Avicenna J Dent Res. 17(3):172-177.
doi: 10.34172/ajdr.2185
Original Article
Comparison of Marginal Ridge Fracture Resistance of Restored Primary Molar Teeth Using Flowable Bulk-Fill and Smart Monochromatic Composites: An In-Vitro Study
Fahimeh Daneshyar Conceptualization, Funding acquisition, Investigation, Methodology, Supervision, 1 
Mandana Karimi Investigation, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing, 2
Sahar Yaghoutiazar Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Software, Validation, Visualization, Writing – review & editing, 3, *
Author information:
1Department of Pediatric Dentistry, School of Dentistry, Hamadan University of Medical Sciences, Hamadan, Iran
2Department of Restorative Dentistry, Faculty of Dentistry, Alborz University of Medical Sciences, Alborz, Iran
3Department of Pediatric Dentistry, Faculty of Dentistry, Hamadan University of Medical Sciences, Hamadan, Iran
Abstract
Background: The durability of marginal ridges has a significant effect on maintaining the structural integrity and functional performance of primary molar teeth. This study evaluated and compared marginal ridge fracture resistance of restored primary molars using two innovative restorative materials, namely, flowable bulk-fill and smart monochromatic composites.
Methods: In this experimental study, 38 primary molar teeth were randomly divided into two binary groups. After the removal of caries and undermined enamel, conventional amalgam class II (≈ 3 mm×3 mm×4 mm) was prepared in one proximal surface. Flowable bulk fill universal composite (Palfique® Bulk Flow, Tokuyama, Japan) was applied in one group, and smart monochromatic universal composite (Omnichroma, Tokuyama, Japan) was placed and cured in another group. All samples were subjected to 5000 thermal cycles ranging from 5 °C to 55 °C. Next, the teeth were mounted with self-curing acrylic resin 1 mm above the CEJ. The fracture resistance of the teeth was measured using a universal testing machine with a maximum force of 1000 Newton. The intact marginal ridges of the opposite sides were also tested for resistance to failure as control groups. The force at which the marginal ridge was broken indicated the resistance to failure in Newton units. The data were analyzed using the Kolmogorov-Smirnov test.
Results: The Kolmogorov-Smirnov test results revealed that fracture resistance measurements in both groups had a normal distribution (P>0.05). In addition, the comparison of the average resistance in the two composite groups showed that the resistance in the Omnichroma group was significantly higher than the flowable bulk-fill group (P<0.001).
Conclusion: Based on the findings, smart monochromatic (Omnichroma) composites have higher marginal fracture resistance than flowable bulk-fill (Bulk-Flow U) composites in the restoration of posterior primary teeth.
Keywords: Fracture strength, Composite resins, Primary tooth
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Daneshyar F, Karimi M, Yaghoutiazar S. Comparison of marginal ridge fracture resistance of restored primary molar teeth using flowable bulk-fill and smart monochromatic composites: an in-vitro study. Avicenna J Dent Res. 2025;17(3):172-177. doi:10.34172/ajdr.2185
Background
Dental caries is a chronic infectious disease and the most common dental condition in childhood (1). This condition develops when acids produced by oral bacteria, such as Streptococcus mutans, metabolize fermentable carbohydrates present in saliva, leading to enamel demineralization and tooth structure destruction (2). While bacterial factors play a central role, other factors, including host susceptibility and diet, are also important in the development of caries (3). Early childhood caries is a particularly common form of the disease in children, characterized by its rapid progression (4). These lesions can result in significant functional and psychological challenges, underscoring the importance of maintaining primary teeth in the oral cavity until their natural exfoliation (4).
Several treatment options exist for carious primary teeth, including stainless steel crowns, amalgam fillings, and composite restorations (5,6). The introduction of resin-based composites has significantly advanced pediatric restorative dentistry by offering improved esthetics and favorable mechanical properties (7-9). However, certain challenges remain, such as achieving proper isolation, managing patient cooperation, and minimizing chair time, which are particularly critical in pediatric patients (7,8). To overcome these limitations, newer materials, including flowable bulk-fill and smart monochromatic composites, have been developed, aiming to simplify the restorative process while maintaining optimal clinical outcomes (10,11).
Bulk-fill composites are classified into flowable (low-viscosity) and sculptable (high-viscosity) types (11). Flowable bulk-fill composites offer excellent adaptation to cavity walls and margins. They are formulated to allow for greater curing depths (4–5 mm) and lower polymerization shrinkage, which can streamline the restorative process and reduce chair time (12). Several studies have evaluated the fracture resistance of primary molars restored with incremental versus bulk-fill composite techniques. These studies demonstrated that bulk-fill composites generally exhibit higher fracture resistance compared to the incremental technique, indicating a potential advantage in pediatric restorations (11-13). However, other studies have reported no significant difference in fracture resistance between bulk-fill and conventional composite restorations (14,15).
Regarding monochromatic composites, recent studies have emphasized the unique ability of materials such as Omnichroma (Tokuyama, Japan) to seamlessly blend with surrounding tooth structures, utilizing structural color technology and thereby eliminating the need for shade selection (11). This material incorporates a distinctive feature known as “smart chromatic technology,” which simplifies the restorative process by allowing a single shade to adapt across a wide range of tooth colors, reducing the potential confusion associated with multiple shade options for clinicians (16,17). Most of the existing studies on Omnichroma have focused on permanent teeth and are primarily limited to anterior restorations, leaving a gap in the literature regarding its performance in posterior primary teeth, especially in terms of marginal fracture resistance (18-20).
These types of modern dental composites can be a suitable alternative to conventional composites, especially in pediatric dentistry, due to their simplified application and promising mechanical properties. Despite their advantages, the available literature on flowable bulk-fill composites (e.g., Palfique® Bulk Flow, Tokuyama, Japan) and smart monochromatic composites (e.g., OMNICHROMA, Tokuyama, Japan) remains limited and, in some cases, presents contradictory results regarding their mechanical performance, particularly in primary teeth (10-20). Considering that maintaining marginal integrity is critical for the longevity of restorations, especially in high-stress areas (e.g., marginal ridges of posterior primary teeth), this study aims to compare the marginal ridge fracture resistance of Bulk-Flow U (Tokuyama, Japan) and Omnichroma (Tokuyama, Japan) when used for restoring class II cavities in primary molars. The findings of this study may help guide material selection in pediatric restorative dentistry.
Materials and Methods
In this experimental study, two types of composite resins were investigated, including flowable bulk-fill (Palfique® Bulk Flow, Tokuyama, Japan) and smart monochromatic universal (Omnichroma, Tokuyama, Japan) composites at the Dental School of Hamedan University of Medical Sciences in 2023. According to the study by Yeolekar et al, the sample size was estimated to be 19 in each group; therefore, the total sample size was 38 (21). The study protocol was approved by the Ethics Committee of the Dental School at Hamedan University of Medical Sciences (IR.UMSHA.REC.1402.291).
Inclusion and Exclusion Criteria
The crowns of the posterior primary teeth that had at least one intact marginal ridge were included in this study. In addition, the teeth had no history of pulp therapy. These teeth had been extracted from patients without medical or systemic problems within the past 6 months. On the other hand, any posterior primary tooth with restoration, crack, or caries developed to the cementoenamel junction, severe root resorption, and endodontic treatment was excluded from the study (21).
Sample Preparation
First, the surface debris of the teeth was removed using a prophylaxis brush and pumice paste without fluoride. After extraction, the teeth were placed in chloramine T solution for one week and then kept in distilled water solution until the start of the experiment. After removing caries and undermined enamel, conventional amalgam class II (≈ 3 mm × 3 mm × 4 mm) was prepared in one proximal surface (mesial or distal) of all teeth using a flat-ended cylindrical diamond bur (No. 835. FG.012, Jota, Switzerland) in a high-speed handpiece with air-water spray. All preparations were prepared to the same size as much as possible by the same operator and checked with a periodontal probe. The teeth that did not meet this conventional amalgam class II preparation were eliminated and replaced. Buccal and lingual walls of the cavity were shaped parallel to each other, and the faciolingual dimensions of the box-shaped preparations were 3 mm. The depth of the box gingivally from the marginal ridge was 4 mm, and the axial depth of the gingival floor was 3 mm. The prepared margins lacked any bevel. The bur was replaced after preparing every 5 cavities (21-23).
Restorative Procedure
The enamel and dentin surfaces of the teeth in the coronal area were etched using 35% phosphoric acid (FGM, Brazil) for 20 seconds and 10 seconds, respectively. Next, the etched surfaces were washed for 5–10 seconds and dried slowly with air spray. The two-step etch-and-rinse dental adhesive (Scotchbond, 3M ESPE, St. Paul, MN, USA) was placed on the etched surfaces according to the manufacturer’s instructions and then cured for 10 seconds with the LED light curing unit by a 1500 mW/cm2 curing light output (Woodpecker ILED plus, China).
Subsequently, the teeth were randomly divided into two groups of 19. In one group, the flowable bulk-fill universal composite (Palfique® Bulk Flow, Tokuyama, Japan) was applied as a single layer of 4 mm and cured with the LED light curing unit by a 1500 mW/cm2 curing light output (Woodpecker ILED plus, China) according to the manufacturer’s instructions for 40 seconds. In another group, the smart monochromatic universal composite (Omnichroma, Tokuyama, Japan) was placed using the oblique incremental technique, and each increment was cured with the same LED light curing unit for 40 seconds.
The operator finished all restorations using a fine diamond bur (No. 862. FG.012, Jota, Switzerland) and subsequently polished with aluminum oxide discs (Sof-Lex, Prop On, 3M ESPE, USA) (24,25).
Evaluation of Fracture Resistance
All samples were placed in distilled water at 37 °C for 24 hours and then subjected to 5000 thermal cycles ranging from 5 °C to 55 °C. The dwell time and the transfer time were 20 seconds and 10 seconds, respectively. After preparation, the samples were stored in distilled water in an incubator at 37 °C for one week.
Afterward, the teeth were mounted with self-curing acrylic resin 1 mm above the CEJ with equal shapes and sizes. The fracture resistance of the teeth was measured using a universal testing machine (Zwick Roell, Ulm, Germany) with a maximum force of 1000 Newtons. The force was applied mesiodistally at a speed of 1 mm/min in the one-way medial region of the marginal ridge of the teeth. The force was slowly increased until failure occurred. The intact opposite-side marginal ridges were also subjected to the fracture resistance test as control groups. The force at the time of failure was calculated in Newtons and indicated fracture resistance in Newtons (21-23).
Statistical Analysis
The obtained data were analyzed by SPSS software (version 22) and then compared regarding fracture resistance using a paired t-test. The P value < 0.05 was considered statistically significant.
Results
In this study, the results of the Kolmogorov-Smirnov test showed that the fracture resistance measurements had a normal distribution in both groups (P > 0.05).
The average ( ± standard deviation) fracture resistance of the bulk flow composite group and its control group was 198.67 N ( ± 27.68) and 543.98 N ( ± 136.70), respectively. The findings demonstrated that there was a significant difference in the average fracture resistance of bulk flow composite U compared to the control group on the opposite side (Table 1, P < 0.001). In other words, the average fracture resistance of healthy samples was more than 2.5 times (2.74) higher than Bulk-Flow U samples.
Table 1.
Means, Standard Deviations, and Paired Samples T-Test Data of Flexural Strength of the Bulk-Flow U and its Control (Healthy) Groups
|
Paired Samples Statisticsa
|
|
|
|
|
Mean
|
N
|
SD
|
Standard Error of the Mean
|
Paired T-Test
|
| Pair 1 |
Bulk-Flow U composite |
198.67 |
19 |
27.68 |
6.35 |
T = -9.74, df = 18, P< 0.001 |
| Healthy group |
543.98 |
19 |
136.70 |
31.36 |
Note. N: Number; SD: Standard deviation; Std. error: Standard error; df: Degree of freedom.
Moreover, the average ( ± standard deviation) fracture resistance of the Omnichroma composite group and its control group was 276.63 N ( ± 59.08) and 508.45 N ( ± 146.03), respectively. Based on the findings, the average fracture resistance of the Omnichroma composite was significantly higher than the control group on the opposite side (Table 2, P< 0.001).
Table 2.
Means, Standard Deviations, and Paired Samples T-Test Data of Flexural Strength of the Omnichroma and its Control (Healthy) Groups
|
Paired Samples Statisticsa
|
|
|
|
|
Mean
|
N
|
SD
|
Standard Error of the Mean
|
Paired T-Test
|
Pair 1 |
Omnichroma composite |
276.63 |
19 |
59.08 |
13.55 |
T = -6.553, df = 18, P < 0.001 |
| Healthy group |
508.45 |
19 |
146.03 |
33.50 |
Note. N: Number; SD: Standard deviation; Std. error: Standard error; df: Degree of freedom.
Figure 1 displays the average fracture resistance of the examined samples for each of the composite groups compared to the adjacent healthy samples (control groups).
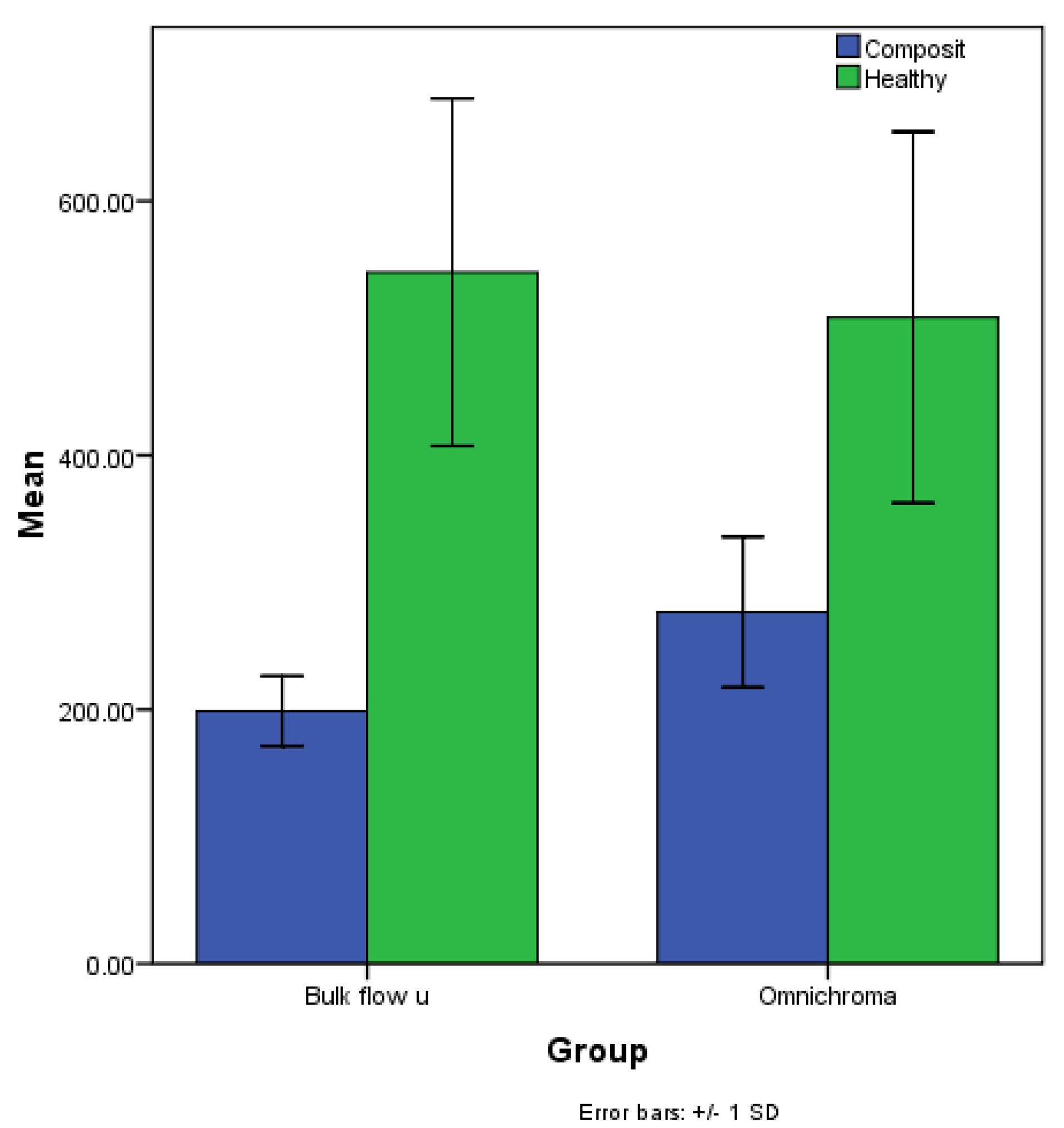
Figure 1.
The Average Fracture Resistance of the Samples for Each of the Composite Groups (Blue Ones) Compared to the Adjacent Healthy Samples (Green Ones)
.
The Average Fracture Resistance of the Samples for Each of the Composite Groups (Blue Ones) Compared to the Adjacent Healthy Samples (Green Ones)
The data comparison between composite groups indicated that the average fracture resistance in the Bulk-Flow U group was noticeably lower than that of the Omnichroma group (Table 3, P< 0.001).
Table 3.
Means, Standard Deviations, and Independent T-Test Data of Flexural Strength of the Bulk-Flow U and Omnichroma Groups
|
Group Statistics
|
|
|
|
Group
|
N
|
Mean
|
SD
|
Standard Error of the Mean
|
Independent T-Test
|
| Composite |
Bulk-Flow U |
19 |
198.67 |
27.68 |
6.35 |
T = -5.209, df = 25.54, P < 0.001 |
| Omnichroma |
19 |
276.63 |
59.08 |
13.55 |
Note. N: Number; SD: Standard deviation; Std. error: Standard error; df: Degree of freedom.
Discussion
The present study assessed and compared the fracture resistance of two different new dental composites in primary molar teeth. The null hypothesis was that no significant difference would be found in the fracture resistance of primary molar teeth restored with different composite groups. The results confirmed that the fracture resistance was significantly higher in control groups (intact marginal ridges). It was also significantly higher in the smart monochrome (Omnichroma) group compared to the bulkfill (Bulkfill-Flow U) group.
The success and longevity of restorations in primary teeth are largely determined by the physical and mechanical properties of restorative materials, including fracture strength, hardness, and wear resistance (8). Beyond ensuring adequate durability, the increased risk of trauma and crown fractures in children further underscores the importance of achieving sufficient fracture resistance in the restorations of primary teeth (8,26).
Bulk-fill and conventional composites share a similar base composition; however, modifications in monomer chemistry, filler size, and filler content have been introduced, enabling bulk-fill composites to be placed in increments of up to 4 mm (10). Nevertheless, these alterations can potentially influence the physical and mechanical properties of the material, including its toughness and fracture strength (12).
Bulk-fill composites exhibit lower post-gel shrinkage compared to conventional composites (10,12). Additionally, the use of bulk-fill techniques has been associated with reduced cusp deflection and enhanced fracture resistance. These advantages suggest that bulk-fill composites may be a preferable option for clinicians, as they can simplify the restorative process while minimizing the adverse effects commonly observed in traditional techniques (13).
In an in-vitro study by Mosharrafian et al, the fracture resistance of bulk-fill and conventional composites was evaluated in the restoration of severely damaged anterior primary teeth (14). Their results demonstrated no statistically significant difference among the three tested groups (14). Similarly, another study reported no difference in fracture resistance between restorations using bulk-fill flowable and conventional resin composites (27). Conversely, multiple studies indicated that paste bulk-fill composites exhibit superior marginal ridge fracture resistance compared to the other types of composites (21,28-30), with one study even suggesting that the fracture resistance of paste bulk-fill composites was comparable to that of the intact tooth structure (21). Although these findings are not fully aligned with the results of our study, it is important to note that most previous studies compared bulk-fill composites with conventional composites, whereas our study focused on comparing bulk-fill composites with a smart monochromatic composite.
A recent in-vitro study evaluated the fracture resistance of primary anterior teeth restored with different post and composite restorations (31). The reinforced bulk fill composite with short fibers had enhanced fracture resistance and increased reparability in case of restoration fracture (31). This technique was recommended for the restoration of primary teeth since it is simple and saves time (31). However, due to the use of posts in this study, its results may not be generalizable to studies that did not use posts because the use of the posts will increase fracture resistance (32).
Systematic reviews and meta-analyses have demonstrated that Omnichroma (smart monochromatic) composite resins yield promising outcomes in direct dental restorations. These materials are increasingly favored by pediatric dentists due to advantages such as ease of handling, good wear resistance, excellent polishability, high fracture resistance, effective color matching, and reduced chair time (11,16). Kikuti et al reported that resin composites with higher flexural strength and elastic modulus exhibited greater fracture resistance when used with an etch-and-rinse adhesive system (33), which is consistent with the findings of our study. In our observations, the Omnichroma composite showed a higher elastic modulus and fracture resistance compared to the Bulk-Flow U composite.
Variations observed across studies can be attributed to intrinsic composite properties, such as photoinitiator systems, resin matrix chemistry, and filler types, as well as extrinsic factors. These factors include restorative techniques (increment thickness, placement methods, and application temperature), light activation parameters (curing mode and exposure duration), characteristics of the curing unit (light intensity, wavelength, heat emission, and diameter), thermocycling protocols, and the location of load application. Another critical factor is the difference between flowable and paste-type bulk-fill composites used in these studies. Most studies indicate that paste bulk-fill composites possess mechanical properties comparable or superior to conventional composites, though they are generally outperformed by fiber-reinforced composites (28-31,34-36). Flowable bulk-fill composites typically exhibit lower fracture resistance due to their reduced filler content but demonstrate better marginal adaptation (35). Consequently, based on current evidence and consistent with the findings of this study, flowable bulk-fill composites are recommended for narrow cavities deeper than 4 mm, particularly when enhanced adaptation in less accessible areas is required (13). It should be noted that “full-body” bulk-fill composites are preferred for larger cavities demanding higher filler loads (10,12).
Considering the inherent limitations of current in-vitro investigations, robust clinical trials are imperative to comprehensively evaluate the performance and longevity of flowable bulk-fill and smart monochromatic composites under clinical conditions. Furthermore, expanding comparative analyses to include a wider spectrum of composite materials will enhance the reliability and generalizability of the findings.
Conclusion
Within the limitations of this in-vitro study, the smart monochromatic composite (Omnichroma) demonstrated higher marginal fracture resistance than the flowable bulk-fill composite (Bulk-Flow U) in restoring posterior primary teeth. This suggests that Omnichroma may provide enhanced resistance to marginal ridge fractures and potentially improve the clinical longevity of restorations in pediatric dentistry. However, given the limitations of an in-vitro setup, further in-vivo studies are required to validate these findings under functional and long-term clinical conditions.
Competing Interests
The authors declare that there is no conflict of interests.
Ethical Approval
This study was approved by the Ethics Committee of Hamedan University of Medical Sciences, the School of Dentistry (IR.UMSHA.REC.1402.291).
Funding
This work was supported as a university research project funded by Hamedan University of Medical Sciences under grant number 140204273456.
References
- Kazeminia M, Abdi A, Shohaimi S, Jalali R, Vaisi-Raygani A, Salari N. Dental caries in primary and permanent teeth in children’s worldwide, 1995 to 2019: a systematic review and meta-analysis. Head Face Med 2020; 16(1):22. doi: 10.1186/s13005-020-00237-z [Crossref] [ Google Scholar]
- Spatafora G, Li Y, He X, Cowan A, Tanner ACR. The evolving microbiome of dental caries. Microorganisms 2024; 12(1):121. doi: 10.3390/microorganisms12010121 [Crossref] [ Google Scholar]
- Giacaman RA, Fernández CE, Muñoz-Sandoval C, León S, García-Manríquez N, Echeverría C. Understanding dental caries as a non-communicable and behavioral disease: management implications. Front Oral Health 2022; 3:764479. doi: 10.3389/froh.2022.764479 [Crossref] [ Google Scholar]
- Nadeeshani H, Kudagammana ST, Herath C, Jayasinghe R, Liyanage R. Early childhood caries and nutritional status of children: a review. Food Nutr Bull 2023; 44(4):249-64. doi: 10.1177/03795721231209358 [Crossref] [ Google Scholar]
- Jenkins N. Jenkins NMaterials for paediatric dentistryPart 1: background to the treatment of carious primary teeth. Dent Update 2015; 42(10):905-10. doi: 10.12968/denu.2015.42.10.905 [Crossref] [ Google Scholar]
- Keels MA. Personalized dental caries management in children. Dent Clin North Am 2019; 63(4):621-9. doi: 10.1016/j.cden.2019.06.002 [Crossref] [ Google Scholar]
- Amend S, Seremidi K, Kloukos D, Bekes K, Frankenberger R, Gizani S. Clinical effectiveness of restorative materials for the restoration of carious primary teeth: an umbrella review. J Clin Med 2022; 11(12):3490. doi: 10.3390/jcm11123490 [Crossref] [ Google Scholar]
- Chisini LA, Collares K, Cademartori MG, de Oliveira LJ, Conde MC, Demarco FF. Restorations in primary teeth: a systematic review on survival and reasons for failures. Int J Paediatr Dent 2018; 28(2):123-39. doi: 10.1111/ipd.12346 [Crossref] [ Google Scholar]
- Karimi M, Ataee E, Omrani LR, Abbasi M, Ahmadi E. Influence of different light-activated bleaching gels on pulp chamber temperature: an in vitro study. Avicenna J Dent Res 2024; 16(4):225-31. doi: 10.34172/ajdr.1743 [Crossref] [ Google Scholar]
- Chesterman J, Jowett A, Gallacher A, Nixon P. Bulk-fill resin-based composite restorative materials: a review. Br Dent J 2017; 222(5):337-44. doi: 10.1038/sj.bdj.2017.214 [Crossref] [ Google Scholar]
- AlHamdan EM, Bashiri A, Alnashmi F, Al-Saleh S, Al-shahrani K, Al-shahrani S, Alsharani A, Alzahrani KM, Alqarawi FK, Vohra F. Evaluation of Smart Chromatic Technology for a Single-Shade Dental Polymer Resin: An In Vitro Study. Applied Sciences 2021; 11(21):10108. doi: 10.3390/app112110108 [Crossref] [ Google Scholar]
- Van Ende A, De Munck J, Lise DP, Van Meerbeek B. Bulk-fill composites: a review of the current literature. J Adhes Dent 2017; 19(2):95-109. doi: 10.3290/j.jad.a38141 [Crossref] [ Google Scholar]
- Parra Gatica E, Duran Ojeda G, Wendler M. Contemporary flowable bulk-fill resin-based composites: a systematic review. Biomater Investig Dent 2023; 10(1):8-19. doi: 10.1080/26415275.2023.2175685 [Crossref] [ Google Scholar]
- Mosharrafian S, Shafizadeh M, Sharifi Z. Fracture resistance of a bulk-fill and a conventional composite and the combination of both for coronal restoration of severely damaged primary anterior teeth. Front Dent 2019; 16(1):69-77. doi: 10.18502/fid.v16i1.1112 [Crossref] [ Google Scholar]
- Al-Ibraheemi ZA, Abdullah HA, Jawad NA, Haider J. Assessing fracture resistance of restored premolars with novel composite materials: an in vitro study. Int J Dent 2021; 2021:5512708. doi: 10.1155/2021/5512708 [Crossref] [ Google Scholar]
- Eliezer R, Devendra C, Ravi N, Tangutoori T, Yesh S. Omnichroma: one composite to rule them all. SSRG Int J Med Sci 2020; 7(6):6-8. [ Google Scholar]
- Yamaguchi S, Karaer O, Lee C, Sakai T, Imazato S. Color matching ability of resin composites incorporating supra-nano spherical filler producing structural color. Dent Mater 2021; 37(5):e269-75. doi: 10.1016/j.dental.2021.01.023 [Crossref] [ Google Scholar]
- de Fátima Soares Garcia B, Lachi EL, Ferraresso LF, Besegato JF, Hoeppner MG. Restoration of fractured anterior tooth with monochrome composite resin in pediatric dental patient. Rev Odontoped Latinoam 2024; 14:e243663. doi: 10.47990/nf9dgw12 [Crossref] [ Google Scholar]
- Ahmed MA, Jouhar R, Khurshid Z. Smart monochromatic composite: a literature review. Int J Dent 2022; 2022:2445394. doi: 10.1155/2022/2445394 [Crossref] [ Google Scholar]
- Hasanain FA. Flexural strength and depth of cure of single shade dental composites. J Pharm Res Int 2021; 33(49A):110-8. doi: 10.9734/jpri/2021/v33i49A33310 [Crossref] [ Google Scholar]
- Yeolekar TS, Chowdhary NR, Mukunda KS, Kiran NK. Evaluation of microleakage and marginal ridge fracture resistance of primary molars restored with three restorative materials: a comparative in vitro study. Int J Clin Pediatr Dent 2015; 8(2):108-13. doi: 10.5005/jp-journals-10005-1294 [Crossref] [ Google Scholar]
- Wafaie RA, Ahmed B, Mahmoud SH. Fracture resistance of molars with class II MOD cavities restored with bulk-fill, no-cap flowable bulk-fill, and conventional resin composite restorative systems after 6-months water storage. BMC Oral Health 2025; 25(1):741. doi: 10.1186/s12903-025-05951-1 [Crossref] [ Google Scholar]
- Al-Thobity AM, Altaher A, Alharbi A, Elnour M. An in vitro comparison of the fracture resistance of standard and modified mesio-occluso-distal cavity designs restored with resin composite restoration. Int J Health Sci (Qassim) 2018; 12(2):26-30. [ Google Scholar]
- Ghasemi A, Mohammadzadeh A, Molaei M, Sheikh-Al-Eslamian SM, Karimi M. Effect of wet and dry finishing and polishing technique on microhardness and flexural strength of nanocomposite resins. Int J Dent 2023; 2023:2182094. doi: 10.1155/2023/2182094 [Crossref] [ Google Scholar]
- Saati K, Valizadeh S, Rahmaniparast A, Karimi M. In vitro effects of Sof-Lex, Eve, and Astropol polishing systems on composite resin surface roughness after aging. Front Dent 2024; 21:35. doi: 10.18502/fid.v21i35.16473 [Crossref] [ Google Scholar]
- Yengopal V, Harnekar SY, Patel N, Siegfried N. WITHDRAWN: dental fillings for the treatment of caries in the primary dentition. Cochrane Database Syst Rev 2016; 10(10):CD004483. doi: 10.1002/14651858.CD004483.pub3 [Crossref] [ Google Scholar]
- Toz T, Tuncer S, Öztürk Bozkurt F, Kara Tuncer A, Gözükara Bağ H. The effect of bulk-fill flowable composites on the fracture resistance and cuspal deflection of endodontically treated premolars. J Adhes Sci Technol 2015; 29(15):1581-92. doi: 10.1080/01694243.2015.1037381 [Crossref] [ Google Scholar]
- Ilie N, Keßler A, Durner J. Influence of various irradiation processes on the mechanical properties and polymerisation kinetics of bulk-fill resin-based composites. J Dent 2013; 41(8):695-702. doi: 10.1016/j.jdent.2013.05.008 [Crossref] [ Google Scholar]
- Kim RJ, Kim YJ, Choi NS, Lee IB. Polymerization shrinkage, modulus, and shrinkage stress related to tooth-restoration interfacial debonding in bulk-fill composites. J Dent 2015; 43(4):430-9. doi: 10.1016/j.jdent.2015.02.002 [Crossref] [ Google Scholar]
- Akman H, Tosun G. Clinical evaluation of bulk-fill resins and glass ionomer restorative materials: a 1-year follow-up randomized clinical trial in children. Niger J Clin Pract 2020; 23(4):489-97. doi: 10.4103/njcp.njcp_519_19 [Crossref] [ Google Scholar]
- Alamdari Mahd M, Moeiny P, Heshmat H, Askarizadeh N. In vitro comparison of fracture resistance of severely damaged primary anterior teeth restored with different post and core systems. Int J Dent 2023; 2023:2895892. doi: 10.1155/2023/2895892 [Crossref] [ Google Scholar]
- Saad KB, Bakry SI, AboElhassan RG. Fracture resistance of endodontically treated teeth, restored with two post-core systems in different post space diameters (in vitro study). BMC Oral Health 2023; 23(1):992. doi: 10.1186/s12903-023-03730-4 [Crossref] [ Google Scholar]
- Kikuti WY, Chaves FO, Di Hipólito V, Rodrigues FP, D’Alpino PH. Fracture resistance of teeth restored with different resin-based restorative systems. Braz Oral Res 2012; 26(3):275-81. doi: 10.1590/s1806-83242012005000004 [Crossref] [ Google Scholar]
- Ibrahim MS, AlKhalefah AS, Alsaghirat AA, Alburayh RA, Alabdullah NA. Comparison between different bulk-fill and incremental composite materials used for class II restorations in primary and permanent teeth: in vitro assessments. Materials (Basel) 2023; 16(20):6674. doi: 10.3390/ma16206674 [Crossref] [ Google Scholar]
- Gindri LD, Cassol IP, Fröhlich TT, Rocha RO. One-year clinical evaluation of class II bulk-fill restorations in primary molars: a randomized clinical trial. Braz Dent J 2022; 33(6):110-20. doi: 10.1590/0103-6440202205069 [Crossref] [ Google Scholar]
- Rosatto CM, Bicalho AA, Veríssimo C, Bragança GF, Rodrigues MP, Tantbirojn D. Mechanical properties, shrinkage stress, cuspal strain and fracture resistance of molars restored with bulk-fill composites and incremental filling technique. J Dent 2015; 43(12):1519-28. doi: 10.1016/j.jdent.2015.09.007 [Crossref] [ Google Scholar]