the voxels of the volumetric images. Exact estimation needs very small voxel size, so the underestimation might be associated to voxel (3,11). The results showed that the 7 mm slice thickness is more accurate to determine the height of alveolar crest to the mental foramen.
At 9 mm slice thickness, the measurements are overestimated, increasing the slice thickness adjacent crest to be superimposed. These superimposed areas are located in one voxel, and as a result, the thin margin of cortical bone appear thicker. Thus, the measurement accuracy is decreased and the area under question is estimated larger than its actual size. By increasing the slice thickness, the noise increased, and with the disappearance of a sharp margin measurement, the accuracy decreased to some extent (16).
The overestimated measurements introduced in tangential view may be due to the convexity and concavity on the outer plate of the mandibular bone. It can cause changes in display of the jaw height in tangential view. In other words, the measurement accuracy decreased because the imaging of the highest tip of alveolar crest and the upper border of mental foramen at same plane is impossible.
Shokri et al (2) measured the accuracy of CBCT in 0.5, 1, 2, 3, 5, and 10 mm slice thicknesses and reported that there was no significant difference in bone width in any areas; but there were significant differences in bone height at the central and molars areas. The measurements were not significant only at 4 mm and 5 mm slice thickness options for height compared with the gold standard. The highest measurement accuracy at 4 mm slices was for bone width and at 5 mm slice thickness was for bone height. These results are different from the results of current study. In our study, the differences between the measurements made by CBCT and gold standard were significant only at 1 mm slices option, and tangential view. This difference might be due to the type of CBCT machine (2). The tangential view was not evaluated in the study by Shokri et al.
In most studies (9,22-24) the accuracy of CBCT was compared to other imaging or CBCT systems. Generally, the results showed that the accuracy of CBCT is high, and the slight difference from gold standard is due to the measurement errors with CBCT or caliper. In the current study, the results revealed that the cross-sectional imaging is preferred to the tangential view. In terms of slice thicknesses, the accuracy of measurements wre more accurate in thickness of 7 mm.
Previous studies have not evaluated the different views (cross-sectional and tangential) and different slice thicknesses.
Baumgaertel et al (11) reported that the measurements by CBCT devices are slightly less than the gold standard. The current study showed that the measurements are slightly less than the gold standard. However, in the mentioned study, the size of different landmarks was evaluated without the effect of different slice thicknesses.
In another study, Strateman et al (14) compared measurement accuracy of CBCT in two New Tom and Mercury devices and reported that both systems had acceptable accuracy and slight differences with gold standard. In addition, they reported that the accuracy of New Tom system is slightly better than Mercury system. In the present study, the differences between measurements made by the CBCT and gold standard were significant only in slice thickness of 1 mm and tangential view. Accordingly, it can be said that absence of total volume of the crest in voxel, in 1 mm slice, leads to underestimation.
In tangential view, the measurement accuracy decreased because imaging the tip of alveolar crest and the upper border of mental foramen simultaneously is impossible.
Sheikhi et al (13) reported that there were no significant differences between the measurements of central, premolars, and mandibular molars sites. In the present study, the measurements were carried out only at the mental foramen and the results showed that in thickness of less than 7 mm slice, measurements tended to be underestimated. This can be due to the measurement errors with CBCT or caliper. In slice thickness of 9 mm, the measurements were higher than the gold standard, but in general, the measurement error was less than 0.5 mm, and in cross-sectional view it was not clinically significant. However, in tangential view, the measurements had a tendency to be overestimated. The differences between the mean measurements in this view and the gold standard were more than 1 mm, which was clinically significant. In tangential view, it is not possible to display the outer surface of the mandible as a surface.
Chadwick and Lam (25) studied the bone height in various slice thicknesses and distances. Their results showed that there was a statistically significant difference between bone heights when slice thickness or inter-slice interval varied more than 1 mm (P = 0.005). Understanding the effects of slice thickness and inter-slice interval is important in the portrayal of both normal anatomy and pathoses in CBCT images.
Conclusions
Based on the results of current study, the tangential view is not appropriate for measuring bone height, and cross-sectional view is preferred. However, measurements are slightly less than the gold standard in slice thicknesses less than 7 mm.
Conflict of Interest Disclosures
The authors declare that they have no conflict of interests.
Ethical Statement
The Research Ethics Committee of Isfahan University of Medical Sciences approved this study (code: 394506).
Authors’ Contribution
MSH:Conceived and designed the analysis, supervised the paper
SASGH: Conceived and designed the analysis; collected the data;
contributed data or analysis tools;wrote the paper
MGH: performed the analysis; wrote the paper.
Funding
This research was supported by Isfahan University of Medical
Science. Grant No.394506.
References
- Kamburoğlu K, Kiliç C, Ozen T, Yüksel SP. Measurements of mandibular canal region obtained by cone-beam computed tomography: a cadaveric study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009; 107(2):e34-42. doi: 10.1016/j.tripleo.2008.10.012 [Crossref] [ Google Scholar]
- Shokri A, Khajeh S. In vitro comparison of the effect of different slice thicknesses on the accuracy of linear measurements on cone beam computed tomography images in implant sites. J Craniofac Surg 2015; 26(1):157-60. doi: 10.1097/scs.0000000000001031 [Crossref] [ Google Scholar]
- Lund H, Gröndahl K, Gröndahl HG. Accuracy and precision of linear measurements in cone beam computed tomography Accuitomo tomograms obtained with different reconstruction techniques. Dentomaxillofac Radiol 2009; 38(6):379-86. doi: 10.1259/dmfr/15022357 [Crossref] [ Google Scholar]
- Karjodkar FR. Implant radiology. In: Textbook of Dental and Maxillofacial Radiology. 2nd ed. New Delhi, IND: Jaypee; 2011. p. 881-928.
- Lofthag-Hansen S, Gröndahl K, Ekestubbe A. Cone-beam CT for preoperative implant planning in the posterior mandible: visibility of anatomic landmarks. Clin Implant Dent Relat Res 2009; 11(3):246-55. doi: 10.1111/j.1708-8208.2008.00114.x [Crossref] [ Google Scholar]
- Tantanapornkul W, Okouchi K, Fujiwara Y, Yamashiro M, Maruoka Y, Ohbayashi N. A comparative study of cone-beam computed tomography and conventional panoramic radiography in assessing the topographic relationship between the mandibular canal and impacted third molars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007; 103(2):253-9. doi: 10.1016/j.tripleo.2006.06.060 [Crossref] [ Google Scholar]
- Liu T, Xia B, Gu Z. Inferior alveolar canal course: a radiographic study. Clin Oral Implants Res 2009; 20(11):1212-8. doi: 10.1111/j.1600-0501.2009.01736.x [Crossref] [ Google Scholar]
- Rockenbach MI, Sampaio MC, da Costa LJ, da Costa NP. Evaluation of mandibular implant sites: correlation between panoramic and linear tomography. Braz Dent J 2003; 14(3):209-13. doi: 10.1590/s0103-64402003000300013 [Crossref] [ Google Scholar]
- Dreiseidler T, Mischkowski RA, Neugebauer J, Ritter L, Zöller JE. Comparison of cone-beam imaging with orthopantomography and computerized tomography for assessment in presurgical implant dentistry. Int J Oral Maxillofac Implants 2009; 24(2):216-25. [ Google Scholar]
- Gupta S, Patil N, Solanki J, Singh R, Laller S. Oral implant imaging: a review. Malays J Med Sci 2015; 22(3):7-17. [ Google Scholar]
- Baumgaertel S, Palomo JM, Palomo L, Hans MG. Reliability and accuracy of cone-beam computed tomography dental measurements. Am J Orthod Dentofacial Orthop 2009; 136(1):19-25. doi: 10.1016/j.ajodo.2007.09.016 [Crossref] [ Google Scholar]
- Gahleitner A, Hofschneider U, Tepper G, Pretterklieber M, Schick S, Zauza K. Lingual vascular canals of the mandible: evaluation with dental CT. Radiology 2001; 220(1):186-9. doi: 10.1148/radiology.220.1.r01jl05186 [Crossref] [ Google Scholar]
- Sheikhi M, Ghorbanizadeh S, Abdinian M, Goroohi H, Badrian H. Accuracy of linear measurements of galileos cone beam computed tomography in normal and different head positions. Int J Dent 2012; 2012:214954. doi: 10.1155/2012/214954 [Crossref] [ Google Scholar]
- Stratemann SA, Huang JC, Maki K, Miller AJ, Hatcher DC. Comparison of cone beam computed tomography imaging with physical measures. Dentomaxillofac Radiol 2008; 37(2):80-93. doi: 10.1259/dmfr/31349994 [Crossref] [ Google Scholar]
- Kobayashi K, Shimoda S, Nakagawa Y, Yamamoto A. Accuracy in measurement of distance using limited cone-beam computerized tomography. Int J Oral Maxillofac Implants 2004; 19(2):228-31. [ Google Scholar]
- White SC. Oral Radiology: Principles and Interpretation. 6th ed. St. Louis: Elsevier; 2009. p. 225-43.
- Gupta J, Ali SP. Cone beam computed tomography in oral implants. Natl J Maxillofac Surg 2013; 4(1):2-6. doi: 10.4103/0975-5950.117811 [Crossref] [ Google Scholar]
- Abramovitch K, Rice DD. Basic principles of cone beam computed tomography. Dent Clin North Am 2014; 58(3):463-84. doi: 10.1016/j.cden.2014.03.002 [Crossref] [ Google Scholar]
- Halperin-Sternfeld M, Machtei EE, Horwitz J. Diagnostic accuracy of cone beam computed tomography for dimensional linear measurements in the mandible. Int J Oral Maxillofac Implants 2014; 29(3):593-9. doi: 10.11607/jomi.3409 [Crossref] [ Google Scholar]
- Cavalcanti MG, Rocha SS, Vannier MW. Craniofacial measurements based on 3D-CT volume rendering: implications for clinical applications. Dentomaxillofac Radiol 2004; 33(3):170-6. doi: 10.1259/dmfr/13603271 [Crossref] [ Google Scholar]
- Marmulla R, Wörtche R, Mühling J, Hassfeld S. Geometric accuracy of the NewTom 9000 Cone Beam CT. Dentomaxillofac Radiol 2005; 34(1):28-31. doi: 10.1259/dmfr/31342245 [Crossref] [ Google Scholar]
- Sohrabi M. Comparative evaluation of linear measurement accuracy of CBCT, Spiral CBCT and digital panoramic techniques in the alveolar bone [dissertation]. 2008.
- Loubele M, Van Assche N, Carpentier K, Maes F, Jacobs R, van Steenberghe D. Comparative localized linear accuracy of small-field cone-beam CT and multislice CT for alveolar bone measurements. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008; 105(4):512-8. doi: 10.1016/j.tripleo.2007.05.004 [Crossref] [ Google Scholar]
- Suomalainen A, Vehmas T, Kortesniemi M, Robinson S, Peltola J. Accuracy of linear measurements using dental cone beam and conventional multislice computed tomography. Dentomaxillofac Radiol 2008; 37(1):10-7. doi: 10.1259/dmfr/14140281 [Crossref] [ Google Scholar]
- Chadwick JW, Lam EW. The effects of slice thickness and interslice interval on reconstructed cone beam computed tomographic images. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010; 110(4):e37-42. doi: 10.1016/j.tripleo.2010.05.008 [Crossref] [ Google Scholar]