Avicenna J Dent Res. 11(4):139-143.
doi: 10.34172/ajdr.2019.28
Original Article
The Ability of Different Observers in Measuring Dimensions of Objects and Cavities in Cone Beam-CT Images
Fatemeh Eskandarloo 1, Amir Eskandarloo 2, *  , Payam Amini 3
, Payam Amini 3
Author information:
1Dental Research Center, Research Institute of Dental Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2Department of Oral Radiology, School of Dentistry, Hamadan University of Medical Sciences, Hamadan, Iran.
3Department of Biostatistics and Epidemiology, School of Public Health, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
*
Correspondence to Amir Eskandarloo, Department of Oral Radiology, School of Dentistry, Hamadan University of Medical Sciences, Hamadan, Iran. Tel:+98-81-3838105, Email:
dr.eskandarloo@gmail.com
Abstract
Background: Accuracy of measurements obtained from cone-beam computed tomography (CBCT) images, which is a diagnostic tool in dentistry, is an important issue. The aim of this study was to compare the ability of different operators in measuring dimensions using CBCT software.
Methods: In this experimental study, 35 different areas using opaque objects and drilling cavities were prepared on 3 phantoms which were made from fresh beef ribs. Then each phantom was scanned by CBCT Promax 3D. The mentioned areas were measured on CBCT images 2 times with one week interval by four observer groups consisting two radiologists, two periodontists, two maxillofacial surgeons, and two general dentists. Obtained measurements from each group of observers were compared with those of other groups and also with measurements of a digital caliper as a gold standard by intra-class correlation coefficient (ICC). Then the measured dimensions, with respect to their application, were divided into three clusters including cluster 1: 2-7 mm, cluster 2: 7-16 mm, and cluster 3: more than 16 mm. t test was used to compare the mean value of each cluster with the mean value of the gold standard.
Results: In general, based on ICC, inter- and intra-observer agreement, agreement between observer groups, and agreement between each group and the gold standard were significant. The results of t test showed a significant difference between the mean value of data and that of gold standard in clusters 1 and 3.
Conclusions: Generally, high accuracy and reliability were reported for different specialists of dentistry and general dentists in measuring the dimensions of objects and cavities in CBCT images.
Keywords: Cone Beam-CT, Measurement, Observer
Copyright and License Information
© 2019 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Citation: Eskandarloo F, Eskandarloo A, Amini P. The Ability of Different Observers in Measuring Dimensions of Objects and Cavities in Cone Beam-CT Images. Avicenna J Dent Res. 2019;11(4):139-143. doi: 10.54172/ajdr.2019.28.
Background
Highlights
-
Accuracy of measurements obtained from CBCT images, which is a diagnostic tool in dentistry, is very important.
-
Providing enough adduction and correct training, accuracy and ability of different specialists of dentistry and even general dentists in measuring dimensions of objects and cavities in CBCT images also need attention.
-
High accuracy and reliability were reported by different specialists of dentistry and general dentists in measuring dimensions of objects and cavities in CBCT images.
There are various indications for the use of imaging in the field of dentistry and oral surgery. Radiographic examination is regarded as one of the important diagnostic tools in dental treatments (1). Cone-beam computed tomography (CBCT) was an innovation in maxillofacial imaging. It can produce a rapid volumetric image with a low-dose scan of the patient (low mA). CBCT provides multiple planar images of both jaws by a single rotational scan (2-5). This imaging system can provide 3-dimensional visualization of all tooth surfaces as digital images (6). CBCT is a user friendly and autorun software package. Many clinicians use the capability of linear measurement in measuring the distances between anatomic landmarks or measuring bone thickness for treatment planning and surgery. Therefore, any error could affect treatment processes (7-10). The reliability of radiographic angles, ratio, and length measurements are the key factors that contribute to the clinical decisions in treatment plans (11). CBCT can be used as a diagnostic tool that produces images with the actual anatomic size (12). In addition to the precision of CBCT, another problem is the accuracy of measurements that could be very different depending on who analyzes/measures it (11). For example, during surgery to place the implant, the positioning of implant and the measured areas need to be changed by the radiologist due to changes in the treatment plan or any other reason. In this case, surgeon or prosthetist should be able to interpret new positions from the perspective of length and width of bone and proximity to anatomic elements, as accurate as a radiologist (13). Some studies have evaluated the accuracy of linear measurements conducted using different CBCT systems (14). Some studies on the interpretation of information obtained from CBCT conducted by different radiologists and also by one radiologist at different times have not shown significant differences between measurements (1,15). There is no complete information about the accuracy of measurements gained from different specialists of dentistry in comparison with a radiologist. This research was therefore carried out given the importance of this issue and due to the lack of similar studies on the ability of specialists of different fields of dentistry in measuring dimensions of CBCT images in Hamadan, west of Iran.
Materials and Methods
Three phantoms were used in this experimental study. For producing these phantoms, using a hacksaw, some parts were made from fresh beef rib bone and these parts were placed in a wax mold formed as human mandible. In their different areas, by means of implant drills, some cavities with known height and diameter were made as lucent spaces for measuring purposes. Moreover, gutta-percha, extracted teeth, and titanium screws were used as opaque materials. Gutta-perchas were stuck to the buccal or lingual surfaces of phantom by a drip tape and teeth and titanium screws were placed into the bone (Figure 1). Overall, 35 areas were embedded in phantoms to be measured. Intended areas including height and diameter of each cavity at the upper side of the cavity, length of each gutta-percha and the distance between them, height and width of middle part of each titanium screw, and the biggest length of each tooth and the buccolingual width of them in the cementoenamel junction (CEJ) were measured twice within a week using a digital caliper with 0.01 mm accuracy as a gold standard and the average value was registered. Then, the phantoms were mounted on paraffin (Figure 2). All phantoms were scanned one by one using the CBCT Promax 3D device (Planmeca GmbH, Helsinki, Finland). To prepare the images, phantom was slightly fixed in a situation similar to its situation in the chin of a patient in chin rest and in a constant area with a field of view of the device. All of the prepared images were taken at 74kv, 10mA, 12s (120mAs) in 8*8 field of view and data of the device were reconstructed in Romexis software. For operating the Romexis software, each of the observers was trained and in order to consolidate, the how of measuring the intended areas was fully described to them. Measurements were made by two radiologists, two oral and maxillofacial surgeons, two periodontists, and two general dentists using the on-screen ruler in a 13-inch, 1600*900 resolution TFT LED-back light LCD monitor with AMD Radeon HD 6650M-1GB graphic processor, made in china in a room with appropriate light. Height and width of cavities, length of gutta-percha, height and width of screws, width of teeth in a cross-sectional view, distance of gutta-perchas in axial view, and length of teeth in panoramic view were measured (Figures 3-5). Measurement was made twice within a week by each observer and registered in a checklist.

Figure 1.
Prepared Phantom Before Mounting
.
Prepared Phantom Before Mounting

Figure 2.
Mounted Phantoms with Paraffin
.
Mounted Phantoms with Paraffin
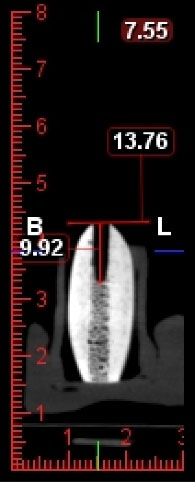
Figure 3.
Measurement of Prepared Cavity Length in Cross Sectional Image
.
Measurement of Prepared Cavity Length in Cross Sectional Image
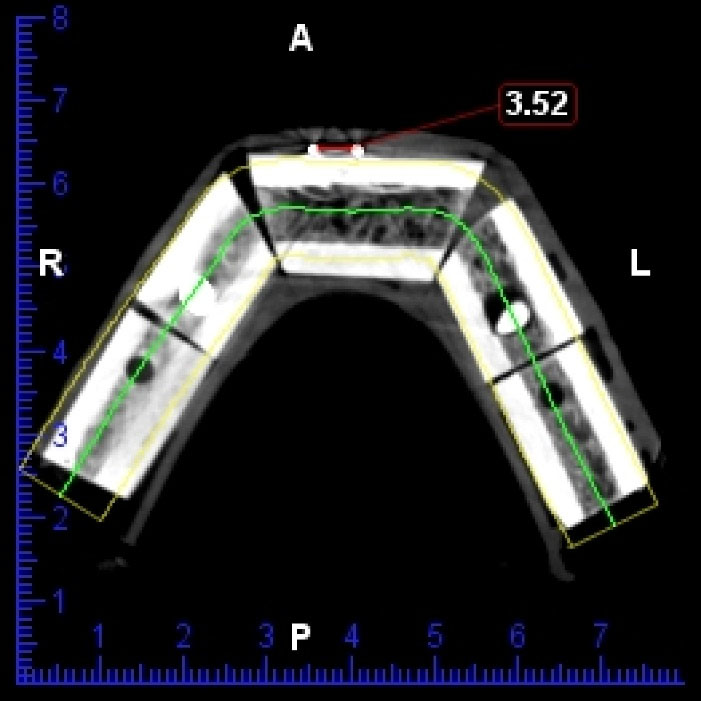
Figure 4.
Measurement of Distance Between Gutta Perchas in Axial Image
.
Measurement of Distance Between Gutta Perchas in Axial Image
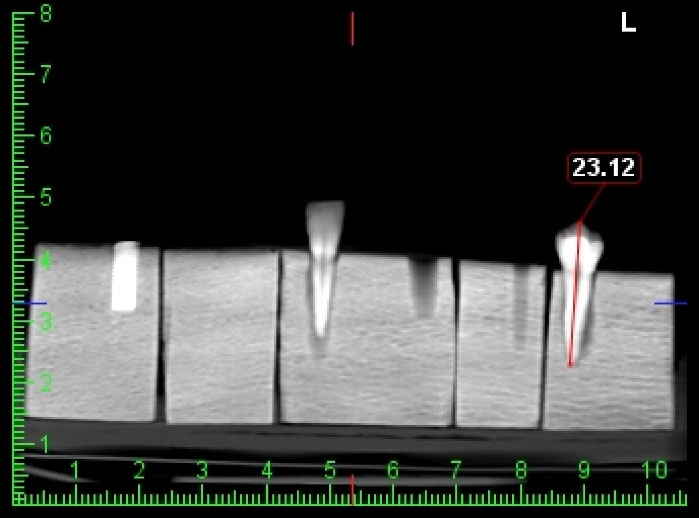
Figure 5.
Measurement of Tooth Length in Panoramic Like Image
.
Measurement of Tooth Length in Panoramic Like Image
Since the calculation of height and width of the ridge, the determinants of length and diameter of the implant, is necessary and since they are common areas measured in clinic, and considering the length and diameter of produced implants for analyzing the data achieved from this study, registered values were divided into 3 clusters including cluster 1: values from 2-7 mm, cluster 2: values from 7-16 mm, and cluster 3: values more than 16 mm. To investigate the reliability of obtained measurements from observers in each turn, and also to compare the observer groups to each other and to the gold standard, intra-class correlation coefficient (ICC) was employed once for each cluster and once for all the data. To demonstrate the presence or absence of difference between mean values of the clusters with each other, the ANOVA was used. Further, to investigate the reliability of mean values within all clusters and the gold standard, t-test was used.
Results
Generally, 16 values per area and 560 values overall was registered by observers and divided by the clusters. Results of ICC showed inter- and intra-observer agreement, agreement between observer groups and between each group and the gold standard (Tables 1 to 4). ANOVA results demonstrated a considerable statistical difference between the clusters (Table 5). Results from t-test showed that in clusters 1 and 3, unlike cluster 2, the mean values were significantly different (Tables 6 to 8).
Table 1.
Intra-observer Reliability
|
Reliability
|
Observer
|
Cluster 1
|
Cluster 2
|
Cluster 3
|
All
|
| Intra-observer |
Radiologist 1 |
0.98 |
0.99 |
0.99 |
0.99 |
| Radiologist 2 |
0.99 |
0.99 |
0.99 |
0.99 |
| Periodontist 1 |
0.94 |
0.99 |
0.97 |
0.99 |
| Periodontist 2 |
0.98 |
0.99 |
0.98 |
0.99 |
| Surgeon 1 |
0.98 |
0.99 |
0.99 |
0.99 |
| Surgeon 2 |
0.95 |
0.99 |
0.99 |
0.99 |
| General dentist 1 |
0.97 |
0.99 |
0.99 |
0.99 |
| General dentist 2 |
0.95 |
0.99 |
0.99 |
0.99 |
Table 2.
Inter-observer Reliability
|
Reliability
|
Observer
|
Cluster 1
|
Cluster 2
|
Cluster 3
|
All
|
| Inter-observer |
Radiologists |
0.98 |
0.99 |
0.99 |
0.99 |
| Periodontists |
0.98 |
0.99 |
0.97 |
0.99 |
| Surgeons |
0.97 |
0.99 |
0.99 |
0.99 |
| General dentists |
0.98 |
0.99 |
0.99 |
0.99 |
Table 3.
Reliability of Observer Groups in Relation With Gold Standard
|
Reliability
|
Observer group
|
Cluster 1
|
Cluster 2
|
Cluster 3
|
All
|
| Gold standard |
Radiology |
0.94 |
0.99 |
0.98 |
0.99 |
| Periodontology |
0.95 |
0.99 |
0.99 |
0.99 |
| Surgery |
0.94 |
0.99 |
0.98 |
0.99 |
| General dentists |
0.98 |
0.99 |
0.99 |
0.99 |
Table 4.
Reliability Between Observer Groups
|
Reliability
|
Observer group
|
Cluster 1
|
Cluster 2
|
Cluster 3
|
All
|
| Between groups |
Radiology and periodontology |
0.95 |
0.99 |
0.98 |
0.99 |
| Radiology and surgery |
0.98 |
0.99 |
0.98 |
.990 |
| Radiology and general dentists |
0.97 |
0.99 |
0.98 |
0.99 |
| Periodontology and surgery |
0.96 |
0.99 |
0.98 |
0.99 |
| Periodontology and general dentists |
0.96 |
0.99 |
0.99 |
0.99 |
| Surgery and general dentists |
0.98 |
0.99 |
0.99 |
0.99 |
Table 5.
ANOVA Results
|
Cluster
|
N
|
Mean
|
Standard Deviation
|
Minimum
|
Maximum
|
Sig. Between Clusters
|
| 1 |
208 |
4.3471 |
1.04692 |
2.54 |
6.11 |
0.001 |
| 2 |
240 |
11.0326 |
2.88085 |
6.40 |
16.32 |
| 3 |
112 |
20.4276 |
2.04389 |
16.27 |
23.63 |
Table 6.
Results of T Test for Cluster 1 Compared to 4.17 as Gold Standard
|
|
N
|
Mean
|
Standard Deviation
|
Sig. (2-tailed)
|
| R |
208 |
4.3471 |
1.04692 |
0.016 |
Table 7.
Results of T Test for Cluster 2 Compared to 11.12 as Gold Standard
|
|
N
|
Mean
|
Standard Deviation
|
Sig. (2-tailed)
|
| R |
240 |
11.0326 |
2.88085 |
0.639 |
Table 8.
Results of T Test for Cluster 3 Compared to 20.88 as Gold Standard
|
|
N
|
Mean
|
Std. Deviation
|
Sig. (2-tailed)
|
| R |
112 |
20.4276 |
2.04389 |
0.021 |
Discussion
Neither intraoral nor panoramic radiographs give the 3-dimensional information of the imaged area needed for pre-operative planning of dental implant placement. Therefore, special dental CBCT examinations have been used recently for this purpose (16). Applications of CBCT in maxillofacial imaging are increasing. Currently CBCT is commonly used for implantology, periodontics, temporomandibular joint pathology, airway analysis, and endodontics. Linear measurements are used for the quantitative analysis of the alveolar bone (height and width) (17). In this study, we considered the ability of specialists of different fields of dentistry and general dentists in accurate measurement of different dimensions. According to Tables 1-4, agreement between observers in each field and between observers of different fields, and their agreement with gold standard was evident. In a study conducted by Al-Ekrish and Ekram (18), dimensions of marked edentulous areas of human dry skulls were recorded from reformatted sections by two observers. There was a high inter- and intra-examiner reliability that was consistent with the results of our research. Accordingly, in the study of Ruellas et al (19), five observers repeated 12 linear measurements in CBCT scans of 10 patients within 10 days. The reliability of operators was high and in line with our results. De Santana Santos et al (13) conducted a study and used CBCT scans of 50 patients. Two examiners located some landmarks and linear measurements twice in images on different days. Corroborating our results, there was no significant difference between intra- and inter-examiners. Moshfeghi et al (17) aimed to evaluate the accuracy of linear measurements of CBCT. To this end, 15 radiographic linear measurements were made twice by three observers. High level of inter- and intra-observer reliability was achieved that was similar to the results of our study. Berco et al (15) and Suomalainen et al also came to the same results (16).
ICC was employed in the studies conducted for investigating the reliability of observers. All of them demonstrated high reliability of observers, confirming our results. In this study, in addition to ICC, t test was used to analyze the data including three clusters. As shown in Tables 6-88, in cluster 2, there was not a significant difference between the mean value and mean value of the gold standard, while in clusters 1 and 3, this difference was significant. In cluster 1, the difference might have been caused by small sizes and consequently difficulty of measuring accurate distance by observer’s hand. Moreover in cluster 3, the cause might have been the characteristics of measuring areas. For instance, the length of tooth comes in this cluster (more than 16 mm) and since a petty curvature is on apex of the tooth, there is possibility for lack of attention and misdiagnosis of the curvature in observer’s eyes that causes an inaccurate measurement. Generally at the range of named values (clusters 1 and 3), it seems more training is needed for observers.
Conclusions
Providing enough adduction and correct training, accuracy and ability of different specialists of dentistry and even general dentists, in measuring dimensions of objects and cavities in CBCT images, can be completely reliable.
Conflict of Interest Disclosures
The authors declare that they have no conflict of interests.
Ethical Statement
The ethics committee of Hamadan University of Medical Sciences approved this study.
Authors’ Contribution
The authors had the same contribution in this study.
References
- Tomasi C, Bressan E, Corazza B, Mazzoleni S, Stellini E, Lith A. Reliability and reproducibility of linear mandible measurements with the use of a cone-beam computed tomography and two object inclinations. Dentomaxillofac Radiol 2011; 40(4):244-50. doi: 10.1259/dmfr/17432330 [Crossref] [ Google Scholar]
- Ludlow JB, Davies-Ludlow LE, Brooks SL, Howerton WB. Dosimetry of 3 CBCT devices for oral and maxillofacial radiology: CB Mercuray, NewTom 3G and i-CAT. Dentomaxillofac Radiol 2006; 35(4):219-26. doi: 10.1259/dmfr/14340323 [Crossref] [ Google Scholar]
- Mozzo P, Procacci C, Tacconi A, Martini PT, Andreis IA. A new volumetric CT machine for dental imaging based on the cone-beam technique: preliminary results. Eur Radiol 1998; 8(9):1558-64. doi: 10.1007/s003300050586 [Crossref] [ Google Scholar]
- Sukovic P. Cone beam computed tomography in craniofacial imaging. Orthod Craniofac Res 2003; 6 Suppl 1:31-6. doi: 10.1034/j.1600-0544.2003.259.x [Crossref] [ Google Scholar]
- Tsiklakis K, Donta C, Gavala S, Karayianni K, Kamenopoulou V, Hourdakis CJ. Dose reduction in maxillofacial imaging using low dose Cone Beam CT. Eur J Radiol 2005; 56(3):413-7. doi: 10.1016/j.ejrad.2005.05.011 [Crossref] [ Google Scholar]
- Eskandarloo A, Saati S, Purabdolahi Ardakani M, Jamalpour M, Mezerji N and Akheshteh V. Diagnostic Accuracy of Three Cone Beam Computed Tomography Systems and Periapical Radiography for Detection of Fenestration Around Dental Implants. Contemp Clin Dent 2018; 9(3):376-381. doi: 10.4103/ccd.ccd_103_18 [Crossref] [ Google Scholar]
- Cavalcanti MG, Yang J, Ruprecht A, Vannier MW. Accurate linear measurements in the anterior maxilla using orthoradially reformatted spiral computed tomography. Dentomaxillofac Radiol 1999; 28(3):137-40. doi: 10.1038/sj/dmfr/4600426 [Crossref] [ Google Scholar]
- Cavalcanti MG, Yang J, Ruprecht A, Vannier MW. Accurate linear measurements in the anterior maxilla using orthoradially reformatted spiral computed tomography. Dentomaxillofac Radiol 1999; 28(3):137-40. doi: 10.1038/sj/dmfr/4600426 [Crossref] [ Google Scholar]
- Jacobs R. Preoperative radiologic planning of implant surgery in compromised patients. Periodontol 2000 2003; 33:12-25. doi: 10.1046/j.0906-6713.2002.03302.x [Crossref] [ Google Scholar]
- Marmulla R, Wörtche R, Mühling J, Hassfeld S. Geometric accuracy of the NewTom 9000 Cone Beam CT. Dentomaxillofac Radiol 2005; 34(1):28-31. doi: 10.1259/dmfr/31342245 [Crossref] [ Google Scholar]
- Segev E, Hemo Y, Wientroub S, Ovadia D, Fishkin M, Steinberg DM. Intra- and interobserver reliability analysis of digital radiographic measurements for pediatric orthopedic parameters using a novel PACS integrated computer software program. J Child Orthop 2010; 4(4):331-41. doi: 10.1007/s11832-010-0259-5 [Crossref] [ Google Scholar]
- Eskandarloo A, Abdinian M, Salemi F, Hashemzadeh Z, Safaei M. Effect of object location on the density measurement in cone-beam computed tomography versus multislice computed tomography. Dent Res J (Isfahan) 2012; 9(Suppl 1):S81-7. [ Google Scholar]
- de Santana Santos T, Gomes AC, de Melo DG, Melo AR, Cavalcante JR, de Araújo LC. Evaluation of reliability and reproducibility of linear measurements of cone-beam-computed tomography. Indian J Dent Res 2012; 23(4):473-8. doi: 10.4103/0970-9290.104952 [Crossref] [ Google Scholar]
- Katkar RA, Kummet C, Dawson D, Moreno Uribe L, Allareddy V, Finkelstein M. Comparison of observer reliability of three-dimensional cephalometric landmark identification on subject images from Galileos and i-CAT cone beam CT. Dentomaxillofac Radiol 2013; 42(9):20130059. doi: 10.1259/dmfr.20130059 [Crossref] [ Google Scholar]
- Berco M, Rigali PH Jr, Miner RM, DeLuca S, Anderson NK, Will LA. Accuracy and reliability of linear cephalometric measurements from cone-beam computed tomography scans of a dry human skull. Am J Orthod Dentofacial Orthop 2009; 136(1):17.e1-9. doi: 10.1016/j.ajodo.2008.08.021 [Crossref] [ Google Scholar]
- Suomalainen A, Vehmas T, Kortesniemi M, Robinson S, Peltola J. Accuracy of linear measurements using dental cone beam and conventional multislice computed tomography. Dentomaxillofac Radiol 2008; 37(1):10-7. doi: 10.1259/dmfr/14140281 [Crossref] [ Google Scholar]
- Moshfeghi M, Tavakoli MA, Hosseini ET, Hosseini AT, Hosseini IT. Analysis of linear measurement accuracy obtained by cone beam computed tomography (CBCT-NewTom VG). Dent Res J (Isfahan) 2012; 9(Suppl 1):S57-62. [ Google Scholar]
- Al-Ekrish AA, Ekram M. A comparative study of the accuracy and reliability of multidetector computed tomography and cone beam computed tomography in the assessment of dental implant site dimensions. Dentomaxillofac Radiol 2011; 40(2):67-75. doi: 10.1259/dmfr/27546065 [Crossref] [ Google Scholar]
- Ruellas AC, Koerich L, Baratieri C, Mattos CT, Alves M Jr, Brunetto D. Reliability of CBCT in the diagnosis of dental asymmetry. Dental Press J Orthod 2014; 19(2):90-5. doi: 10.1590/2176-9451.19.2.090-095.oar [Crossref] [ Google Scholar]