Avicenna J Dent Res. 17(2):109-117.
doi: 10.34172/ajdr.2165
Original Article
How Common Are the Anatomical Anomalies of Mandibular Molars in an Iranian Subpopulation? A Cone-Beam Computed Tomography Assessment
Shamsodin Heydari Investigation, Software, Writing – review & editing, 1 
Behnam Bolhari Conceptualization, Investigation, Methodology, Supervision, 1
Foozie Zahedi Data curation, Project administration, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing, 2, *
Shima Younespour Data curation, Formal analysis, Methodology, 3
Author information:
1Department of Endodontics, School of Dentistry, Tehran University of Medical Sciences, Tehran, Iran
2Radiology Department, School of Dentistry, Dental Research Center, Hamadan University of Medical Sciences, Hamadan, Iran
3Dental Research Center, Dentistry Research Institute, Tehran University of Medical Sciences, Tehran, Iran
Abstract
Background: Information about root canal anatomical variations is important for successful root canal treatment. This study assessed the frequency of common anomalies of permanent mandibular first and second molars using cone-beam computed tomography (CBCT).
Methods: In this cross-sectional study, 505 CBCT scans were evaluated by an oral radiologist and an endodontist to determine the presence/absence of the mid-mesial canal, the C-shaped canal configuration and its type, the third root and its type, taurodontism and its percentage, and dilaceration and its degree. To assess intra- and inter-observer agreements, all CBCT scans were evaluated twice at a one-week interval by both observers. The data were analyzed using the kappa coefficient and univariate logistic regression.
Results: The kappa values showed acceptable inter-observer (0.780) and intra-observer (0.983) agreements. Of all, 21 teeth (4.17%) had a mid-mesial canal, 20 teeth (3.96%) had a third root, and 38 teeth (7.52%) had a C-shaped canal. The frequency of the third root (P=0.01) and C-shaped canal (P<0.000) in mandibular second molars was significantly higher than that in mandibular first molars (P<0.000). Taurodontism was detected in 6 teeth (1.19%), while root dilaceration was present in 162 teeth (34.23%). Age and gender had no significant association with the presence of a mid-mesial canal, third root, C-shaped canal, or dilaceration (P>0.05).
Conclusion: Mandibular first and second molars were not significantly different in the frequency of mid-mesial canal, taurodontism, and dilaceration. Considering the relatively high prevalence of dilaceration and C-shaped canals in the study population, these anatomical variations should be taken into account in root canal treatment.
Keywords: Anatomy, Cone-beam computed tomography, Taurodontism, Tooth root
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Heydari S, Bolhari B, Zahedi F, Younespour S. How Common Are the Anatomical Anomalies of Mandibular Molars in an Iranian Subpopulation? A Cone-Beam Computed Tomography Assessment. Avicenna J Dent Res. 2025;17(2):109-117. doi:10.34172/ajdr.2165
Background
Precise knowledge about the root canals is essential for a successful endodontic treatment. The most common morphological forms of the root canals have been well investigated in the literature. However, some anatomical variations are more important, and dental clinicians should be well aware of the possible presence of such complexities (1).
The mid-mesial canal is an anatomical variation observed in mandibular molars. It is located between the mesiobuccal and mesiolingual canals and has a variable prevalence rate in the literature (2-5).
Mandibular molar root canals show complex anatomical variations, such as C-shaped canals. This unique morphology manifests as the presence of one to three canals that are mainly related to ribbon-like or fan-shaped communication paths. This characteristic makes their complete debridement, shaping, and obturation more challenging. In addition, molars with C-shaped canals are more susceptible to iatrogenic errors, such as strip perforation, due to the thin root dentin and external root canal wall (6). Some previous studies evaluated the effect of race and ethnicity on the C-shaped root canal configuration (7,8). The East Asian population (29%–45%) has a much higher prevalence of C-shaped mandibular molars than the North American, African, West Asian, and European populations (7,9).
The external anatomy of mandibular molar teeth usually includes the presence of two roots with well-defined borders in most cases. One exception is the presence of an additional distolingual root known as the radix entomolaris. Another less common variation is the presence of an additional mesiobuccal root referred to as the radix paramolaris. It has been confirmed that the presence of a third root in mandibular first molars has a close association with race (10). In general, this anatomical variation has a high prevalence in specific populations, including Mongols, Native American Indians, Eskimos, and Chinese populations, such that it is considered a normal finding in these populations (11,12).
Taurodontism is defined as the abnormal enlargement of the pulp chamber characterized by apical displacement of the furcation area. This anomaly is normally detected by radiography rather than clinical examination. The percentage of taurodontism on three-dimensional (3D) radiographs is calculated according to the taurodontism index and has three main classes, namely, hypo-taurodontism, meso-taurodontism, and hyper-taurodontism (13).
Dilaceration occurs by the angulation of each part of the tooth length, which may include the crown, cementoenamel junction, root length, or only the root apex. This deformity is caused by the ectopic development of a tooth germ. Nonetheless, trauma has also been suggested as a possible cause, especially in the anterior region (14). Radiography is the only method for the detection of dilaceration. Older studies typically used 2D radiographic modalities, such as intraoral radiography and panoramic radiography, to report the prevalence of dilaceration, which are usually inefficient in the demonstration of dilaceration in the third dimension (15). Currently, cone-beam computed tomography (CBCT) is the preferred and relatively routine imaging modality for endodontic assessments. This modality has overcome the low accuracy of 2D radiographic modalities and can accurately reveal the details of the root canal system (16).
Previous studies only assessed one or two anomalies, and, to the best of our knowledge, no study has simultaneously evaluated different types of anomalies and their association with demographic factors, such as age and gender, in an Iranian population. Thus, this study aims to assess the frequency of five common anomalies in permanent mandibular first and second molars, including the presence of mid-mesial canal, C-shaped canal configuration and its type, third root and its type, taurodontism and its percentage, and dilaceration and its degree, using CBCT. Moreover, the association of these anomalies with demographic factors (e.g., age and gender) underwent analysis.
Materials and Methods
This cross-sectional study was conducted on 505 CBCT scans obtained from the Radiology Department of the School of Dentistry, Hamadan University of Medical Sciences, between 2019 and 2023. The sample size was calculated using NCSS statistical software (PASS 15; Kaysville, Utah: NCSS, LLC; 2020 available at https://www.ncss.com/software/pass), assuming a type I error of 0.05, an estimated proportion of mandibular molars with mesial canals to be 0.17 (17), and a confidence interval width of 0.067. Based on these parameters, the required sample size was determined to be 505 mandibular first and second molars. The eligible CBCT scans had optimal quality, visualized at least one mandibular molar (the first or second molar), and had been taken with the CS9600 CBCT scanner (Carestream Dental Rochester, NY, USA) with the exposure settings of 90 kVp tube potential, 10 mA tube current, 5 × 5-inch field of view, and 70 μm voxel size. CBCT scans without molar teeth, or molars with open apex, root resorption, history of trauma, restoration or crown, opacity or calcification in the pulp chamber or root canal system, and internal/external pathologies (periapical lesions and extensive or deep caries) were excluded from the analysis.
All CBCT scans were evaluated by one experienced and calibrated oral radiologist and one endodontist on a 20-inch monitor (LG, Seoul, Korea) with a 0.5 mm slice interval in a dimly lit room using OnDemand 3D Viewer. Scrolling was performed once in the corono-apical and then in the apico-coronal direction. Next, To relate the results/data to axial view findings, all CBCT scans were examined in coronal and sagittal views as well. The coronal, axial, and sagittal planes relative to the longitudinal axis of the tooth were evaluated by each observer as desired to assess the presence of any anomaly. Furthermore, the observers were free to do multi-planar reconstruction with no limitations and were allowed to zoom and change the brightness or contrast of the images. The presence and type of the mid-mesial canal, C-shaped canal, additional root(s), dilaceration, and taurodontism were recorded for each tooth by each observer.
In the case of disagreement, the final assessment was performed by another oral radiologist. To assess intra- and inter-observer agreements, all CBCT scans underwent evaluation again after a one-week interval by all three observers. Normally, mandibular molars have three root canals (two in the mesial and one in the distal root). The mid-mesial canal manifests as a fourth additional canal between the mesiobuccal and mesiolingual canals. Upon its observation in the axial section, other sections were also examined to ensure and confirm its presence (Figure 1).
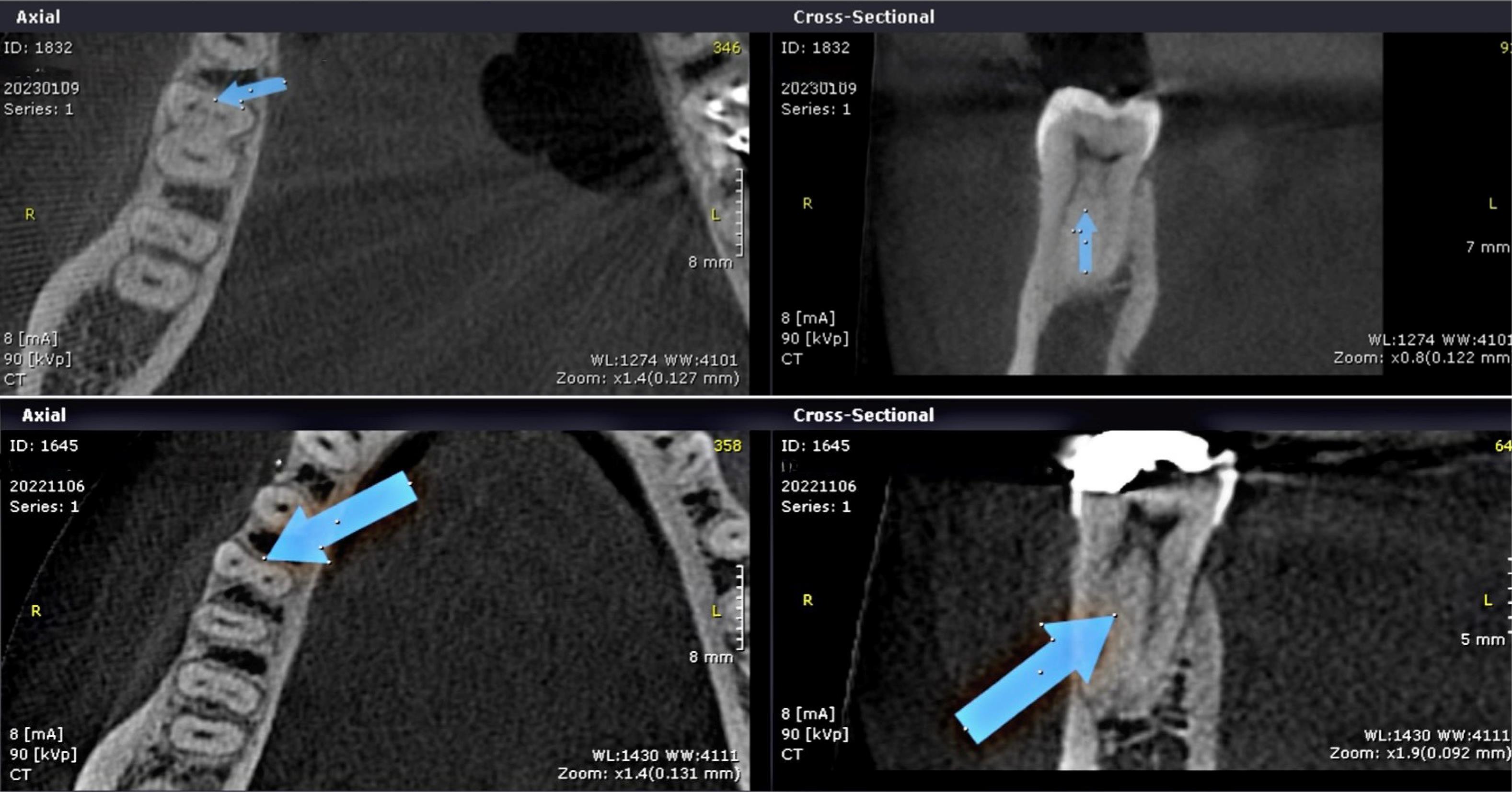
Figure 1.
Axial (A&C) and Cross-Sectional (B&D) CBCT Plane Showing Mid Mesial Canal Observed in the First Mandibular Molars. Note. CBCT: Cone-beam computed tomography
.
Axial (A&C) and Cross-Sectional (B&D) CBCT Plane Showing Mid Mesial Canal Observed in the First Mandibular Molars. Note. CBCT: Cone-beam computed tomography
Unlike the common anatomical variations of the root canal system, the external anatomy of mandibular molar teeth usually includes the presence of two roots with well-defined borders in most cases. One exception is the presence of an additional distolingual root referred to as the radix entomolaris. Another less common variation is the presence of an additional mesiobuccal root known as the radix paramolaris, which is detectable by the assessment of the axial section (Figure 2).

Figure 2.
Axial CBCT Plane Displaying Tooth 46 With Three Roots (A) and Tooth 36 With Four Roots (B). Note. CBCT: Cone-beam computed tomography.
.
Axial CBCT Plane Displaying Tooth 46 With Three Roots (A) and Tooth 36 With Four Roots (B). Note. CBCT: Cone-beam computed tomography.
In the present study, C-shaped canals were classified in axial sections (Figure 3), according to the classification by Fan et al (18), which has five types as follows:
-
C1: C-shaped canal with no interference
-
C2: Intermittent C-shaped canal in the form of a comma such that the alpha and beta angles are not smaller than 60 degrees
-
C3: Two or three separate canals with both alpha and beta angles smaller than 60 degrees
-
C4: One round or oval-shaped single canal
-
C5: No canal lumen

Figure 3.
Axial CBCT Plane Illustrating C-Shape Canal in Mandibular Molars. Note. CBCT: Cone-beam computed tomography
.
Axial CBCT Plane Illustrating C-Shape Canal in Mandibular Molars. Note. CBCT: Cone-beam computed tomography
In the present study, the definition by Chohayeb (19) was used for the detection of dilaceration such that any deviation over 20 degrees from the longitudinal tooth axis was considered as dilaceration (Figure 4). Moreover, the severity of dilaceration was recorded as mild (20-40 degrees), moderate (41-60 degrees), or severe ( > 60 degrees). Furthermore, the bending angle of dilaceration was measured using the method described by Schneider (20), where the angle formed between the two hypothetical lines connecting the apex and the orifice to the initiation point of the curve is measured. In case of the presence of dilaceration in only one root, the tooth was considered to have dilaceration, and if more than one root was affected, the highest value was reported.
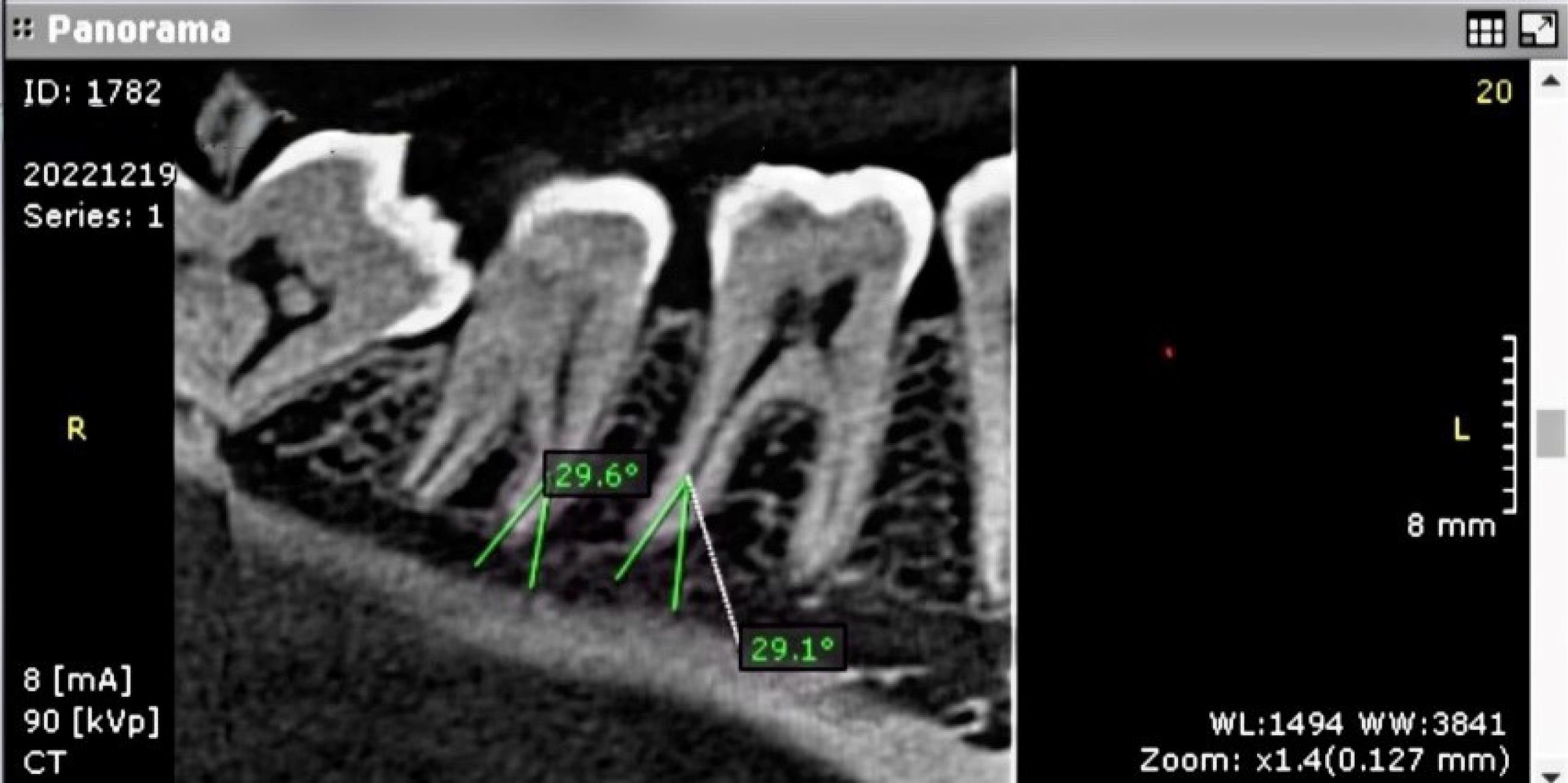
Figure 4.
Panoramic-Like CBCT Plane With 0 mm Thickness Depicting Dilaceration Degrees in Mandibular Molars. Note. CBCT: Cone-beam computed tomography
.
Panoramic-Like CBCT Plane With 0 mm Thickness Depicting Dilaceration Degrees in Mandibular Molars. Note. CBCT: Cone-beam computed tomography
The percentage of taurodontism on 3D radiographs was calculated as the ratio of the height of the pulp chamber, between the lowest point of the roof and the highest point of the floor, to the distance between the lowest point of the roof of the pulp chamber and the apex of the longest root multiplied by 100 (Figure 5); if this index was equal to or larger than 20, the tooth would be diagnosed with taurodontism. Index values between 20%–30%, 30%–40%, and 40%–75% indicated hypo-taurodontism, meso-taurodontism, and hyper-taurodontism, respectively. (13)
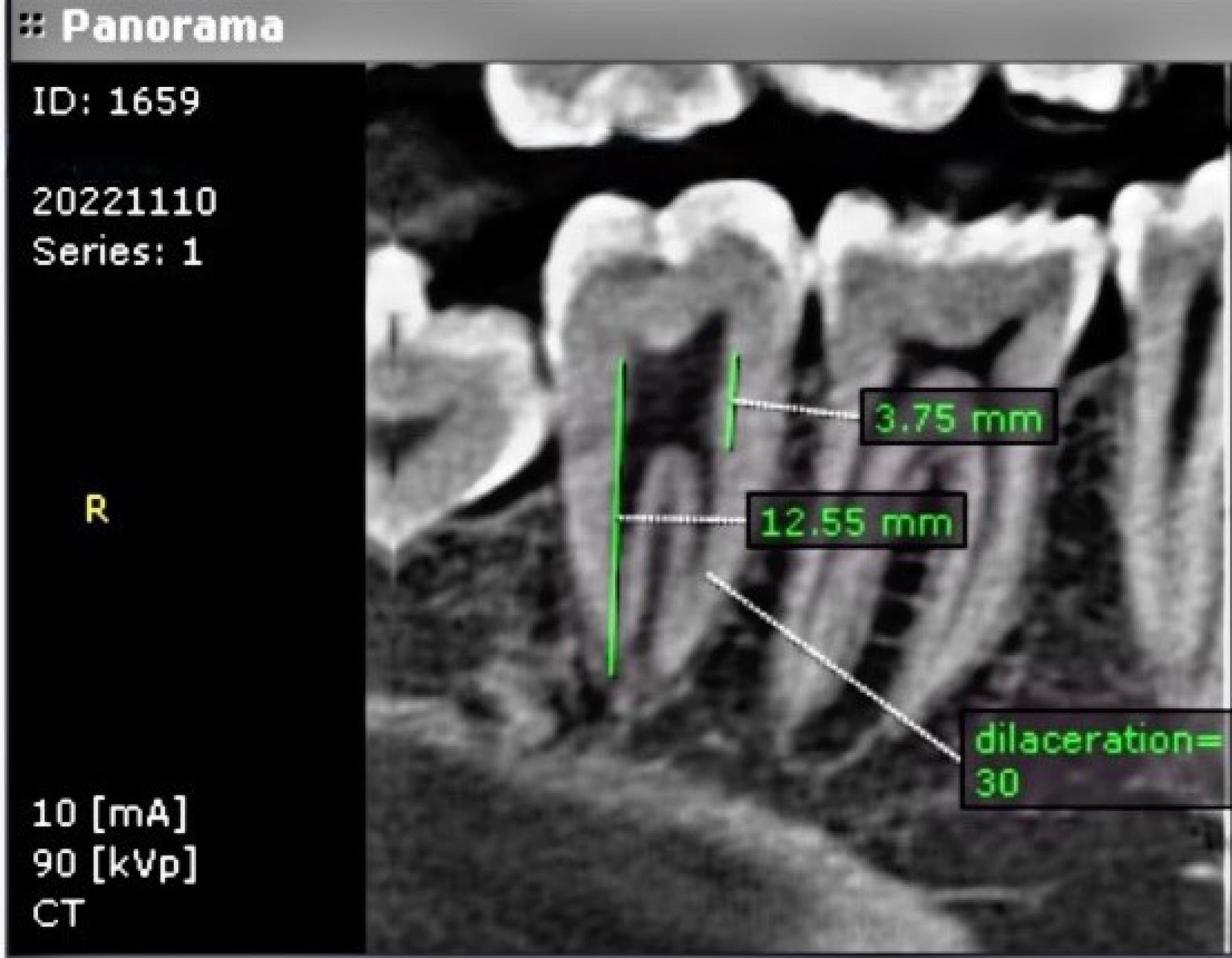
Figure 5.
Panoramic-Like CBCT Plane Showing Taurodontism Ratio Calculation (3.75/12.55 × 100) in the Second Mandibular Molar. Note. CBCT: Cone-beam computed tomography
.
Panoramic-Like CBCT Plane Showing Taurodontism Ratio Calculation (3.75/12.55 × 100) in the Second Mandibular Molar. Note. CBCT: Cone-beam computed tomography
The obtained data were analyzed by SPSS, version 25. The Shapiro-Wilk test was used to analyze the normality of data distribution. Quantitative variables were reported as means and standard deviations or medians (the first and third quartiles) and ranges, depending on the distribution of data. Qualitative variables were reported as numbers and percentages. Additionally, the association of anatomical anomalies with age and gender was analyzed by binary logistic regression.
Results
A total of 1202 CBCT scans were initially evaluated, out of which 505 scans, including 245 (48.52%) first molars and 260 (51.48%) second molars belonging to 375 females (74.85%) and 126 males (25.15%) with a mean age of 28 years (range 15–62 years), were enrolled according to the eligibility criteria.
Two observers evaluated the CBCT scans independently, and the kappa test demonstrated acceptable inter-observer (0.780) and intra-observer (0.983) agreements according to Altman’s scale.
Overall, 21 teeth (4.17%) had a mid-mesial canal. The prevalence of the mid-mesial canal was 4.89% and 3.45% in the first and second molars, respectively. However, no significant difference was found between the first and second molars regarding the percentage of teeth with a mid-mesial canal (P= 0.72).
The third root was observed in 20 teeth (3.96%), including 1.63% of the first molars and 6.15% of the second molars. First and second molars had a significant difference in the percentage of teeth with a third root, and the prevalence of the third root in mandibular second molars was significantly higher than that in mandibular first molars (P = 0.01). Of molars with a third root, 75% had a radix entomolaris, 20% had both radix entomolaris and radix paramolaris, and 5% had radix paramolaris.
The C-shaped canals were detected in 38 mandibular molars (7.52%); their frequency was 1.63% and 13.08% in the first and second molars, respectively. A significant difference was found in the percentage of C-shaped canals between the first and second molars, such that C-shaped canals were significantly more prevalent in mandibular second molars than in mandibular first molars (P < 0.000). Table 1 presents the frequency of C-shaped canals in permanent mandibular first and second molars.
Table 1.
Frequency Distribution of Different Types of C-Shaped Canals in Mandibular First and Second Molars
|
Permanent Molars With a C-Shaped Canal
|
Type of C-Shaped Canal
|
|
C1
|
C2
|
C3
|
C4
|
C5
|
| Mandibular first molars (n = 4) |
Number |
2 |
0 |
2 |
0 |
0 |
| Percentage |
50.00 |
0.00 |
50.00 |
0.00 |
0.00 |
| Mandibular second molars (n = 34) |
Number |
10 |
8 |
4 |
10 |
2 |
| Percentage |
29.41 |
23.53 |
11.76 |
29.41 |
5.88 |
| Total (N = 38) |
Number |
12 |
8 |
6 |
10 |
2 |
| Percentage |
31.58 |
21.05 |
15.79 |
26.32 |
5.26 |
Taurodontism was observed in 6 teeth (1.19%), including 0.41% of first molars and 1.92% of second molars. No significant difference was noted in the frequency of taurodontism between mandibular first and second molars (P= 0.22). Table 2 provides the frequency distribution of types of taurodontism in permanent mandibular first and second molars. In general, 162 mandibular molars (34.23%) had root dilaceration; it had a frequency of 29.80% in the first molars and 32.08% in the second molars. No significant difference was found between the first and second molars in terms of the frequency of dilaceration (P = 0.30).
Table 2.
Frequency Distribution of Different Types of Taurodontism in Permanent Mandibular First and Second Molars
|
Permanent Molars With Taurodontism
|
Type of Taurodontism
|
|
Hypo-Taurodontism
|
Meso-Taurodontism
|
Hypo-Taurodontism
|
| Mandibular first molars (n = 1) |
Frequency |
1 |
- |
- |
| Mandibular second molars (n = 5) |
4 |
1 |
- |
| Total (N = 6) |
5 |
1 |
- |
Table 3 lists the frequency of dilaceration in permanent mandibular first and second molars. Univariate logistic regression was used to analyze the correlation of anatomical anomalies with age and gender, which showed no association between age and gender with the presence of mid-mesial canal, third root, C-shaped canal, and dilaceration. Considering that the number of cases with taurodontism was extremely small, no logistic regression analysis was performed for this parameter (Table 4).
Table 3.
Frequency Distribution of Dilaceration Severity in Permanent Mandibular First and Second Molars
|
Permanent Molars With Dilaceration
|
Dilaceration Severity
|
|
Mild
|
Moderate
|
Severe
|
| Mandibular first molars (n = 73) |
Number |
63 |
10 |
- |
| Percentage |
86.30 |
13.70 |
- |
| Mandibular second molars (n = 89) |
Number |
79 |
8 |
2 |
| Percentage |
88.76 |
8.99 |
2.25 |
| Total (N = 162) |
Number |
142 |
18 |
2 |
| Percentage |
87.65 |
11.11 |
1.23 |
Table 4.
Results of Binary Logistic Regression Regarding the Association of Anatomical Anomalies of Mandibular Molars With Age and Gender
|
|
Odds Ratio
|
95% CI
|
P
value
|
| Presence of mid-mesial canal |
|
|
|
| Age |
0.98 |
0.91–1.06 |
0.58 |
| Gender |
0.49 |
0.06–4.13 |
0.51 |
| Presence of a third root |
|
|
|
| Age |
0.99 |
0.95–1.04 |
0.76 |
| Gender |
0.32 |
0.07–1.40 |
0.13 |
| Presence of a C-shaped canal |
|
|
|
| Age |
1.01 |
0.98–1.04 |
0.41 |
| Gender |
0.78 |
0.35–1.75 |
0.55 |
| Presence of dilaceration |
|
|
|
| Age |
0.98 |
0.97–1.00 |
0.09 |
| Gender |
0.81 |
0.52–1.26 |
0.35 |
Note. CI: Confidence interval.
Discussion
Detection of the mid-mesial canal in mandibular molars is essential for successful root canal therapy (3,4). The possibility of the presence of a mid-mesial canal was first proposed by Pomeranz (21), and since then, it has been demonstrated in different populations with various prevalence rates ranging from 3.41% (4) to 37.5% (2).
The prevalence of mid-mesial canal was found to be 4.17% in the current study, which was close to the value reported by Qiao et al (4) Several factors may be responsible for the variable prevalence rates, such as the method of assessment and detection of the mid-mesial canal. CBCT was used for this purpose in the present study and many previous studies, while some in vivo studies utilized an operating microscope intra-operatively for this purpose (2,22). Obviously, the latter method has the advantage of detecting negotiable canals, which is probably responsible for the higher prevalence rates reported in such studies. Nonetheless, a previous study pointed to the comparable efficacy of CBCT and the operating microscope for this particular diagnostic purpose (2). The study population is another influential parameter in this regard. Race can affect root morphology and anatomical variations of the root canal system. Accordingly, studies conducted on Iranian (3), Chinese (4), and American (5) populations confirmed 3.41%, 8.1%, and 13.72% prevalence rates for this anomaly, respectively. The possibility of racial affinity in Asia explains close values obtained in studies conducted in China and Iran. Tahmasbi et al (23) evaluated the prevalence of mid-mesial canal and isthmus in the mesial roots of mandibular molars using CBCT and reported the prevalence of mid-mesial canal to be 16.4%; its frequency in mandibular first molars was almost 3 times higher than that in mandibular second molars. No such significant difference was observed between first and second molars in the current study. The CBCT exposure settings, particularly the voxel size, are among other influential parameters. A recent study showed that a smaller voxel size can better reveal details, such as the presence of a second mesiobuccal canal in maxillary molars (24). Thus, scans taken with 70 µm voxel size and limited field of view were employed to achieve maximum resolution in the present study.
The presence of a distolingual third root is a common anatomical variation in mandibular molars. If the additional root is detected prior to root canal therapy, a larger access cavity would be prepared, and the prediction of the presence of an additional canal would improve the treatment prognosis (25). The reason behind the presence of radix entomolaris is unknown; however, it may be due to the effect of external factors during odontogenesis or the presence of specific genes. (25) The prevalence of radix entomolaris in mongoloid populations (Chinese, Eskimos, and American Indians) ranges from 5% to 30% (17). The frequency of the third root was 3.96% in the present study, which was close to rates found by Al-Alawi et al (26) in their study on a Saudi Arabian population (4.5% in mandibular first molars) and Talabani et al (17) in their study on an Iraqi population (4.1%–4.5%). A high variation exists in this regard in the literature, such that this rate varies from 1.9% in the Turkish population (27) to 33.3% in the Chinese population. (28) In the present study, gender had no significant association with the presence of the third root, which conforms to the findings of a study by Chandra et al (29) on an Indian population. However, some others reported a significant association in this respect (17,27). The presence of three-rooted mandibular second molars has been reported in the literature with a prevalence rate ranging from 0.26% to 8.98% (16,30). In the current study, the third root was a distolingual root in 75% of cases, which is in line with previous observations on other populations (31,32). Likewise, the frequency of four roots was 0.79% in our study, which was close to the value found in a previous study (0.6%) on an Emirati population (31).
C-shaped canal configuration was first suggested by Cooke and Cox (33) The reason behind this anatomical variation has been proposed to be the failure in the attachment of Hertwig’s epithelial root sheath at the buccal or lingual root surface. Knowledge about the prevalence of C-shaped canals in a population is important prior to root canal therapy to take the necessary measures, such as the use of an ultrasonic instrument for root canal irrigation and better mechanical preparation of the root canal isthmi, more efficient application of sealer with ultrasonic files, and the use of thermoplasticized gutta-percha for better obturation of isthmi. In the current study, the frequency of C-shaped canals was 13.08% in mandibular second molars; previous studies reported frequency values from 7.2% to 44.5% for C-shaped canals in mandibular second molars, depending on the race of the study population and methodology. (34) In the present study, C-shaped canals had a frequency of 1.63% in first molars, which was close to the prevalence rates reported in Latin American (35), Brazilian (6), Korean (36), and Israeli (37) populations. Unlike some previous studies that demonstrated a higher prevalence of C-shaped canals in females (32,34-36), the present study found no significant association between gender and C-shaped canal configuration. Similarly, there was no significant association between age and C-shaped canal configuration either, which corroborates previous findings. (32,35) Evidence shows that the prevalence of C-shaped canals is higher in East Asian populations compared with others. For instance, this value was 44.5% in the Korean population (38) and 39% in the Chinese population. (28) By moving toward the west, this value further decreased such that it was 12.3% in the Indian population, (39) 10% in the Thai population, (40) and 9.1% in a Saudi Arabian population. (34) The corresponding values were 14% and 8.5% in the Russian population (41) and the Portuguese population, respectively (42). In Mexico and Brazil (Latin America), this value was 14.2% (39) and 3.5%–15%, respectively (6,43). According to the prevalence range reported in the Middle East, that is, 8.9%–19.1% (44,45), the value obtained in the present study was somewhere in the middle of this range.
The assessment of morphological variations of the C-shaped canals according to the classification by Fan et al (18) revealed that the C1 form was most frequent in the coronal third. This finding is in line with the results of a previous study on Iranian and Emirati populations (31), while the C3 type had the highest prevalence in the Saudi Arabian population (34).
In the present study, the researchers attempted to select CBCT scans taken with the smallest voxel size available (70 µm) to obtain the highest resolution for the evaluation of the root canal anatomy. Taurodontism changes the pulp chamber and root canal morphology since it changes the crown/root ratio. Thus, knowledge in this regard is imperative prior to treatment since it affects all steps of treatment, such as canal negotiation, instrumentation, and obturation. The prevalence of taurodontism is variable in different racial groups (46). This difference may be due to the adopted technique for assessments or the applied classification system.
Previous studies reported variable prevalence rates for taurodontism in different populations; this rate was 8% in Saudi Arabian (47) and Jordanian (48) populations, 0.4% in north India, and 5.5% in southern Iran (49). This value was 1.19% in the present study. Such variations may be explained by racial and sample size differences.
Taurodontism is a developmental anomaly of Hertwig’s epithelial root sheath observed in some syndromes, such as Down syndrome, and even in healthy individuals. Some researchers have suggested that its cause is dentin deposition, a sort of adaptive response of the pulp to attrition due to heavy masticatory forces (50). Consistent with previous findings (39), the prevalence of C-shaped canals and taurodontism in second molars was higher than that in first molars. Further, in molars with taurodontism, the frequency of hypo-taurodontism was higher than that of meso-taurodontism (51). No case of hyper-taurodontism was observed in the present study. In general, the frequency of taurodontism was 1.19% in the current study. The prevalence of taurodontism has been variable in studies on molar teeth (including third molars). It had a prevalence of 1.5% in an Israeli population (52), 0.61% in a German population (53), and 4.41% in a Turkish population. (54) Some others, similar to the present investigation, only evaluated first and second molars (55).
The presence of dilaceration also affects root canal treatment success such that in severe cases of dilaceration, alternative treatments, such as vital pulp therapy, may be considered instead of root canal treatment. Similar to other anomalies, high variability exists in the reported prevalence rates for dilaceration in the literature. It is believed to be the most common anatomical variation in the Iranian population, accounting for 15% of all dental anomalies (56). In the present study, 34.23% of mandibular molars had root dilaceration. It should be noted that many previous studies used 2D radiography for its detection and reported prevalence rates below 9% for this anomaly (3,56). Obviously, since 2D radiographic modalities are incapable of visualizing the third dimension, many cases of dilaceration are missed in such studies, explaining the lower prevalence rates. Recently, Asheghi et al (57) evaluated the CBCT scans of an Iranian population and found that the prevalence of dilaceration was 28.8%, which is in conformity with the value obtained in the current study (34.23%).
This study was conducted on a small Iranian subpopulation, and the mean age of patients was 28 years (relatively young); thus, it may not be a true representation of the entire Iranian population. Future in vivo studies that include the same or larger sample size and use an endodontic microscope would probably yield more reliable results. Additionally, the gender distribution in this study was skewed, with 74.85% female participants, which may affect the generalizability of the findings. In addition, the effect of gender on the frequency of each anomaly could not be analyzed due to this limitation. While the current sample reflects the population that sought dental care at the Radiology Department during the study period, it may not fully represent broader populations. In light of this limitation, future studies should consider a more balanced gender distribution and various age groups to validate the results and increase the generalizability of the findings.
Conclusion
Mandibular first and second molars were not significantly different in the frequency of mid-mesial canal, taurodontism, and dilaceration. Considering the relatively high prevalence of dilaceration and C-shaped canals in the study population, these anatomical variations should be taken into consideration in root canal treatment.
Acknowledgements
This study was conducted at Tehran University of Medical Sciences. The authors would like to thank the staff and authorities of the university for supporting this study.
Competing Interests
The authors declare that they have no competing interests.
Ethical Approval
No ethical approval is applicable since this study has been conducted on extracted CBCT scans from the archive of the radiology department, and all patients had already signed informed consent before imaging for other diagnostic reasons and not for this investigation.
Funding
None.
References
- Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics 2005; 10(1):3-29. doi: 10.1111/j.1601-1546.2005.00129.x [Crossref] [ Google Scholar]
- Azim AA, Deutsch AS, Solomon CS. Prevalence of middle mesial canals in mandibular molars after guided troughing under high magnification: an in vivo investigation. J Endod 2015; 41(2):164-8. doi: 10.1016/j.joen.2014.09.013 [Crossref] [ Google Scholar]
- Kuzekanani M, Walsh LJ, Amiri M. Prevalence and distribution of the middle mesial canal in mandibular first molar teeth of the Kerman population: a CBCT study. Int J Dent 2020; 2020:8851984. doi: 10.1155/2020/8851984 [Crossref] [ Google Scholar]
- Qiao X, Zhu H, Yan Y, Li J, Ren J, Gao Y. Prevalence of middle mesial canal and radix entomolaris of mandibular first permanent molars in a western Chinese population: an in vivo cone-beam computed tomographic study. BMC Oral Health 2020; 20(1):224. doi: 10.1186/s12903-020-01218-z [Crossref] [ Google Scholar]
- Weinberg EM, Pereda AE, Khurana S, Lotlikar PP, Falcon C, Hirschberg C. Incidence of middle mesial canals based on distance between mesial canal orifices in mandibular molars: a clinical and cone-beam computed tomographic analysis. J Endod 2020; 46(1):40-3. doi: 10.1016/j.joen.2019.10.017 [Crossref] [ Google Scholar]
- Silva EJ, Nejaim Y, Silva AV, Haiter-Neto F, Cohenca N. Evaluation of root canal configuration of mandibular molars in a Brazilian population by using cone-beam computed tomography: an in vivo study. J Endod 2013; 39(7):849-52. doi: 10.1016/j.joen.2013.04.030 [Crossref] [ Google Scholar]
- Cantatore G, Berutti E, Castellucci A. Missed anatomy: frequency and clinical impact. Endod Topics 2006; 15(1):3-31. doi: 10.1111/j.1601-1546.2009.00240.x [Crossref] [ Google Scholar]
- Chen YC, Lee YY, Pai SF, Yang SF. The morphologic characteristics of the distolingual roots of mandibular first molars in a Taiwanese population. J Endod 2009; 35(5):643-5. doi: 10.1016/j.joen.2009.01.020 [Crossref] [ Google Scholar]
- De Moor RJ, Deroose CA, Calberson FL. The radix entomolaris in mandibular first molars: an endodontic challenge. Int Endod J 2004; 37(11):789-99. doi: 10.1111/j.1365-2591.2004.00870.x [Crossref] [ Google Scholar]
- de Pablo OV, Estevez R, Péix Sánchez M, Heilborn C, Cohenca N. Root anatomy and canal configuration of the permanent mandibular first molar: a systematic review. J Endod 2010; 36(12):1919-31. doi: 10.1016/j.joen.2010.08.055 [Crossref] [ Google Scholar]
- Gu Y, Lu Q, Wang P, Ni L. Root canal morphology of permanent three-rooted mandibular first molars: part II--measurement of root canal curvatures. J Endod 2010; 36(8):1341-6. doi: 10.1016/j.joen.2010.04.025 [Crossref] [ Google Scholar]
- Wang Y, Zheng QH, Zhou XD, Tang L, Wang Q, Zheng GN. Evaluation of the root and canal morphology of mandibular first permanent molars in a western Chinese population by cone-beam computed tomography. J Endod 2010; 36(11):1786-9. doi: 10.1016/j.joen.2010.08.016 [Crossref] [ Google Scholar]
- MacDonald D. Taurodontism. Oral Radiol 2020; 36(2):129-32. doi: 10.1007/s11282-019-00386-1 [Crossref] [ Google Scholar]
- Malcić A, Jukić S, Brzović V, Miletić I, Pelivan I, Anić I. Prevalence of root dilaceration in adult dental patients in Croatia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006; 102(1):104-9. doi: 10.1016/j.tripleo.2005.08.021 [Crossref] [ Google Scholar]
- Kuzekanani M, Sadeghi MT. Prevalence and distribution of dilacerations in the permanent dentition of an Iranian population. Eur J Anat 2019; 23(4):273-7. [ Google Scholar]
- Patel S, Brown J, Pimentel T, Kelly RD, Abella F, Durack C. Cone beam computed tomography in endodontics - a review of the literature. Int Endod J 2019; 52(8):1138-52. doi: 10.1111/iej.13115 [Crossref] [ Google Scholar]
- Talabani RM, Abdalrahman KO, Abdul RJ, Babarasul DO, Hilmi Kazzaz S. Evaluation of radix entomolaris and middle mesial canal in mandibular permanent first molars in an iraqi subpopulation using cone-beam computed tomography. Biomed Res Int 2022; 2022:7825948. doi: 10.1155/2022/7825948 [Crossref] [ Google Scholar]
- Fan B, Cheung GS, Fan M, Gutmann JL, Fan W. C-shaped canal system in mandibular second molars: part II--radiographic features. J Endod 2004; 30(12):904-8. doi: 10.1097/01.don.0000136206.73115.93 [Crossref] [ Google Scholar]
- Chohayeb AA. Dilaceration of permanent upper lateral incisors: frequency, direction, and endodontic treatment implications. Oral Surg Oral Med Oral Pathol 1983; 55(5):519-20. doi: 10.1016/0030-4220(83)90239-6 [Crossref] [ Google Scholar]
- Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol 1971; 32(2):271-5. doi: 10.1016/0030-4220(71)90230-1 [Crossref] [ Google Scholar]
- Pomeranz HH, Eidelman DL, Goldberg MG. Treatment considerations of the middle mesial canal of mandibular first and second molars. J Endod 1981; 7(12):565-8. doi: 10.1016/s0099-2399(81)80216-6 [Crossref] [ Google Scholar]
- Nosrat A, Deschenes RJ, Tordik PA, Hicks ML, Fouad AF. Middle mesial canals in mandibular molars: incidence and related factors. J Endod 2015; 41(1):28-32. doi: 10.1016/j.joen.2014.08.004 [Crossref] [ Google Scholar]
- Tahmasbi M, Jalali P, Nair MK, Barghan S, Nair UP. Prevalence of middle mesial canals and isthmi in the mesial root of mandibular molars: an in vivo cone-beam computed tomographic study. J Endod 2017; 43(7):1080-3. doi: 10.1016/j.joen.2017.02.008 [Crossref] [ Google Scholar]
- Mouzinho-Machado S, de Paula Lopes Rosado L, Coelho-Silva F, Neves FS, Haiter-Neto F, de-Azevedo-Vaz SL. Influence of voxel size and filter application in detecting second mesiobuccal canals in cone-beam computed tomographic images. J Endod 2021; 47(9):1391-7. doi: 10.1016/j.joen.2021.06.011 [Crossref] [ Google Scholar]
- Abella F, Mercadé M, Duran-Sindreu F, Roig M. Managing severe curvature of radix entomolaris: three-dimensional analysis with cone beam computed tomography. Int Endod J 2011; 44(9):876-85. doi: 10.1111/j.1365-2591.2011.01898.x [Crossref] [ Google Scholar]
- Al-Alawi H, Al-Nazhan S, Al-Maflehi N, Aldosimani MA, Zahid MN, Shihabi GN. The prevalence of radix molaris in the mandibular first molars of a Saudi subpopulation based on cone-beam computed tomography. Restor Dent Endod 2020; 45(1):e1. doi: 10.5395/rde.2020.45.e1 [Crossref] [ Google Scholar]
- Duman SB, Duman S, Bayrakdar IS, Yasa Y, Gumussoy I. Evaluation of radix entomolaris in mandibular first and second molars using cone-beam computed tomography and review of the literature. Oral Radiol 2020; 36(4):320-6. doi: 10.1007/s11282-019-00406-0 [Crossref] [ Google Scholar]
- Zhang R, Wang H, Tian YY, Yu X, Hu T, Dummer PM. Use of cone-beam computed tomography to evaluate root and canal morphology of mandibular molars in Chinese individuals. Int Endod J 2011; 44(11):990-9. doi: 10.1111/j.1365-2591.2011.01904.x [Crossref] [ Google Scholar]
- Chandra SS, Chandra S, Shankar P, Indira R. Prevalence of radix entomolaris in mandibular permanent first molars: a study in a South Indian population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011; 112(3):e77-82. doi: 10.1016/j.tripleo.2011.02.016 [Crossref] [ Google Scholar]
- Pan JY, Parolia A, Chuah SR, Bhatia S, Mutalik S, Pau A. Root canal morphology of permanent teeth in a Malaysian subpopulation using cone-beam computed tomography. BMC Oral Health 2019; 19(1):14. doi: 10.1186/s12903-019-0710-z [Crossref] [ Google Scholar]
- Khawaja S, Alharbi N, Chaudhry J, Khamis AH, Abed RE, Ghoneima A. The C-shaped root canal systems in mandibular second molars in an Emirati population. Sci Rep 2021; 11(1):23863. doi: 10.1038/s41598-021-03329-1 [Crossref] [ Google Scholar]
- Martins JNR, Marques D, Silva E, Caramês J, Mata A, Versiani MA. Prevalence of C-shaped canal morphology using cone beam computed tomography - a systematic review with meta-analysis. Int Endod J 2019; 52(11):1556-72. doi: 10.1111/iej.13169 [Crossref] [ Google Scholar]
- Cooke HG 3rd, Cox FL. C-shaped canal configurations in mandibular molars. J Am Dent Assoc 1979; 99(5):836-9. doi: 10.14219/jada.archive.1979.0402 [Crossref] [ Google Scholar]
- Alfawaz H, Alqedairi A, Alkhayyal AK, Almobarak AA, Alhusain MF, Martins JNR. Prevalence of C-shaped canal system in mandibular first and second molars in a Saudi population assessed via cone beam computed tomography: a retrospective study. Clin Oral Investig 2019; 23(1):107-12. doi: 10.1007/s00784-018-2415-0 [Crossref] [ Google Scholar]
- Nejaim Y, Gomes AF, de Paula Lopes Rosado L, Freitas DQ, Martins JN, da Silva EJ. C-shaped canals in mandibular molars of a Brazilian subpopulation: prevalence and root canal configuration using cone-beam computed tomography. Clin Oral Investig 2020; 24(9):3299-305. doi: 10.1007/s00784-020-03207-6 [Crossref] [ Google Scholar]
- Kim SY, Kim BS, Woo J, Kim Y. Morphology of mandibular first molars analyzed by cone-beam computed tomography in a Korean population: variations in the number of roots and canals. J Endod 2013; 39(12):1516-21. doi: 10.1016/j.joen.2013.08.015 [Crossref] [ Google Scholar]
- Shemesh A, Levin A, Katzenell V, Itzhak JB, Levinson O, Avraham Z. C-shaped canals-prevalence and root canal configuration by cone beam computed tomography evaluation in first and second mandibular molars-a cross-sectional study. Clin Oral Investig 2017; 21(6):2039-44. doi: 10.1007/s00784-016-1993-y [Crossref] [ Google Scholar]
- Jin GC, Lee SJ, Roh BD. Anatomical study of C-shaped canals in mandibular second molars by analysis of computed tomography. J Endod 2006; 32(1):10-3. doi: 10.1016/j.joen.2005.10.007 [Crossref] [ Google Scholar]
- von Zuben M, Martins JN, Berti L, Cassim I, Flynn D, Gonzalez JA. Worldwide Prevalence of Mandibular Second molar C-shaped morphologies evaluated by cone-beam computed tomography. J Endod 2017; 43(9):1442-7. doi: 10.1016/j.joen.2017.04.016 [Crossref] [ Google Scholar]
- Gulabivala K, Opasanon A, Ng YL, Alavi A. Root and canal morphology of Thai mandibular molars. Int Endod J 2002; 35(1):56-62. doi: 10.1046/j.1365-2591.2002.00452.x [Crossref] [ Google Scholar]
- Rogazkyn D, Metzger Z, Solomonov M. The prevalence and asymmetry of C-shaped root canals in second mandibular molars in a European-Russian population: a cone-beam computed tomography study in vivo. Int J Endod Rehabil 2016; 2(1):12-6. [ Google Scholar]
- Martins JN, Mata A, Marques D, Caramês J. Prevalence of C-shaped mandibular molars in the Portuguese population evaluated by cone-beam computed tomography. Eur J Dent 2016; 10(4):529-35. doi: 10.4103/1305-7456.195175 [Crossref] [ Google Scholar]
- Ladeira DB, Cruz AD, Freitas DQ, Almeida SM. Prevalence of C-shaped root canal in a Brazilian subpopulation: a cone-beam computed tomography analysis. Braz Oral Res 2014; 28:39-45. doi: 10.1590/s1806-83242013005000027 [Crossref] [ Google Scholar]
- Helvacioglu-Yigit D, Sinanoglu A. Use of cone-beam computed tomography to evaluate C-shaped root canal systems in mandibular second molars in a Turkish subpopulation: a retrospective study. Int Endod J 2013; 46(11):1032-8. doi: 10.1111/iej.12094 [Crossref] [ Google Scholar]
- Madani ZS, Mehraban N, Moudi E, Bijani A. Root and canal morphology of mandibular molars in a selected Iranian population using cone-beam computed tomography. Iran Endod J 2017; 12(2):143-8. doi: 10.22037/iej.2017.29 [Crossref] [ Google Scholar]
- Manjunatha BS, Kovvuru SK. Taurodontism-a review on its etiology, prevalence and clinical considerations. J Clin Exp Dent 2010; 2(4):e187-90. doi: 10.4317/jced.2.e187 [Crossref] [ Google Scholar]
- Jabali AH, Chourasia HR, Wasli AS, Alkhayrat AM, Mahnashi HM, Kamly MJ. Taurodontism in maxillary and mandibular molars using cone beam computed tomography in a dental center in Saudi Arabia. Ann Saudi Med 2021; 41(4):232-7. doi: 10.5144/0256-4947.2021.232 [Crossref] [ Google Scholar]
- Darwazeh AM, Hamasha AA, Pillai K. Prevalence of taurodontism in Jordanian dental patients. Dentomaxillofac Radiol 1998; 27(3):163-5. doi: 10.1038/sj/dmfr/4600342 [Crossref] [ Google Scholar]
- Bronoosh P, Haghnegahdar A, Dehbozorgi M. Prevalence of taurodontism in premolars and molars in the south of Iran. J Dent Res Dent Clin Dent Prospects 2012; 6(1):21-4. doi: 10.5681/joddd.2012.005 [Crossref] [ Google Scholar]
- Madeira MC, Leite HF, Niccoli Filho WD, Simões S. Prevalence of taurodontism in premolars. Oral Surg Oral Med Oral Pathol 1986; 61(2):158-62. doi: 10.1016/0030-4220(86)90179-9 [Crossref] [ Google Scholar]
- Aricioğlu B, Tomrukçu DN, Köse TE. Taurodontism and C-shaped anatomy: is there an association?. Oral Radiol 2021; 37(3):443-51. doi: 10.1007/s11282-020-00476-5 [Crossref] [ Google Scholar]
- Shifman A, Chanannel I. Prevalence of taurodontism found in radiographic dental examination of 1,200 young adult Israeli patients. Community Dent Oral Epidemiol 1978; 6(4):200-3. doi: 10.1111/j.1600-0528.1978.tb01150.x [Crossref] [ Google Scholar]
- Bürklein S, Breuer D, Schäfer E. Prevalence of taurodont and pyramidal molars in a German population. J Endod 2011; 37(2):158-62. doi: 10.1016/j.joen.2010.10.010 [Crossref] [ Google Scholar]
- Bilge NH, Yeşiltepe S, Törenek Ağırman K, Çağlayan F, Bilge OM. Investigation of prevalence of dental anomalies by using digital panoramic radiographs. Folia Morphol (Warsz) 2018; 77(2):323-8. doi: 10.5603/FM.a2017.0087 [Crossref] [ Google Scholar]
- MacDonald-Jankowski DS, Li TT. Taurodontism in a young adult Chinese population. Dentomaxillofac Radiol 1993; 22(3):140-4. doi: 10.1259/dmfr.22.3.8299833 [Crossref] [ Google Scholar]
- Ezoddini AF, Sheikhha MH, Ahmadi H. Prevalence of dental developmental anomalies: a radiographic study. Community Dent Health 2007; 24(3):140-4. [ Google Scholar]
- Asheghi B, Sahebi S, Zangooei Booshehri M, Sheybanifard F. Evaluation of root dilaceration by cone beam computed tomography in Iranian south subpopulation: permanent molars. J Dent (Shiraz) 2022; 23(2 Suppl):369-76. doi: 10.30476/dentjods.2021.91035.1547 [Crossref] [ Google Scholar]