Avicenna J Dent Res. 17(3):160-166.
doi: 10.34172/ajdr.2276
Original Article
Comparative Effects of Premedication With Acetaminophen Versus Ketorolac on Postoperative Pain in 4–7-Year-Old Children Undergoing Dental Treatment Under General Anesthesia: A Parallel Triple-Blind Randomized Clinical Trial
Nastaransadat Mahdavi Conceptualization, Investigation, Methodology, Project administration, Supervision, 1 
Fahimeh Kooshki Conceptualization, Investigation, Methodology, Project administration, Supervision, Writing – review & editing, 2
Ali Asghar Soleimani Methodology, Supervision, 2
Mansooreh Soltani Writing – original draft, Writing – review & editing, 2, *
Boshra Alimoradi Data curation, Investigation, 3
Farid Zayeri Data curation, Formal analysis, Validation, 4
Author information:
1Department of Anesthesiology, School of Medicine, Mofid Children’s Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2Department of Pediatric Dentistry, School of Dentistry, Shahid Beheshti University of Medical Sciences, Tehran, Iran
3Private Practice, Tehran, Iran
4Proteomics Research Center and Department of Biostatistics, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Abstract
Background: Pain is the most common complication of dental procedures under general anesthesia in children. Premedication with analgesics can decrease the need for intraoperative and postoperative analgesic administration. This study compared the effects of premedication with acetaminophen versus ketorolac on postoperative pain in 4–7-year-old children undergoing dental treatment under general anesthesia.
Methods: This parallel triple-blind randomized clinical trial was conducted on 100 children requiring dental procedures under general anesthesia. The children were randomly allocated to two groups (n=50) by block randomization with size 4 blocks for premedication with either 10–12 mg/kg acetaminophen or 0.5 mg/kg ketorolac immediately after the onset of general anesthesia and before the onset of the dental procedure. The two groups were standardized regarding type of dental procedure, duration of anesthesia, age, and gender. The heart rate (HR), systolic blood pressure (SBP), and peripheral capillary oxygen saturation (SPO2) were recorded before and after the treatment. The pain intensity of patients was quantified at recovery time and 2 hours later using the Wong-Baker FACES Pain Rating Scale. The data were analyzed by the chi-square test, t-test, marginal modeling, and generalized estimating equations.
Results: No significant difference existed in the mean pain score between the two groups during the recovery time (P=0.494), but the pain score was significantly lower in the ketorolac group after 2 hours (P=0.009). The mean reduction in the pain score within 2 hours was only significant in the ketorolac group (P=0.002).
Conclusion: Acetaminophen and ketorolac were both effective for the reduction of postoperative pain in 4–7-year-old children undergoing dental treatment under general anesthesia, but ketorolac was significantly more effective after 2 hours.
Keywords: Acetaminophen, Anesthesia, Dental care for children, Pain, Premedication, Ketorolac
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Mahdavi N, Kooshki F, Soleimani AA, Soltani M, Alimoradi B, Zayeri F. Comparative effects of premedication with acetaminophen versus ketorolac on postoperative pain in 4–7-year-old children undergoing dental treatment under general anesthesia: a parallel triple-blind randomized clinical trial. Avicenna J Dent Res. 2025;17(3):160-166. doi:10.34172/ajdr.2276
Background
Pain is a prevalent complication after dental procedures. It is a complex, multifactorial phenomenon with a subjective nature (1). Over 70% of patients complain of pain after dental procedures, and over 25% complain of side effects after the consumption of analgesics (2). Pain control is a common concern for dental clinicians and patients. Postoperative pain can cause sleep disturbances, respiratory depression, cough, and sputum formation (2).
Dental treatment under general anesthesia is a well-accepted approach for children who cannot be managed by other commonly practiced behavioral control methods. According to the American Academy of Pediatric Dentistry, the indications for dental treatment under general anesthesia include uncooperative and emotionally or physiologically immature patients, those with mental retardation or physical disability, medically compromised patients, cases with local anesthesia contraindications (e.g., acute infection, anatomical variations, or allergy), and highly uncooperative and anxious patients that require urgent treatment (3,4). In addition, uncooperative children with extensive caries that need several long treatment sessions often require dental treatment under general anesthesia (5-7). The main advantages of dental treatment under general anesthesia include the provision of more efficient treatment with minimal discomfort and mental and physical stress for patients and dental clinicians (8).
The complications of dental procedures under general anesthesia in children vary widely (9-11). Pain is the most common complication that requires analgesic intake post-treatment (9-11). O’Donnell et al (12) suggested a diclofenac suppository for this purpose (12). Sleep disturbances in the first night after general anesthesia are also common (13-15). Nausea and vomiting are among the side effects of opioids that may occur after general anesthesia. Holt et al (10) reported that 21% of patients had nausea, and 20% had vomiting after general anesthesia. Psychological problems, such as crying, sleep disturbances, nightmares, eating problems, postoperative epistaxis, sore throat, and hoarseness, have been reported as well (16,17). Many factors, such as age, underlying systemic diseases, patients’ dental needs, experience of the personnel, type of premedication, difficult intubation, duration of anesthesia, and the administered anesthetic agents, can affect the occurrence and severity of postoperative complications (18-21).
A wide range of analgesics may be used for pain control, including opioids, alpha-2-agonists, non-steroidal anti-inflammatory drugs (NSAIDs), and anti-convulsant medications; further, a combination of drugs is often preferred to monotherapy (22). Acetaminophen and intravenous ketorolac are two non-opioid analgesic agents that are successfully used for pain control after dental procedures worldwide (22-24). Acetaminophen was approved by the United States Food and Drug Administration for monotherapy for the alleviation of mild to moderate pain, and in combination with opioids for the alleviation of moderate to severe pain. Ketorolac gained the United States Food and Drug Administration approval in 1989 (23,24). Ketorolac is an NSAID with analgesic properties that inhibits both the lipoxygenase and cyclooxygenase pathways and can be administered orally or intravenously.
Premedication with analgesics can decrease the need for intraoperative and postoperative analgesic administration (25,26). It has been suggested that premedication with acetaminophen or NSAIDs, such as ketorolac, may decrease postoperative pain and complications (27). Considering the scarcity of clinical trials in this regard, this study aims to compare the effects of premedication with acetaminophen versus ketorolac on postoperative pain in 4–7-year-old children receiving dental treatment under general anesthesia.
Materials and Methods
This parallel triple-blind randomized clinical trial was conducted at Mofid Children’s Hospital in Tehran from August 2023 to July 2024. The ethical code (IR.SBMU.DRC.REC.1402.071) was obtained from Shahid Beheshti University of Medical Sciences, and the clinical trial registration code was IRCT20240408061442N1.
Trial Design
A parallel triple-blind randomized clinical trial was designed in which one group underwent premedication with acetaminophen, while the other group underwent premedication with ketorolac before undergoing general anesthesia for dental treatment. The Consolidated Standards of Reporting Trials were used to report the results.
Participants, Eligibility Criteria, and Settings
The inclusion criteria were children aged 4–7 years with Class I general health status (according to the American Society of Anesthesiologists (ASA) physical status classification system) whose parents consented to their participation in the study and to dental treatment under general anesthesia requiring the extraction of 2–3 teeth or pulpotomy of 1–3 teeth and a mean surgery duration of 2.5–3 hours. All procedures were performed by the same dental clinician.
The exclusion criteria were children with specific needs and those with underlying conditions such as heart disease, diabetes mellitus, or intellectual retardation.
Totally, 100 children presenting to Mofid Children’s Hospital for dental treatment under general anesthesia who were selected by convenience sampling were enrolled in this study.
Interventions
Following parental consent, demographic information of children was recorded, and they were allocated to two groups (n = 50) for premedication with either 10–12 mg/kg acetaminophen or 0.5 mg/kg ketorolac immediately after the onset of general anesthesia and before the onset of the dental procedure (injections were performed only once). The two groups were standardized regarding type of dental procedure, duration of anesthesia, age, and gender. All children were clinically examined by a pedodontist one day before the procedure. The children had to fast for at least 6 hours prior to the procedure. They received 5.0 mg oral midazolam as premedication prior to entering the operating room. Subsequently, they received 1–2 µg fentanyl, and nasal intubation was performed after anesthesia induction with 2 mg/kg propofol and 0.5 mg/kg atracurium (a muscle relaxant). After anesthesia induction and maintenance with isoflurane and oxygen, 10–12 mg/kg acetaminophen or 0.5 mg/kg ketorolac was injected, depending on the group allocation of children, prior to the onset of the dental procedure. No local anesthetic was administered. The heart rate (HR), systolic blood pressure (SBP), and peripheral capillary oxygen saturation (SPO2) of children were recorded at the onset of the dental procedure (baseline) and after the completion of treatment. SPO2 was measured by the pulse oximeter of a heart-lung monitoring machine (Alborz B5; Saadat, Iran). SBP was measured by a small BP monitor cuff for children (Alborz B5; Saadat, Iran), and HR was also estimated by the heart-lung monitoring machine (Alborz B5; Saadat, Iran). After regaining consciousness (evidenced by eye opening, a normal deglutition reflex, and normal respiration), the children were transferred to the recovery room. The pain level of patients was recorded in the recovery room and 2 hours later using the Wong-Baker FACES Pain Rating Scale. The Wong-Baker Faces Pain Rating Scale is a famous scale for self-reporting of pain, first introduced in 1980. Its validity and reliability have been confirmed in several previous studies (28,29). This scale includes six faces, with a happy face at one end showing “no pain at all” and a crying face at the other end showing “worst pain possible”. The faces are scored from 0 to 10. A trained operator not involved in any step of the study showed this scale to children after they completely regained their consciousness in the recovery room and 2 hours later and asked them to express their pain level by selecting a face (28,29).
Outcomes
Postoperative pain was the primary outcome, while HR, SBP, and SPO2 were the secondary outcomes.
Sample Size Calculation
The sample size was calculated to be 38 patients in each group according to a pilot study, assuming the standard deviation of the pain score 2 hours after recovery to be 2 in both groups, α = 0.05 β = 0.1, and a significant mean difference of 1.5 units in pain score between the two groups, according to the following formula:
Considering a 20% dropout, 45 patients had to be recruited in each group. However, by further increasing the sample size, beta would decrease, and study power would increase. Thus, due to the availability of more samples, a larger sample size was recruited to increase the power, and 50 patients were selected for each group.
Interim Analyses and Stopping Guidelines
None.
Randomization
The patients were randomly allocated to the groups using random blocks of size 4 (30), according to the randomization chapter of the book authored by Pocock (30). Six different states of blocks with size 4 were first considered, and then random numbers were created between 1 and 6 to choose the blocks using the https://www.sealedenvelope.com/randomisation/ website.
In any way, with any number of blocks, the last number of each block would be predictable. To solve this problem, randomization and allocation concealment were performed by someone not involved in any phase of the study using sealed envelopes.
Blinding
The study had a triple-blind design. The children, their parents, the operating dentist, and the researcher were all blinded to the type of premedication, and only the anesthesiologist who administered the medications was aware of their type. Acetaminophen and ketorolac were injected by the anesthesiologist in coded, identical syringes. Thus, the children, their parents, and the dentist were all unaware of the content of the syringes. Moreover, the information of the participants was provided to the statistician in two code groups; thus, the statistician was also blinded to the group allocation of children.
Statistical Analysis
The normality of the quantitative data was assessed by the Shapiro-Wilk test, which showed normal distribution of data (P > 0.05). Accordingly, the chi-square was utilized to compare the categorical variables between the two groups. Further, paired samples and independent samples t-test were used to compare the quantitative outcomes within and between the groups, respectively, due to their normal distribution. In addition, regarding the repeated measures of the outcomes, comparisons between the groups were made using the marginal modeling and generalized estimating equations (31). All statistical analyses were conducted using SPSS, version 26.0 (SPSS Inc., IL, USA) at a 0.05 level of significance. It should be noted that all analyses were outcome-based.
Results
Participant Flow and Baseline Analysis
The sample consisted of 50 patients in each group. The acetaminophen group included 27 girls (54%) and 23 boys (46%), while the ketorolac group included 23 girls (46%) and 27 boys (54%) (Figure 1). The two groups had no significant difference in gender distribution (P =0.356). The mean age was 5.22 ± 1.13 years and 5.06 ± 1.03 years in the acetaminophen and ketorolac groups, respectively. The two groups were not significantly different in terms of the mean age (P =0.513).
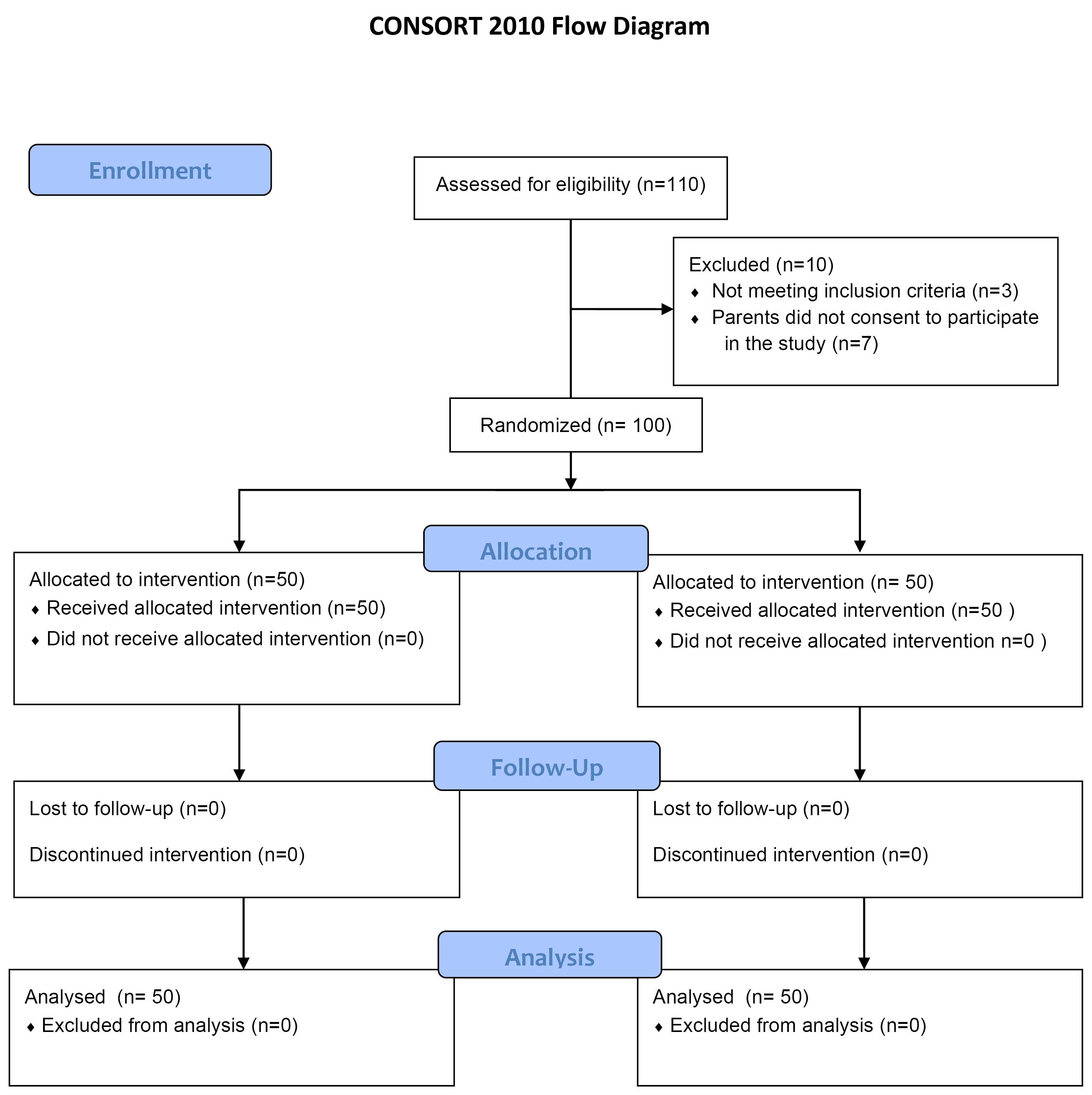
Figure 1.
CONSORT Flow Diagram of Patient Selection and Allocation. Note. CONSORT: Consolidated Standards of Reporting Trials
.
CONSORT Flow Diagram of Patient Selection and Allocation. Note. CONSORT: Consolidated Standards of Reporting Trials
Harms
No patients were harmed during the study.
Subgroup Analyses
Primary Outcomes
Pain: Independent samples t-test (Table 1) demonstrated no significant difference in the mean pain score between the two groups during the recovery time (P =0.494). However, this difference was significant after 2 hours and was significantly lower in the ketorolac group (P =0.009).
Table 1.
Comparisonof Mean Pain Score in the Two Groups
|
Time
|
Acetaminophen
|
Ketorolac
|
P
Value*
|
| Recovery |
5.10 ± 2.20 |
4.80 ± 2.18 |
0.494 |
| Two hours |
4.53 ± 2.15 |
3.40 ± 2.07 |
0.009 |
| Change |
0.57 ± 3.19 |
1.40 ± 3.00 |
0.186 |
|
P value** |
0.216 |
0.002 |
- |
Note.*Between groups; **Within group.
Based on the results of the paired samples t-test, the mean reduction in the pain score within 2 hours was not significant in the acetaminophen group (P =0.216). However, this reduction was significant in the ketorolac group (P =0.002). Children in the ketorolac group reported significantly lower pain levels (Table 1). The reduction in pain score was not significantly different between the two groups (P =0.186).
The generalized estimating equation (Table 2) revealed that children in the acetaminophen group experienced, on average, 0.3 units more pain than the ketorolac group; this difference was not significant (P= 0.488). Within 2 hours after recovery, the mean pain score decreased by an average of 1.4 units in the acetaminophen group. At 2 hours after recovery, patients in the acetaminophen group experienced on average 0.83 units more pain than those in the ketorolac group; nonetheless, this difference was not significant (P= 0.179).
Table 2.
The Results of Generalized Estimating Equation Regarding the Effect of Group and Time on the Pain Score
|
Variable
|
Group
|
Estimate*
|
SE
|
P
Value
|
| Group |
Acetaminophen |
0.302 |
0.436 |
0.488 |
| Ketorolac |
Ref. Cat. |
| Time |
- |
-1.400 |
0.421 |
0.001 |
| Group-time |
Acetaminophen |
0.829 |
0.617 |
0.179 |
| Ketorolac |
Ref. Cat. |
Note. SE: Standard error. *The estimation column shows the estimated coefficients of model parameters in the applied marginal model.
Secondary Outcomes
Heart Rate, Systolic Blood Pressure, and Peripheral Capillary Oxygen Saturation: The results of the independent samples t-test (Table 3) indicated that the two groups had no significant difference in the HR, SBP, or SPO2 at any time point (P> 0.05).
Table 3.
HR and Systolic BP of Patients in the Two Groups Before and After the Procedure
|
Variable
|
Acetaminophen
|
Ketorolac
|
P
Value
|
| SBP at baseline (mm Hg) |
1.40 ± 7.59* |
1.34 ± 7.67 |
0.772 |
| HR at baseline |
9.59 ± 107.90 |
8.63 ± 107.90 |
1.000 |
| SPO2 at baseline (%) |
0.69 ± 99,38 |
0.77 ± 99.34 |
0.786 |
| SBP post-treatment (mm Hg) |
1.53 ± 7.55 |
1.31 ± 7.38 |
0.559 |
| HR post-treatment |
8.34 ± 110.12 |
8.98 ± 111.16 |
0.550 |
| SPO2 post-treatment (%) |
0.74 ± 99.24 |
0.77 ± 99.12 |
0.431 |
Note. *Mean ± standard deviation; HR: Heart rate; SBP: Systolic blood pressure; SPO2: Peripheral capillary oxygen saturation
Discussion
This study assessed the effects of premedication with acetaminophen versus ketorolac on postoperative pain in 4–7-year-old children undergoing dental treatment under general anesthesia. The results showed that the two groups did not have any significant difference in the physiological parameters of HR, SBP, and SPO2 at any time point or the pain score after treatment. Time had a significant effect on the pain score, such that the pain decreased 2 hours after treatment in the acetaminophen and ketorolac groups. Previous studies have also shown successful analgesic efficacy of acetaminophen and ketorolac as monotherapy and in combination with opioids for the management of postoperative pain (25,32,33). However, the majority of studies on acetaminophen and ketorolac evaluated their analgesic efficacy for post-surgical pain management in adults, and it was impossible to compare our results due to the scarcity of studies on pain control in children (34-37).
Erkmen Almaz et al (38) observed that the frequency of pain in children 24 hours after general anesthesia was lower than 1.5%, which is in accordance with the current findings. However, some others reported the high frequency of pain in children after dental treatment under general anesthesia. For example, Ghafournia et al (39) concluded that toothache was the most frequent non-psychological postoperative complication. Deng et al (40) found similar results. Based on the findings of Keles and Kocaturk (41), 90% of children who underwent pulpotomy under general anesthesia had immediate postoperative pain with variable degrees. Chen et al (42) reported toothache and cough as the main postoperative complications in children that lasted for more than 24 hours. Gharavi and Soltani (43) found restlessness, vomiting, and pain as postoperative complications that were resolved after 96 hours. Our results contradict those of most of the aforementioned studies, likely because premedication with analgesics was not used in those studies.
Kharouba et al (44) assessed the analgesic efficacy of prophylactic premedication with paracetamol, ibuprofen, and placebo in children and concluded that children who received premedication with paracetamol or ibuprofen had lower odds of requiring analgesics post-treatment compared with those who received placebo, which conforms to the current findings. Alhashemi and Daghistani (45) evaluated the analgesic efficacy of intravenous administration of acetaminophen intraoperatively versus the intramuscular injection of meperidine and reported that children in the meperidine group had a significantly lower level of pain than those in the acetaminophen group. The pain was resolved within 10 hours after the procedure in both groups, which is in line with our findings.
A review study on the efficacy of premedication with analgesics prior to dental surgical procedures revealed that the administration of NSAIDs increases the success of analgesia by inhibiting the cyclooxygenase pathways and production of prostaglandins (46). Hasheminia et al (47) investigated the effect of the subcutaneous injection of ketorolac versus dexamethasone on post-surgical dental pain and observed that the mean pain score in both groups was the same but significantly lower than that of the control group, which corroborates the findings of the present study. Rao and Kumar (22) compared the analgesic efficacy of acetaminophen and ketorolac for the management of pain after tooth extraction. They reported that 10 mg ketorolac was significantly more effective than 500 mg acetaminophen, which contradicts our results.
This study evaluated children aged 4–7 years. Future studies with a larger sample size on older children are required, using different pain assessment scales.
Conclusion
Acetaminophen and ketorolac were both effective in reducing postoperative pain in 4–7-year-old children undergoing dental treatment under general anesthesia, but ketorolac was significantly more effective after 2 hours.
Acknowledgements
The authors would like to thank Mofid Children’s Hospital and the Faculty of Dentistry of Shahid Beheshti University of Medical Sciences for their support.
Competing Interests
The authors certify that they have no conflict of interests.
Ethical Approval
This study was approved by the Committee of Ethics of the School of Dentistry of Shahid Beheshti University of Medical Sciences (IR.SBMU.DRC.REC.1402.071).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
- Shoar S, Esmaeili S, Safari S. Pain management after surgery: a brief review. Anesth Pain Med 2012; 1(3):184-6. doi: 10.5812/kowsar.22287523.3443 [Crossref] [ Google Scholar]
- Meghana S, Manpreet S, Dheeraj K. Pain management in orthopaedic surgeries. Pb J Orthop 2012; 13(1):9-30. [ Google Scholar]
- American Academy on Pediatric Dentistry Ad Hoc Committee on Sedation and Anesthesia; American Academy on Pediatric Dentistry Council on Clinical Affairs. Policy on the use of deep sedation and general anesthesia in the pediatric dental office. Pediatr Dent. 2008;30(7 Suppl):66-7.
- O'Sullivan EA, Curzon ME. The efficacy of comprehensive dental care for children under general anesthesia. Br Dent J 1991; 171(2):56-8. doi: 10.1038/sj.bdj.4807603 [Crossref] [ Google Scholar]
- Lee PY, Chou MY, Chen YL, Chen LP, Wang CJ, Huang WH. Comprehensive dental treatment under general anesthesia in healthy and disabled children. Chang Gung Med J 2009; 32(6):636-42. [ Google Scholar]
- Al-Eheideb AA, Herman NG. Outcomes of dental procedures performed on children under general anesthesia. J Clin Pediatr Dent 2003; 27(2):181-3. doi: 10.17796/jcpd.27.2.k3307186n7086r11 [Crossref] [ Google Scholar]
- Almeida AG, Roseman MM, Sheff M, Huntington N, Hughes CV. Future caries susceptibility in children with early childhood caries following treatment under general anesthesia. Pediatr Dent 2000; 22(4):302-6. [ Google Scholar]
- Eidelman E, Faibis S, Peretz B. A comparison of restorations for children with early childhood caries treated under general anesthesia or conscious sedation. Pediatr Dent 2000; 22(1):33-7. [ Google Scholar]
- Reuter NG, Westgate PM, Ingram M, Miller CS. Death related to dental treatment: a systematic review. Oral Surg Oral Med Oral Pathol Oral Radiol 2017;123(2):194-204.e10. doi: 10.1016/j.oooo.2016.10.015.
- Holt RD, Chidiac RH, Rule DC. Dental treatment for children under general anaesthesia in day care facilities at a London dental hospital. Br Dent J 1991; 170(7):262-6. doi: 10.1038/sj.bdj.4807504 [Crossref] [ Google Scholar]
- Enever GR, Nunn JH, Sheehan JK. A comparison of post-operative morbidity following outpatient dental care under general anaesthesia in paediatric patients with and without disabilities. Int J Paediatr Dent 2000; 10(2):120-5. doi: 10.1046/j.1365-263x.2000.00180.x [Crossref] [ Google Scholar]
- O'Donnell A, Henderson M, Fearne J, O'Donnell D. Management of postoperative pain in children following extractions of primary teeth under general anaesthesia: a comparison of paracetamol, voltarol and no analgesia. Int J Paediatr Dent 2007; 17(2):110-5. doi: 10.1111/j.1365-263X.2006.00800.x [Crossref] [ Google Scholar]
- Prabhu N, Nunn JH, Enever GR. A comparison of factors in pre-anaesthetic dental assessment and post-operative outcomes following dental care under general anaethesia in a group of disabled and anxious patients. J Disabil Oral Health 2003; 4:3-8. [ Google Scholar]
- Vinckier F, Gizani S, Declerck D. Comprehensive dental care for children with rampant caries under general anaesthesia. Int J Paediatr Dent 2001; 11(1):25-32. doi: 10.1046/j.1365-263x.2001.00204.x [Crossref] [ Google Scholar]
- Bridgman CM, Ashby D, Holloway PJ. An investigation of the effects on children of tooth extraction under general anaesthesia in general dental practice. Br Dent J 1999; 186(5):245-7. doi: 10.1038/sj.bdj.4800076 [Crossref] [ Google Scholar]
- Atan S, Ashley P, Gilthorpe MS, Scheer B, Mason C, Roberts G. Morbidity following dental treatment of children under intubation general anaesthesia in a day-stay unit. Int J Paediatr Dent 2004; 14(1):9-16. doi: 10.1111/j.1365-263x.2004.00520.x [Crossref] [ Google Scholar]
- Kocataş Ersin N, Onçag O, Cogulu D, Ciçek S, Balcioglu ST, Cökmez B. Postoperative morbidities following dental care under day-stay general anesthesia in intellectually disabled children. J Oral Maxillofac Surg 2005; 63(12):1731-6. doi: 10.1016/j.joms.2005.08.021 [Crossref] [ Google Scholar]
- Patel RI, Hannallah RS. Anesthetic complications following pediatric ambulatory surgery: a 3-yr study. Anesthesiology 1988; 69(6):1009-12. doi: 10.1097/00000542-198812000-00044 [Crossref] [ Google Scholar]
- Coulthard P, Rolfe S, Mackie IC, Gazal G, Morton M, Jackson-Leech D. Intraoperative local anaesthesia for paediatric postoperative oral surgery pain--a randomized controlled trial. Int J Oral Maxillofac Surg 2006; 35(12):1114-9. doi: 10.1016/j.ijom.2006.07.007 [Crossref] [ Google Scholar]
- Haubek D, Fuglsang M, Poulsen S, Rølling I. Dental treatment of children referred to general anaesthesia--association with country of origin and medical status. Int J Paediatr Dent 2006; 16(4):239-46. doi: 10.1111/j.1365-263X.2006.00737.x [Crossref] [ Google Scholar]
- Mayeda C, Wilson S. Complications within the first 24 hours after dental rehabilitation under general anesthesia. Pediatr Dent 2009; 31(7):513-9. [ Google Scholar]
- Rao TD, Kumar MS. Analgesic efficacy of paracetamol vs ketorolac after dental extractions. Res J Pharm Technol 2018; 11(8):3375-9. doi: 10.5958/0974-360x.2018.00621.2 [Crossref] [ Google Scholar]
- Baley K, Michalov K, Kossick MA, McDowell M. Intravenous acetaminophen and intravenous ketorolac for management of pediatric surgical pain: a literature review. AANA J 2014; 82(1):53-64. [ Google Scholar]
- American Society of Anesthesiologists Task Force on Acute Pain Management. Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology. 2012;116(2): 248-73. doi: 10.1097/ALN.0b013e31823c1030.
- Hong JY, Kim WO, Koo BN, Cho JS, Suk EH, Kil HK. Fentanyl-sparing effect of acetaminophen as a mixture of fentanyl in intravenous parent-/nurse-controlled analgesia after pediatric ureteroneocystostomy. Anesthesiology 2010; 113(3):672-7. doi: 10.1097/ALN.0b013e3181e2c34b [Crossref] [ Google Scholar]
- Watts K, Balzer S, Drum M, Nusstein J, Reader A, Fowler S. Ibuprofen and acetaminophen versus intranasal ketorolac (Sprix) in an untreated endodontic pain model: a randomized, double-blind investigation. J Endod 2019; 45(2):94-8. doi: 10.1016/j.joen.2018.11.005 [Crossref] [ Google Scholar]
- Smith HS. Perioperative intravenous acetaminophen and NSAIDs. Pain Med 2011; 12(6):961-81. doi: 10.1111/j.1526-4637.2011.01141.x [Crossref] [ Google Scholar]
- Wong DL, Baker CM. Pain in children: comparison of assessment scales. Pediatr Nurs 1988; 14(1):9-17. [ Google Scholar]
- Tomlinson D, von Baeyer CL, Stinson JN, Sung L. A systematic review of faces scales for the self-report of pain intensity in children. Pediatrics 2010; 126(5):e1168-98. doi: 10.1542/peds.2010-1609 [Crossref] [ Google Scholar]
- Pocock SJ. Clinical Trials: A Practical Approach. John Wiley & Sons; 1983.
- Fitzmaurice GM, Laird NM, Ware JH. Applied Longitudinal Analysis. John Wiley & Sons; 2011. doi: 10.1002/9781119513469.
- Aghadavoudi O, Hajigholam Saryazdi H, Shafa A, Ramezani A. Comparison of pre-emptive effect of meloxicam and celecoxcib on post-operative analgesia: a double-blind, randomized clinical trial. Middle East J Anaesthesiol 2015; 23(3):289-94. [ Google Scholar]
- El Deeb A, El-Morsy GZ. Comparison of preemptive analgesic effect of intravenous ketorolac versus tramadol in pediatric inguinal herniotomy: a randomized double-blind study. Egypt J Anaesth 2011; 27(4):207-11. doi: 10.1016/j.egja.2011.07.005 [Crossref] [ Google Scholar]
- Morrison NA, Repka MX. Ketorolac versus acetaminophen or ibuprofen in controlling postoperative pain in patients with strabismus. Ophthalmology 1994; 101(5):915-8. doi: 10.1016/s0161-6420(94)31238-3 [Crossref] [ Google Scholar]
- Bean-Lijewski JD, Stinson JC. Acetaminophen or ketorolac for post myringotomy pain in children? A prospective, double-blinded comparison. Paediatr Anaesth 1997; 7(2):131-7. doi: 10.1046/j.1460-9592.1997.d01-47.x [Crossref] [ Google Scholar]
- Watcha MF, Ramirez-Ruiz M, White PF, Jones MB, Lagueruela RG, Terkonda RP. Perioperative effects of oral ketorolac and acetaminophen in children undergoing bilateral myringotomy. Can J Anaesth 1992; 39(7):649-54. doi: 10.1007/bf03008224 [Crossref] [ Google Scholar]
- Hajigholam Saryazdi H, Aghadavoudi O, Shafa A, Baghban-Nikoo M, Rezaei T. A comparative study of the analgesic effects of pethidine versus ketorolac and acetaminophen after lower abdominal and genital surgeries in children. J Isfahan Med Sch 2017; 34(412):1556-62. [ Google Scholar]
- Erkmen Almaz M, Akbay Oba A, Saroglu Sonmez I. Postoperative morbidity in pediatric patients following dental treatment under general anesthesia. Eur Oral Res 2019; 53(3):113-8. doi: 10.26650/eor.20190023 [Crossref] [ Google Scholar]
- Ghafournia M, Eshghi A, Mosleh H, Iranmanesh P. Complications after dental rehabilitation under general anesthesia in Isfahan during February to May 2016. Dent Res J (Isfahan) 2021; 18:53. [ Google Scholar]
- Deng XY, Zhang YH, Zou J, Zhang Q. [Investigation of postoperative complications in children after dental therapy under general anesthesia]. Hua Xi Kou Qiang Yi Xue Za Zhi 2020; 38(3):284-9. doi: 10.7518/hxkq.2020.03.010.[Chinese] [Crossref] [ Google Scholar]
- Keles S, Kocaturk O. Immediate postoperative pain and recovery time after pulpotomy performed under general anaesthesia in young children. Pain Res Manag 2017; 2017:9781501. doi: 10.1155/2017/9781501 [Crossref] [ Google Scholar]
- Chen XX, Jiang X, Zhong J, Zhang HM, Huang Q, Xia B. [Postoperative complications following dental rehabilitation under general anesthesia in children]. Zhonghua Kou Qiang Yi Xue Za Zhi 2017; 52(11):661-6. doi: 10.3760/cma.j.issn.1002-0098.2017.11.003 [Crossref] [ Google Scholar]
- Gharavi M, Soltani G. Evaluation of general anesthesia in pediatric dental procedures. J Mashhad Dent Sch 2008; 32(1):41-6. doi: 10.22038/jmds.2008.1338 [Crossref] [ Google Scholar]
- Kharouba J, Ratson T, Somri M, Blumer S. Preemptive analgesia by paracetamol, ibuprofen or placebo in pediatric dental care: a randomized controlled study. J Clin Pediatr Dent 2019; 43(1):51-5. doi: 10.17796/1053-4625-43.1.10 [Crossref] [ Google Scholar]
- Alhashemi JA, Daghistani MF. Effect of intraoperative intravenous acetaminophen vs intramuscular meperidine on pain and discharge time after paediatric dental restoration. Eur J Anaesthesiol 2007; 24(2):128-33. doi: 10.1017/s0265021506001232 [Crossref] [ Google Scholar]
- Só GB, Silva IA, Weissheimer T, Lenzi TL, Só MV, da Rosa RA. Do NSAIDs used prior to standard inferior alveolar nerve blocks improve the analgesia of mandibular molars with irreversible pulpitis? An umbrella review. Clin Oral Investig 2023; 27(5):1885-97. doi: 10.1007/s00784-023-04979-3 [Crossref] [ Google Scholar]
- Hasheminia D, Faghihian R, Mardani F. Effect of submucosal injection of ketorolac versus dexamethasone on postoperative pain after third molar surgery: a randomized clinical trial. Ain Shams J Anesthesiol 2021; 13(1):1-7. doi: 10.1186/s42077-021-00177-z [Crossref] [ Google Scholar]