Avicenna J Dent Res. 11(2):61-65.
doi: 10.34172/ajdr.2019.11
Original Article
Evaluating the Iatrogenic Errors and the Quality of Root Canal Treatment of Mandibular Premolars in Ardabil Population Using the Cone Beam Computed Tomography in 2018
Ahmad Nouroloyouni 1, *  , Rohollah Basser 2, Zhila Salehi 3, Robab Farhang 4, Firooz Zadfattah 5, Milad Aghajani 6
, Rohollah Basser 2, Zhila Salehi 3, Robab Farhang 4, Firooz Zadfattah 5, Milad Aghajani 6
Author information:
1Assistant Professor, Department of Endodontics, Faculty of Dentistry, Ardabil University of Medical Sciences, Ardabil, Iran
2Assistant Professor, Department of Radiology, Faculty of Dentistry, Ardabil University of Medical Sciences, Ardabil, Iran
3Dentistry Student, Faculty of dentistry, Ardabil University of Medical Sciences, Ardabil, Iran
4Assistant Professor, Department of Endodontics, Faculty of Dentistry, Ardabil University of Medical Sciences, Ardabil, Iran
5Assistant Professor, Department of Endodontics, Faculty of Dentistry, Ardabil University of Medical Sciences, Ardabil, Iran
6Dentistry Student, Faculty of Dentistry, Ardabil University of Medical Sciences, Ardabil, Iran
Abstract
Background: Endodontic procedures such as root canal treatment (RCT) would be at the risk of failure like other medical interventions due to any unsuitable conditions. In this regard, applying low-efficiency techniques can cause several negative consequences such as errors in length, cleaning, shaping, and the quality of obturation. The aim of this study was to determine the iatrogenic errors and the quality of RCTs on mandibular premolars in the Ardabil population by using cone beam computed tomography (CBCT) images in 2018.
Methods: This cross-sectional retrospective study was carried out using the archive of Dr. Basser Radiology Center in 2018. The axial, coronal, and sagittal sections of CBCT images were observed for detecting missing canals, perforations, ledges, vertical root fractures (VRFs), and the quality of endodontic filling. The observation process was done by an endodontist, a radiologist, and a dentistry student. The collected data were analyzed using SPSS software, version 20 and the descriptive statistical method (frequency and percentage) was used for reporting the results.
Results: The results showed that underfilling was the most common error in the second and first mandibular premolar (9.5% compared with 9.2%), respectively. In addition, overfilling and missing canal were the second and third common errors in this study (6.3% and 3.9%). On the other hand, ledge, perforation, and VRF in the second premolar were the least common failures (0.26%). However, perforation and VRF were not found in the first mandibular premolars. It was observed that missing canals occur as lingual, mesial, and buccal types. All the missing canals of the first mandibular premolar were of lingual type. In comparison, in the second premolar, 71.4% of the missing canals were lingual and the remaining canals were mesial or buccal (each 14.3%).
Conclusions: Overall, the results of the present study revealed that the most common mistakes were errors in length and missing canals, therefore, more education is recommended toward employing working length determination techniques, using electric apex locator, obtaining more knowledge of anatomy variation, and using CBCT in doubtful cases.
Keywords: CBCT, Iatrogenic errors, Mandibular premolars, RCT
Copyright and License Information
© 2019 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Citation: Nouroloyouni A Basser R, Salehi ZH, Farhang R, Zadfattah F, Aghajani M. Evaluating the Iatrogenic Errors and the Quality of Root Canal Treatment of Mandibular Premolars in Ardabil Population Using the Cone Beam Computed Tomography in 2018. Avicenna J Dent Res. 2019;11(2):61-65. doi: 10.15171/ajdr.2019.11.
Background
Highlights
The bacterial elimination of the root canal system holds the key to successful endodontic treatment (1) and implementing a thorough and meticulous technique is considered as the primary determinant to achieve this aim and thus to prevent the future encroachment of bacteria. Therefore, the success rate can be as high as 94% when these measures are taken into account (2,3). In addition, the proper technique becomes more important in the presence of periapical infection (4). The thorough knowledge of the basic root canal anatomy and its possible variations is essential for achieving successful nonsurgical endodontic treatment (5). Previous research reported multiple foramina, fins, deltas, loops, furcations, and accessory canals in most teeth (5). The main reasons for endodontic failures are apical percolation and the presence of microorganisms caused by incomplete cleaning, insufficient canal obturation, and the presence of untreated canals (6). Anatomically lower second premolars are described as teeth with a single root and single root canal (7). However, they could be the most challenging teeth in terms of treatment due to the failure to identify the complex variations in their root canal morphology (8). This was well demonstrated by Chugal et al who showed that the failure rate increases by 14% for every 1 mm loss of working length in teeth with apical periodontitis (4). Certain errors represent a significant negative impact on the outcome. These procedural errors compromise canal cleaning and shaping, result in incomplete root filling, and jeopardize the outcome of the treatment (9) A poor technique can be manifested in numerous ways. These include errors in cleaning and shaping (i.e., ledge formation, apical transportation, perforations, and instrument separation) and obturation (i.e., voids, overfill, and underfill). The presence of such errors can lead to severe consequences (10). For instance, Sjögren et al reported that the length of the root filling, relative to the radiographic apex, significantly affected the outcome of root canal treatment (RCT) by 87%-94% healing rates associated with root fillings ending 0-2 mm from the radiographic apex (11-13). Underfill reduces the success rate to 68% (1,11-13,14). Similarly, overfill contributes to failure and reduces the success rate to as low as 76% (1,15). In addition, root fillings with a homogenous mass of filling material while with no voids are strongly correlated with a lower risk of disease (13,16). Instrument separation is also shown to reduce the success rate by up to 14% compared to those with no instrument separation (17,18). Further, preparation outcomes such as ledges and perforations are possible results of canal transportation, which is defined as any undesirable deviation from the natural canal path (15). Perforations are followed by the infection of the periodontal ligament and the alveolar bone, which thus impair the healing (19). A therapist would face a range of undesired and unexpected events and challenges, which could obviously affect disease prognosis. Accordingly, the knowledge and skill of doing the procedure are absolutely important for preventing or solving these kinds of problems (20). A study at the University of Washington assessed the failure rate of non-surgical root canal therapy in all teeth. Based on the results, the mandibular first premolar had the highest failure rate in the study at 11.45% (20). Considering the above-mentioned discussions, the present study aimed to determine the iatrogenic errors and the quality of RCTs of mandibular premolar teeth in Ardabil using the cone beam computed tomography (CBCT) images in 2018. The results of this work are expected to help practitioners to determine the steps of the endodontic procedure that require greater diligence. Most failures occur in mandibular premolars. In this way, it is possible for dental practitioners to substantially improve the quality of their work and ensure long-term viability of the treatment.
Materials and Methods
This cross-sectional retrospective study was performed at Dr. Basser Radiology Center in 2018 and the archive of CBCT images of this center was evaluated for this study. To this end, a total of 327 images of patients with the age of above 15 years were selected for the study. The sample size was estimated to be 327 according to Morgan’s table as there were 2180 CBCTs available. On the other hand, there was no similar study using CBCT for evaluating iatrogenic errors when conducting the study. The CBCT images with at least one mandibular root canal treated premolar were selected from the archive and were then checked by an endodontist, a radiologist, and a dentistry student. The axial, coronal, and sagittal sections of CBCT images were observed for detecting the missing canals, perforations, ledges, vertical root fractures (VRFs), and the quality of endodontic filling (Figure 1).
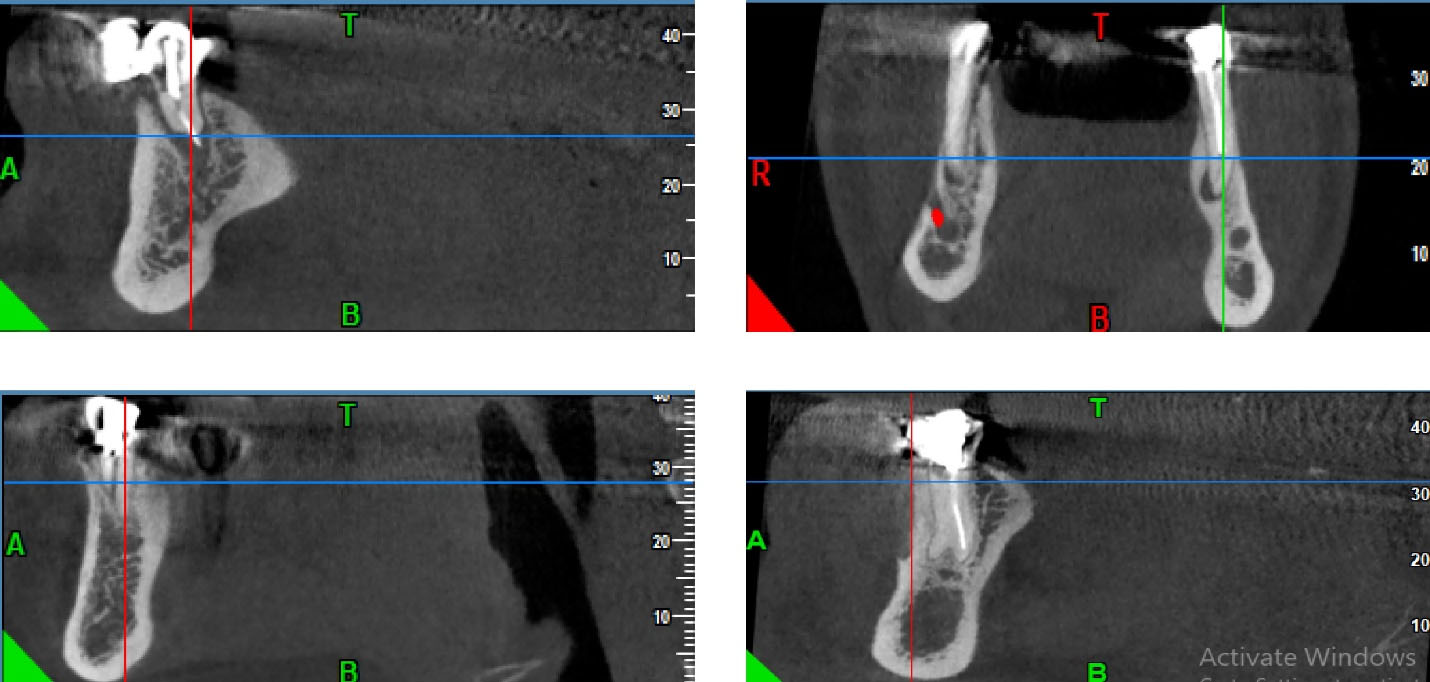
Figure 1.
(A) Overfilling, (B) Underfilling, (C) Vertical Root Fracture, and (D) Missing Canal.
.
(A) Overfilling, (B) Underfilling, (C) Vertical Root Fracture, and (D) Missing Canal.
Criteria for Radiographic Classification
Quality of root fillings:
-
A length of 2 mm from the apex (‘acceptable’ filling): Filling ending 0-2 mm short of the apex with uniform radiodensity and filling adaptation to the root canal walls;
-
Overfilling: Filling extruding beyond the apex;
-
Underfilling (a length of >2 mm from the apex): Filling ending more than 2 mm from the radiographic apex;
-
Detection of iatrogenic errors:
-
Ledge formation was diagnosed when the root filling was at least 1 mm shorter than the initial working length and deviated from the original canal shape in the teeth where root canal curvature occurred.
-
VRF is defined as a complete or incomplete fracture initiated from the root at any level, usually directed buccolingually.
-
Root resorption is a condition associated with either a physiologic or a pathologic process resulting in the loss of dentin or cementum.
-
Missing of the canal was diagnosed when not preparing a canal.
-
Root perforation was diagnosed when extrusion of filling material was detected in any other area of a root canal.
-
Presence of a separation instrument was diagnosed when a fractured instrument was detected inside a root canal.
Inclusion Criteria
At least one premolar of the mandible is treated endodontically.
Exclusion Criteria
Teeth with inter canal post or deep filling that can cause artifact.
Statistical Analysis
The obtained data were analyzed using SPSS software, version 20 and the descriptive statistical method (i.e., frequency and percentage) was used for reporting the results.
Results
A total number of 337 CBCT images were assessed in the present study. The obtained results are summarized in Table 1 and Figure 2. As shown, the most common error was underfilling in the second and first mandibular premolar (9.5% and 9.2%), respectively. In addition, overfilling and missing canal were the second and third common errors in this study (6.3% and 3.9%) and overfilling in the second mandibular premolar was higher than the first mandibular premolar (6.3% and 5.5%). This issue is contrariwise about missing. It was observed that missing canals occur as lingual, mesial, and buccal types. All the missing canals of the first mandibular premolar were lingual. In comparison, 71.4% of missing canals were lingual in the second premolar and the remaining canals were of mesial or Buccal type (each of them was 14. 3%). Ledge, perforation and VRF in the second premolar were the least common failures (0.26%). However, perforation and VRF were not found in the first mandibular premolars.
Table 1.
Percentage of Different Error Types in Endodontically Treated Mandibular Premolars
|
Error Type
|
Tooth Number
|
Abundance
|
Percentage
|
| Over Filling |
4 |
21 |
5.5 |
| 5 |
24 |
6.3 |
| Under Filling |
4 |
35 |
9.2 |
| 5 |
36 |
9.5 |
| Missing Canal |
4 |
15 |
3.9 |
| 5 |
7 |
1.9 |
| Ledge |
4 |
2 |
0.53 |
| 5 |
1 |
0.26 |
| Root Resorbtion |
4 |
5 |
1.3 |
| 5 |
3 |
0.8 |
| Perforation |
4 |
- |
- |
| 5 |
1 |
0.26 |
| Vertical Root Fracture |
4 |
- |
- |
| 5 |
1 |
0.26 |
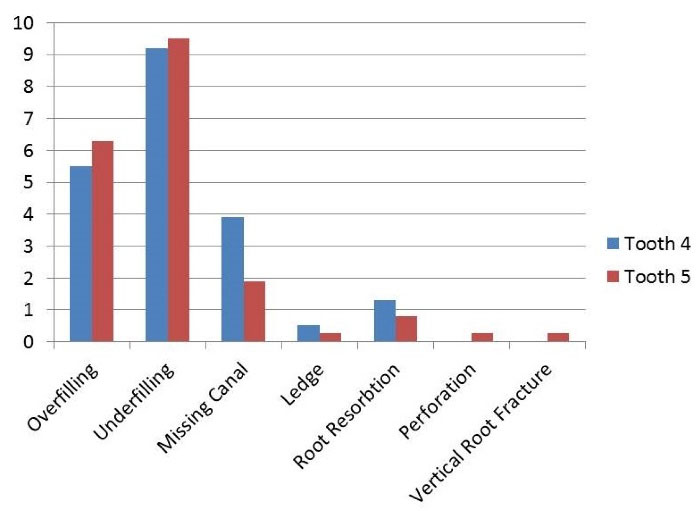
Figure 2.
Percentage of Different Error Types in Endodontically Treated Mandibular Premolars.
.
Percentage of Different Error Types in Endodontically Treated Mandibular Premolars.
Discussion
This study was designed to evaluate the iatrogenic errors and the quality of the RCT of mandibular premolars among the Ardabil population by using CBCT in 2018. CBCT was used to investigate iatrogenic errors in endodontic treatments since periapical radiographs have limitations. In other words, they provide two-dimensional images of three-dimensional objects. The result of this study showed that underfilling in the second and first premolar was the most frequency of errors, respectively, which is in line with the results Lynch and Burke (21). This is probably because of the tooth location and complexity of root canals in the second mandibular premolar. In our study, overfilling was less than underfilling, which corroborates the results of the study by Eleftheriadis and Lambrianidis (22), Khabbaz et al (23), Lynch and Burke (21), and Ilgüy et al (24). According to Eleftheriadis and Lambrianidis (22), Khabbaz et al (23), and Lynch and Burke (21), the radiographically working length of root canal filling in our study was defined when obturation was finished zero to two millimeters of the radiographic apex. However, in the study by Ilgüy et al (24), obturation position in more than 1 mm short or long of the radiographic apex was defined as under- or over-filling, respectively. It appears that working length determination requires further attention in the process of instruction. However, it must be noted that errors in obturation are mostly secondary to errors in canal preparation.
The missing canal was the third common error type in this study. More abundance of missing canals was expected in these teeth (3.9%) considering that the probability of the existence of the second canal in the first premolars was more than that of the second premolars (Table 1). The more complex topology of canals in mandibular second premolars compared to those in the first premolars is responsible for the diversity of missing canals. Therefore, the missing canals of the second premolars consist of three types (i.e., lingual, mesial, and buccal) unlike the first premolar (all missing canals were lingual due to the curve of lingual root canals and difficult accessing to these canals).
Of 327 evaluated images, ledge error in the first premolar (0.53%) and second premolar (0.26%) had a low percentage of errors that was close to the study of Vukadinov et al (25) 2.8% and less than 54.8% and 26% in the studies of Khabbaz et al (23) and Mozayeni et al (26). Our findings regarding the ledge had a significant difference with the findings of the other studies, which is because the present study only evaluated premolar teeth since the root curvature of these teeth is low. As regards the technique of preparation, however, four studies (21,25,27,28) presented some characteristics that possibly contributed to this fact, including the use of flexible instruments and the absence of significant curvatures. It can be further the result of different used radiography techniques and the small deviation from the original canal shape can be more obvious in Periapical (PA) images due to less artifact of the filling material in these images.
The less frequency was related to perforation and VRF. VRFs relate to different factors like the amount of remaining tooth structure, the amount of pressure in endodontic treatment, and the like, therefore, the more percentage of this error in the second premolar is iatrogenic and seem not to be related to the tooth type.
The root resorption of the first premolars was more than that of the second ones. The only explanation for this observation can be remained inflammation due to technical problems in the first premolars since the etiology of root resorption is not completely known.
Totally, the results of this study that focused on the iatrogenic errors of premolar teeth showed that underfilling, overfilling, and missing errors have a higher prevalence in the second mandibular premolars. Thus, more education is needed for correct obturation without under or overfilling in these teeth.
Conclusions
Considering the limitations of the present study, the most common error types were underfilling in the second mandibular premolars and then the first mandibular premolar. Furthermore, overfilling and missing canal were the second and third common error types in this study thus more education is recommended regarding applying working length determination techniques, using an electric apex locator, as well as obtaining more knowledge about anatomy variation and using CBCT in doubtful cases.
The ledge in the second premolar, perforation, and VRF in the first premolar were least common and no perforation and VRF were found in the first mandibular premolars. Generally, problems were more prevalent in the second premolar and more education is needed for root canal therapy of this tooth.
Conflict of Interest Disclosures
The authors declare no competing interests concerning the authorship and/or publication of this article.
Ethics Statement
The ethics approval for this study was achieved from the Ethics Committee of Ardebil University of Medical Sciences with the online code of IR.ARUMS.REC.1397.265.
Funding
This article was funded by Ardabil University of Medical Sciences.
Acknowledgment
The authors would like to thank Dr. Hessam Mikaili Xiavi for his cooperation with this study.
References
- Lin LM, Skribner JE, Gaengler P. Factors associated with endodontic treatment failures. J Endod 1992; 18(12):625-7. doi: 10.1016/s0099-2399(06)81335-x [Crossref] [ Google Scholar]
- Benenati FW, Roane JB, Biggs JT, Simon JH. Recall evaluation of iatrogenic root perforations repaired with amalgam and gutta-percha. J Endod 1986; 12(4):161-6. doi: 10.1016/s0099-2399(86)80055-3 [Crossref] [ Google Scholar]
- Gutmann JL, Lovdahl PE. Problem Solving in Endodontics. 5th ed. China: Elsevier Mosby; 2011. p. 198-239.
- Mukhaimer R. Radiographic technical quality of root canal fillings performed by dental students in Palestine. Indian J Oral Sci 2013; 4(2):55-63. doi: 10.4103/0976-6944.119927 [Crossref] [ Google Scholar]
- Fuss Z, Trope M. Root perforations: classification and treatment choices based on prognostic factors. Endod Dent Traumatol 1996; 12(6):255-64. doi: 10.1111/j.1600-9657.1996.tb00524.x [Crossref] [ Google Scholar]
- Noor N, Maxood A, Kaleem K. Cross-sectional analysis of endodontic failure in PIMS. Pak Oral Dent J 2008; 28:99-102. [ Google Scholar]
- Ray HA, Trope M. Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. Int Endod J 1995; 28(1):12-8. doi: 10.1111/j.1365-2591.1995.tb00150.x [Crossref] [ Google Scholar]
- Simon S, Machtou P, Tomson P, Adams N, Lumley P. Influence of fractured instruments on the success rate of endodontic treatment. Dent Update 2008; 35(3):172-4, 6, 8. doi: 10.12968/denu.2008.35.3.172 [Crossref] [ Google Scholar]
- Torabinejad M, Walton RE. Principle and Practice of Endodontics. 4th ed. China: Saunders; 2009. p. 221-46.
- Kerekes K, Tronstad L. Long-term results of endodontic treatment performed with a standardized technique. J Endod 1979; 5:83-90. [ Google Scholar]
- Eriksen HM, Bjertness E, Orstavik D. Prevalence and quality of endodontic treatment in an urban adult population in Norway. Endod Dent Traumatol 1988; 4(3):122-6. doi: 10.1111/j.1600-9657.1988.tb00309.x [Crossref] [ Google Scholar]
- Saunders WP, Saunders EM, Sadiq J, Cruickshank E. Technical standard of root canal treatment in an adult Scottish sub-population. Br Dent J 1997; 182(10):382-6. doi: 10.1038/sj.bdj.4809394 [Crossref] [ Google Scholar]
- Eleftheriadis GI, Lambrianidis TP. Technical quality of root canal treatment and detection of iatrogenic errors in an undergraduate dental clinic. Int Endod J 2005; 38(10):725-34. doi: 10.1111/j.1365-2591.2005.01008.x [Crossref] [ Google Scholar]
- Crump MC, Natkin E. Relationship of broken root canal instruments to endodontic case prognosis: a clinical investigation. J Am Dent Assoc 1970; 80(6):1341-7. doi: 10.14219/jada.archive.1970.0259 [Crossref] [ Google Scholar]
- Sjogren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endod 1990; 16(10):498-504. doi: 10.1016/s0099-2399(07)80180-4 [Crossref] [ Google Scholar]
- Cheung GSP. Instrument fracture: mechanisms, removal of fragments, and clinical outcomes. Endod Topics 2007; 16(1):1-26. doi: 10.1111/j.1601-1546.2009.00239.x [Crossref] [ Google Scholar]
- Segura-Egea JJ, Jiménez-Pinzón A, Poyato-Ferrera M, Velasco-Ortega E, Ríos-Santos JV. Periapical status and quality of root fillings and coronal restorations in an adult Spanish population. Int Endod J 2004; 37(8):525-30. doi: 10.1111/j.1365-2591.2004.00826.x [Crossref] [ Google Scholar]
- Siqueira JF Jr, Rôças IN. Clinical implications and microbiology of bacterial persistence after treatment procedures. J Endod 2008; 34(11):1291-301. doi: 10.1016/j.joen.2008.07.028 [Crossref] [ Google Scholar]
- Vertucci F, Haddix J, Brito L. Tooth Morphology and Access Cavity Preparation. 9th ed. St Louis, Mo, USA: Mosby; 2006.
- Ingle J, Bakland L. Endodontics. 5th ed. Hamilton, New Zealand: BC Decker; 2002.
- Lynch CD, Burke FM. Quality of root canal fillings performed by undergraduate dental students on single-rooted teeth. Eur J Dent Educ 2006; 10(2):67-72. doi: 10.1111/j.1600-0579.2006.00397.x [Crossref] [ Google Scholar]
- Eleftheriadis GI, Lambrianidis TP. Technical quality of root canal treatment and detection of iatrogenic errors in an undergraduate dental clinic. Int Endod J 2005; 38(10):725-34. doi: 10.1111/j.1365-2591.2005.01008.x [Crossref] [ Google Scholar]
- Khabbaz MG, Protogerou E, Douka E. Radiographic quality of root fillings performed by undergraduate students. Int Endod J 2010; 43(6):499-508. doi: 10.1111/j.1365-2591.2010.01706.x [Crossref] [ Google Scholar]
- Ilgüy D, Ilgüy M, Fisekçioglu E, Ersan N, Tanalp J, Dölekoglu S. Assessment of root canal treatment outcomes performed by Turkish dental students: results after two years. J Dent Educ 2013; 77(4):502-9. [ Google Scholar]
- Vukadinov T, Blažić L, Kantardžić I, Lainović T. Technical quality of root fillings performed by undergraduate students: a radiographic study. ScientificWorldJournal 2014; 2014:751274. doi: 10.1155/2014/751274 [Crossref] [ Google Scholar]
- Mozayeni MA, Asnaashari M, Modaresi SJ. Clinical and radiographic evaluation of procedural accidents and errors during root canal therapy. Iran Endod J 2006; 1(3):97-100. [ Google Scholar]
- Kulić L, Nogo-Živanović D, Krunić J, Vujašković M, Stojanović N. Radiological assessment of the quality of root canal fillings in teeth endodontically treated at students’ practical sessions. Stomatol Glas Srb 2011; 58(3):139-46. doi: 10.2298/SGS1103139K [Crossref] [ Google Scholar]
- Rafeek RN, Smith WA, Mankee MS, Coldero LG. Radiographic evaluation of the technical quality of root canal fillings performed by dental students. Aust Endod J 2012; 38(2):64-9. doi: 10.1111/j.1747-4477.2010.00270.x [Crossref] [ Google Scholar]