Avicenna J Dent Res. 17(3):137-145.
doi: 10.34172/ajdr.2162
Original Article
Comparison of Healing in the Surgical and Non-Surgical Management of Periapical Lesions: A Prospective Clinical Study
P Edith Selva Sudashini Conceptualization, Data curation, Investigation, Resources, Visualization, Writing – original draft, Writing – review & editing, 1
S Rathna Piriyanga Conceptualization, Data curation, Investigation, Methodology, Validation, Writing – review & editing, 1
I Anand Sherwood Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, 1, * 
S Pavula Data curation, Resources, Visualization, 2
Author information:
1Department of Conservative Dentistry and Endodontics, CSI College of Dental Sciences and Research, Madurai, Tamil Nadu - 625001, India
2Department of Conservative Dentistry and Endodontics, Sarjug Dental College and Hospital & MATA R. Devi Dental Hospital, Laheriasarai, Darbhanga, Bihar-846003, India
Abstract
Background: Periapical lesions require accurate diagnosis and effective treatment, with healing serving as a key indicator of endodontic success. Advances in three dimensional imaging and volume analysis have enhanced the evaluation of treatment outcomes. This study assessed the outcomes of surgical and non-surgical endodontic treatments using three-dimensional (3D) volume analysis with a minimum 18-month follow-up. The study aimed to evaluate periapical lesion healing based on modified Penn’s 3D criteria and periapical index (PAI) scores using intraoral periapical radiographs (IOPA) and cone-beam computed tomography (CBCT) and analyze the impact of age, lesion size, treatment type, and materials on healing.
Methods: Ninety-six patients with periapical lesions larger than 10 mm, who underwent CBCT scans and received surgical, non-surgical root canal treatment, or surgical decompression (2017–2021), were included in this study. After dropouts, 64 patients received non-surgical treatment (n =31) and periapical surgery (n =31), respectively, and 1 patient received surgical decompression. Volume analysis was performed using ITK SNAP. Healing was assessed using the modified Penn’s 3D criteria and PAI scores derived from IOPA and CBCT. Finally, statistical analysis was conducted by paired sample t-tests, Levene’s test, and Mann-Whitney U test using SPSS 24.
Results: Mean lesion volume significantly decreased from 696.3961 mm³ to 79.7605 mm³ over 18–48 months. Initial lesion volumes differed significantly between non-surgical and surgical groups (P=0.001), but follow-up volumes demonstrated no difference (P =0.473). Similarly, the Mann-Whitney U test showed no statistically significant difference (P =0.094) between the surgical and non-surgical groups.
Conclusion: No statistical significance was observed in periapical lesion healing between surgical and non-surgical treatments despite the surgical group having larger initial volumes, supporting the efficacy of the treatment protocol and emphasizing proper case selection.
Keywords: Non-surgical root canal treatment, Periapical healing, Periapical surgery, Volume analysis
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Sudashini PES, Piriyanga SR, Sherwood IA, Pavula S. Comparison of healing in the surgical and non-surgical management of periapical lesions: a prospective clinical study. Avicenna J Dent Res. 2025;17(3):137-145. doi:10.34172/ajdr.2162
Background
Periapical lesions are inflammatory responses to microorganisms surrounding root surfaces and root canals, often triggered by trauma, caries, or developmental malformations. Treatment modalities encompass non-surgical root canal treatment, periapical surgery, surgical decompression, or tooth extraction (1,2). Periapical healing is an important prognostic factor that determines the outcome of root canal treatment (3). If non-surgical treatment is deemed ineffective or difficult, periapical surgery is the treatment of choice (4). The assessment of periapical pathologies is important for diagnosing and choosing the right treatment method, as well as evaluating its effectiveness. The radiographic depiction of healing in chronic apical periodontitis has traditionally been evaluated using the periapical index (PAI) criteria (5), as defined by Ørstavik et al. However, the limitations of these two-dimensional (2D) imaging techniques, such as anatomical structure overlap and background noise, underscore the importance of cone-beam computed tomography (CBCT) (6). CBCT provides a 3D perspective, facilitating a more accurate assessment of periapical lesion healing, size, localization, and bone thickness. Estrela et al developed the CBCT-PAI for evaluating the periapical area based on radiolucency measurements interpreted from CBCT scans. This index is determined by the largest extension of the lesion in three planes. Additional scores are assigned for the expansion (E) or destruction (D) of periapical cortical bone (7). Penn’s modified 3D criteria is a framework for evaluating healing in endodontic treatments, offering a multidimensional and comprehensive approach to assessment (8).Volume analysis represents a significant advancement in endodontic diagnostics and treatment planning, offering a more precise, detailed, and informative approach to managing periapical lesions (9).
Various studies have compared periapical lesion healing using CBCT between non-surgical root canal treatment and retreatment, healing after endodontic microsurgery, and 3D analysis of outcomes in non-surgical endodontic treatment (10-12). However, no studies have compared healing in surgical and non-surgical periapical lesions using 3D volume analysis.
Hence, this study aims to prospectively evaluate healing outcomes of surgical and non-surgical endodontic treatments using 3D volume analysis with a minimum 18-month follow-up. In addition, it seeks to assess healing based on modified Penn’s 3D criteria and PAI scores using intraoral periapical radiographs (IOPA) and CBCT and to examine the effect of age, initial lesion size, and treatment type on healing time.
- Null Hypothesis (H₀): There is no significant difference in healing outcomes between surgical and non-surgical treatments for periapical lesions over the 18–48-month follow-up period.
- Alternative Hypothesis (H₁): There is a significant difference in healing outcomes between surgical and non-surgical treatments for periapical lesions over the 18–48-month follow-up period.
Materials and Methods
Ethical clearance for this prospective clinical study was granted by the Institutional Ethical Board of CSI College of Dental Sciences and Research. The trial was registered with the Clinical Trials Registry-India (under the CTRI No. CTRI/2023/02/049775) in compliance with the Committee on Publication Ethics and International Committee of Medical Journal Editors guidelines. Patients presenting to the Department of Conservative Dentistry and Endodontics at CSI College of Dental Sciences and Research between January 2017 and November 2021 were prospectively recruited based on the inclusion criteria (Table 1).
Table 1.
Inclusion and Exclusion Criteria
|
Inclusion Criteria
|
Exclusion Criteria
|
-
Patient ASA I (normal healthy patients)
-
Patients aged 13–60 years with necrotic teeth and periapical lesions ( > 10 mm) with preoperative CBCT who underwent surgical or non-surgical root canal treatment
-
PAI score > 4
-
Failed root canal-treated tooth
|
-
Patients with systemic diseases
-
Pregnant patients
-
Open apices
-
A tooth with internal resorption
-
A tooth with a vertical root fracture
-
Patients not willing to recall visits
|
Note. CBCT: Cone beam computed tomography; PAI: Periapical index.
Clinical Procedure
After obtaining a written informed consent form from the patients, preoperative radiographs were captured using the paralleling technique. Patients with PAI scores exceeding 4 were subsequently recommended for CBCT imaging. The CBCT scans were obtained using the Ray Scan alpha plus machine (On-Demand 3D) with a field of view of 5*5, an exposure setting of 90 kVp, 10 mA, 14 seconds, and a voxel size of 70 μm. Initially, non-surgical treatment was planned for all cases. Therefore, patients with primary and secondary endodontic infections underwent root canal treatment and retreatment, respectively. Patients experiencing symptoms even after non-surgical treatment, with or without bone perforation in the labial, palatal, or both regions, were scheduled for periapical surgery. Surgical decompression was performed on cases with extensive periapical lesions to initially reduce lesion size and facilitate drainage.
Non-surgical Root Canal Treatment/Retreatment
The non-surgical management was conducted under rubber dam isolation with the administration of 2% lignocaine with 1:80,000 adrenaline (Lignox 2% A, Indoco Remedies Ltd.). The access opening was performed using an Endo-access bur (Dentsply Endo Access Bur FG 2, Dentsply Sirona). In cases of primary root canal treatment, the patency of the canals was confirmed using 10-sized or 15-sized K-files (Mani Company, Tochigi, Japan). For non-surgical retreatment, H-files (Mani Company, Tochigi, Japan) were utilized for gutta-percha retrieval after establishing an adequate glide path. Neoendo Flex (Orikam Healthcare India Private Ltd.) rotary instrumentation was employed following the manufacturer’s instructions. The irrigation protocol included the copious irrigation of 3 mL using saline with povidone-iodine, followed by a final rinse with 2% chlorhexidine gluconate (Anabond Asep-RC) (13). All treatments were conducted in two sessions, with calcium hydroxide used as an intracanal medicament (14).The medicament was placed inside the canal using a 40 K File (Mani Company, Tochigi, Japan), and a small cotton pellet was positioned over the orifice, followed by temporary restoration. Final obturation was performed after 2 weeks by placing Biodentine (Septodont, USA) in the apical area for approximately 4–5 mm with the assistance of hand pluggers (GDC, ISO-sized pluggers) (15), followed by the thermoplasticized obturation technique (Super Endo Beta, pen tip 20/4). In cases with thin, narrow canals, single cone obturation (Neoendo GP points, Orikam Healthcare India Private Ltd.) was conducted, with BioRoot RCS used as a sealer (16), and permanent composite restorations (Ivoclar Vivadent Te-Econom Plus Syringe Refill Universal Composite Resin) were provided.
Surgical Decompression
Patients were administered 2% lignocaine with 1:80 000 adrenaline. A small incision in the buccal gingiva via a full-thickness vertical approach was made to locate the lesion. Subsequently, using a round bur (702 Tapered fissure bur), a cavity was prepared within the bone at the specified anatomical location. Thorough irrigation of the cavity was conducted, with a solution comprising normal saline with povidone-iodine. A trimmed nasogastric tube was gently introduced into the cavity and sutured around the collar of the tube. As post-intervention care routine, patients were trained to perform cavity irrigation with 0.2% chlorhexidine twice daily. Subsequent to the intervention, the patient was scheduled for follow-up appointments at monthly intervals for a duration of three months, and the tube was removed at the end of the third month (17).
Periapical Surgery
The surgical procedure began with the administration of 4 mL of 2% lignocaine with 1:80 000 adrenaline. The flap elevation procedure was full-thickness, and the extension of the flap was modified depending on the size and extent of the lesion, and the operator’s need for direct visibility. Periapical surgery was exclusively performed on roots exhibiting periapical disease. The osteotomy was conducted using a handpiece-mounted rounded tungsten carbide drill (small round bur No. 2), with irrigation using sterile normal saline with povidone-iodine. Curettage was employed to eliminate the periapical lesion using a surgical curette (Lucas CL86). Root end resection was performed with a slow-speed straight handpiece, utilizing a No. 702 tapered fissure bur (18).Before the surgical procedure, a small amount of the patient’s own blood (10–40 mL) was collected into sterile-dried Monovettes without an anticoagulant. The collected blood was promptly centrifuged for 10 minutes at 2500 rpm, resulting in distinct layers, including a red lower fraction containing red blood cells, an upper straw-coloured cellular plasma, and the middle fraction containing the fibrin clot. The resulting clot was carefully extracted from the container using thin sterile forceps and entirely placed in a sterile glass container (19).
Finally, the patient’s platelet-rich fibrin and the bone graft (Bio-Oss -Xenograft) were carefully placed in the surgical cavity (20), and the flap was repositioned to its original position and sutured using Ethilon 4–0 non-absorbable surgical suture. All the sutures were removed after 10 days.
Volume Analysis
The patients were recalled and examined for signs and symptoms, such as pain and tenderness on percussion. A review radiograph was taken, and postoperative PAI scores were noted. Finally, the patients were referred for a review of CBCT for healing evaluation and volumetric analysis. Both preoperative and postoperative CBCT scans were utilized for volumetric analysis. The Digital Imaging and Communications in Medicine) files obtained from the CBCT scans were imported into the ITK-SNAP software (version 3.8.0) for processing. Manual segmentation was performed, with a focus solely on the periapical lesion and the associated tooth. This segmentation was carefully conducted in all three planes (sagittal, axial, and coronal) to ensure a comprehensive and precise delineation of the lesion.
Before initiating volumetric measurements, the threshold values in the software were adjusted to accurately differentiate the lesion from surrounding anatomical structures, such as bone, soft tissues, and teeth. This step was critical for isolating the lesion and ensuring the accuracy of the subsequent measurements. Once the threshold was set, segmentation was performed using a “bubble seeding” method. Small bubble-like markers were placed within the lesion, and these bubbles were expanded to outline and mark the entire lesion. The segmentation process visually highlights the periapical lesion, which appears in green for easier identification and verification. After the lesion was completely segmented, the volume of the lesion was calculated using the software’s volume measurement tool, available in the segmentation toolbar. The software automatically computes the lesion volume and displays the measurement (21) (Figures 1, 2, and 3).
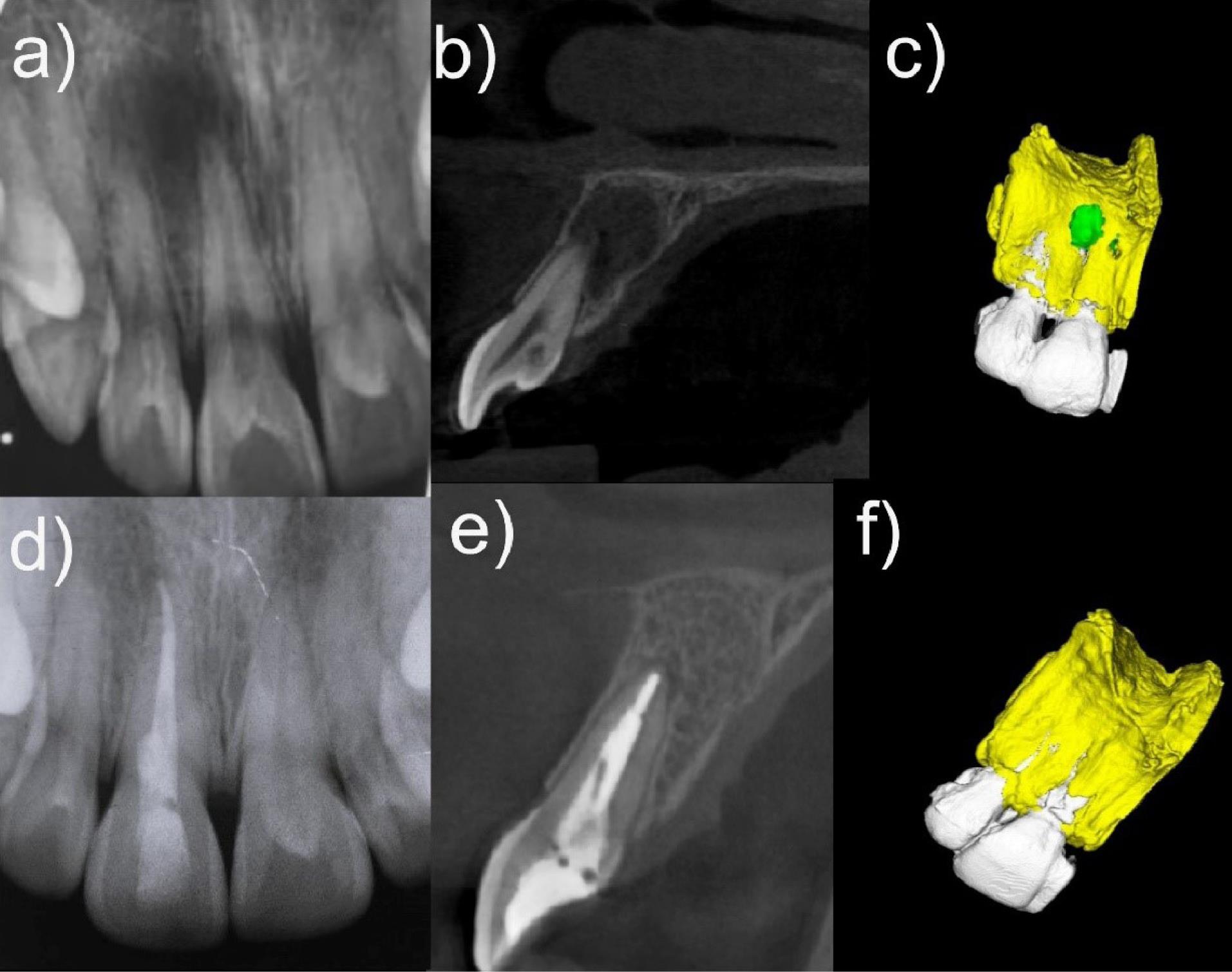
Figure 1.
Healing Following Non-surgical Root Canal Treatment. (a) Preoperative periapical radiograph showing periapical radiolucency in the maxillary right central and lateral incisors. (b) Sagittal CBCT slice demonstrating extensive periapical radiolucency at the apex of the central incisor. (c) 3D CBCT reconstruction using ITK-SNAP software depicting the lesion (green) relative to the surrounding bone (yellow). (d) Postoperative periapical radiograph taken 24 months later, showing complete lesion resolution. (e) Follow-up CBCT taken at 24 months revealing the healed periapical lesion. (f) 3D reconstruction using ITK-SNAP software displaying restored bone (yellow) after non-surgical root canal treatment. Note. CBCT: Cone beam computed tomography; 3D: Three-dimensional
.
Healing Following Non-surgical Root Canal Treatment. (a) Preoperative periapical radiograph showing periapical radiolucency in the maxillary right central and lateral incisors. (b) Sagittal CBCT slice demonstrating extensive periapical radiolucency at the apex of the central incisor. (c) 3D CBCT reconstruction using ITK-SNAP software depicting the lesion (green) relative to the surrounding bone (yellow). (d) Postoperative periapical radiograph taken 24 months later, showing complete lesion resolution. (e) Follow-up CBCT taken at 24 months revealing the healed periapical lesion. (f) 3D reconstruction using ITK-SNAP software displaying restored bone (yellow) after non-surgical root canal treatment. Note. CBCT: Cone beam computed tomography; 3D: Three-dimensional
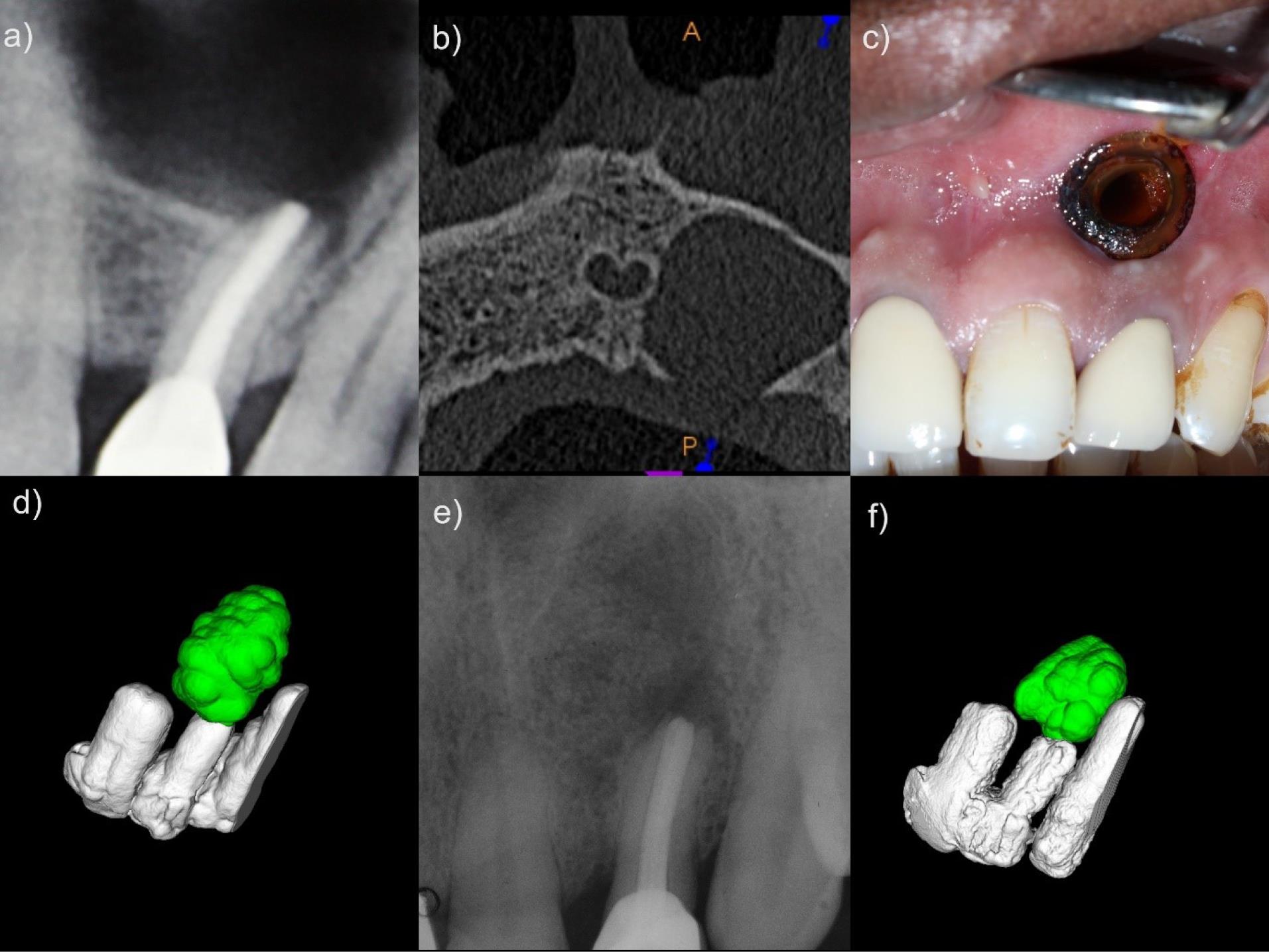
Figure 2.
Healing Following Surgical Decompression. a) Preoperative radiograph showing significant periapical radiolucency in a previously treated maxillary left lateral incisor. b) Axial CBCT view illustrating bone destruction. c) Clinical view of decompression stent placed through mucosal incision for drainage. d) 3D CBCT reconstruction using ITK-SNAP software highlighting the periapical lesion (green). e) Postoperative radiograph taken 18 months after decompression showing lesion healing. f) Final 3D CBCT reconstruction depicting reduced periapical lesion volume (green) after decompression. Note. CBCT: Cone beam computed tomography; 3D: Three-dimensional
.
Healing Following Surgical Decompression. a) Preoperative radiograph showing significant periapical radiolucency in a previously treated maxillary left lateral incisor. b) Axial CBCT view illustrating bone destruction. c) Clinical view of decompression stent placed through mucosal incision for drainage. d) 3D CBCT reconstruction using ITK-SNAP software highlighting the periapical lesion (green). e) Postoperative radiograph taken 18 months after decompression showing lesion healing. f) Final 3D CBCT reconstruction depicting reduced periapical lesion volume (green) after decompression. Note. CBCT: Cone beam computed tomography; 3D: Three-dimensional
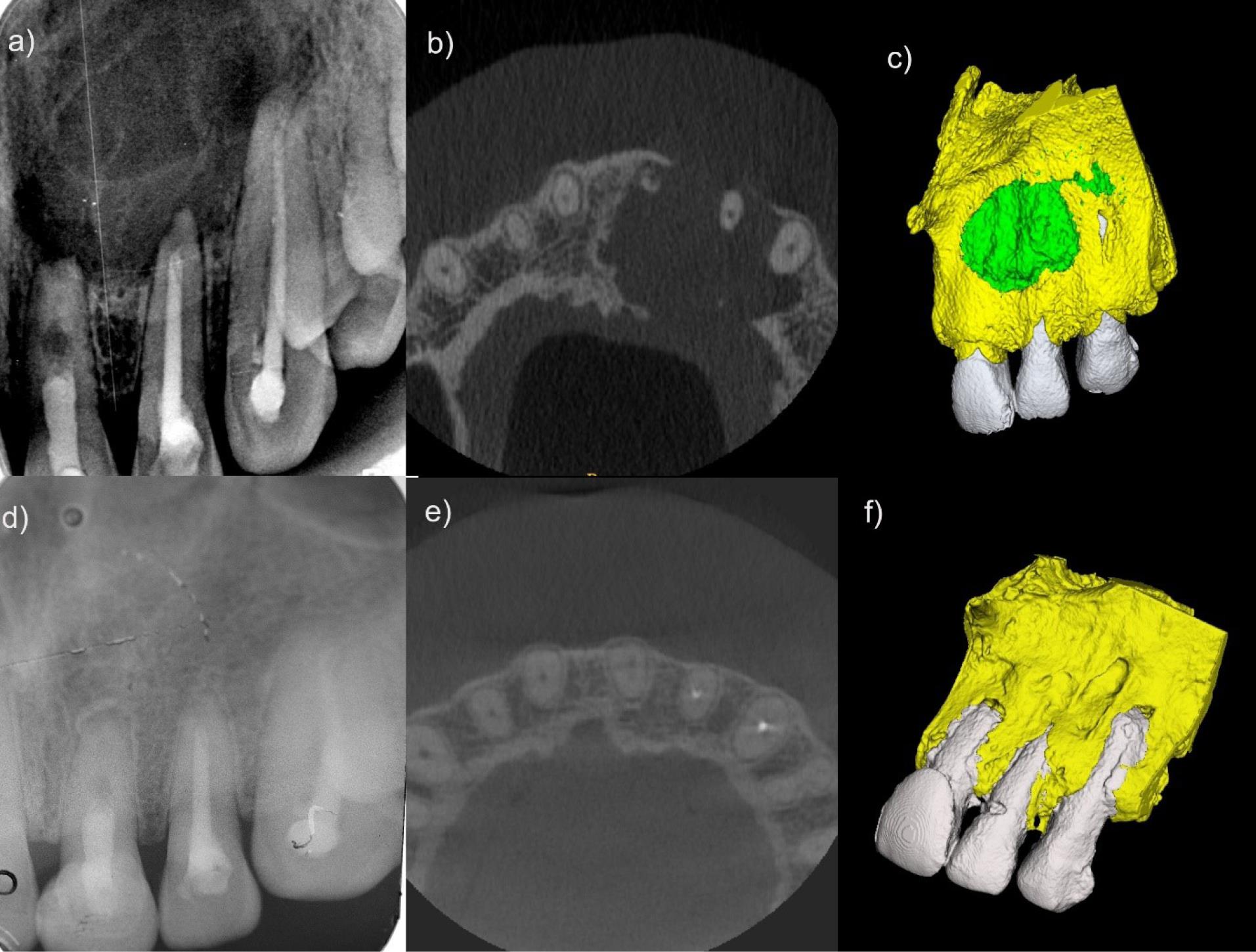
Figure 3.
Healing Following Periapical Surgery. a) Preoperative periapical radiograph showing periapical radiolucency of the maxillary left central and lateral incisors and the canine. b) Sagittal CBCT slice demonstrating extensive periapical radiolucency at the apex of the maxillary left central and lateral incisors and the canine. c) 3D CBCT reconstruction using ITK-SNAP software depicting the lesion (green) relative to the surrounding bone (yellow). d) Postoperative periapical radiograph taken 48 months later illustrating complete lesion resolution. e) Follow-up CBCT taken after 48 months revealing the healed periapical lesion. f) 3D reconstruction using ITK-SNAP software displaying restored bone (yellow) after periapical surgery. Note. CBCT: Cone beam computed tomography; 3D: Three-dimensional.
.
Healing Following Periapical Surgery. a) Preoperative periapical radiograph showing periapical radiolucency of the maxillary left central and lateral incisors and the canine. b) Sagittal CBCT slice demonstrating extensive periapical radiolucency at the apex of the maxillary left central and lateral incisors and the canine. c) 3D CBCT reconstruction using ITK-SNAP software depicting the lesion (green) relative to the surrounding bone (yellow). d) Postoperative periapical radiograph taken 48 months later illustrating complete lesion resolution. e) Follow-up CBCT taken after 48 months revealing the healed periapical lesion. f) 3D reconstruction using ITK-SNAP software displaying restored bone (yellow) after periapical surgery. Note. CBCT: Cone beam computed tomography; 3D: Three-dimensional.
Statistical Analysis
The paired t‐test was used to compare the preoperative and follow-up values of PAI IOPA, PAI-CBCT index scores, and the 3D volume. Levene’s test for equality was utilized to assess the equality between the two groups. Additionally, the Mann-Whitney U test was employed to compare the volume of lesions between the groups (e.g., surgical vs. non-surgical treatments) because lesion volume data did not follow a normal distribution, making it more suitable. Statistical analyses were performed using SPSS 23.0 (IBM 45 Corp, Washington, US), and all P values were considered significant at < 0.05.
Results
Out of 96 patients meeting the inclusion criteria, 64 (40 males [62.5%] and 24 females [37.5%]) were included in the study, and the remaining patients were classified as dropouts. Their ages ranged from 13 years to 47 years (mean: 24 years), with a follow-up of 18–48 months. The primary cause of periapical lesions was trauma (84.4%), followed by caries and dens invaginatus (7.8% each). The number of affected teeth ranged from 1 (64%) to 5 (1%), with maxillary incisors being most commonly involved (76.6%).
Of 64 patients, 44 had primary infections treated with root canal therapy (27 healed non-surgically, and 17 required periapical surgery). For 20 secondary infections, 5 healed non-surgically, and 14 required periapical surgery. Overall, 32 and 31 cases healed non-surgically and surgically, respectively, and 1 case healed via decompression. The Ørstavik’s PAI score, Estella’s CBCT score, modified PENN’S 3D criteria, and ITK-SNAP software were utilized for volume analysis.
Periapical Index Score (Ørstavik’s)
Preoperative scores showed 7 patients at 4 and 57 at 5. Follow-up scores improved significantly. Overall, 29 patients scored 1, 14 scored 2, and 15 scored 3 (Figure 4). Paired t-tests indicated significant improvements (P < 0.001). Mean scores decreased from 4.8125 to 2.0625 and from 4.9677 to 1.8387 for non-surgical and surgical cases, respectively. No significant follow-up difference was found between surgical and non-surgical groups (P = 0.404). In surgical decompression, the scores decreased from 5 to 4.
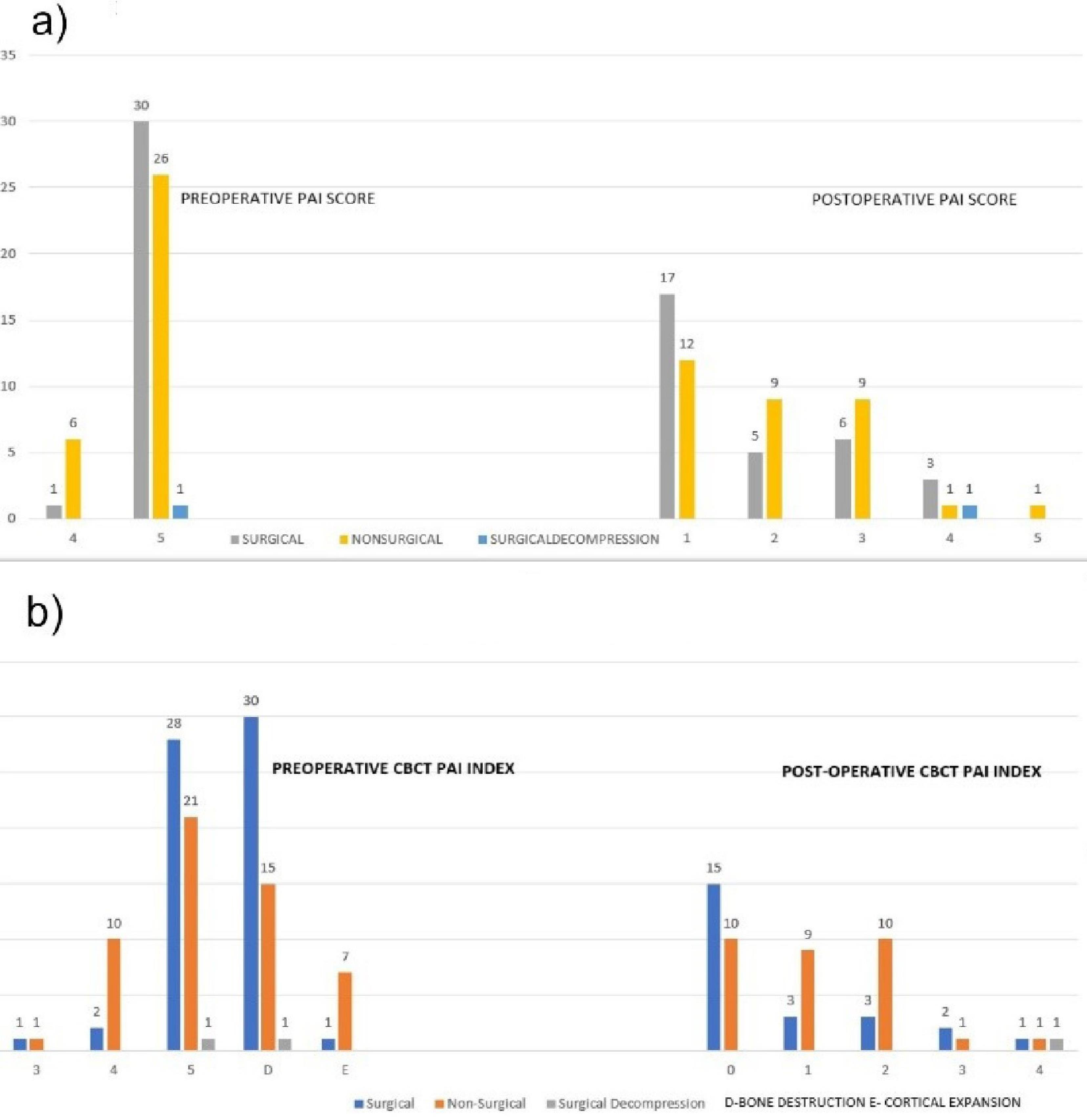
Figure 4.
Radiograph and CBCT PAI scores. a) Frequency distribution of preoperative and postoperative PAI scores (Ørstavik). b) Frequency distribution of preoperative and postoperative PAI CBCT index (Estrela scores). Note. PAI: Periapical index; CBCT: Cone beam computed tomography
.
Radiograph and CBCT PAI scores. a) Frequency distribution of preoperative and postoperative PAI scores (Ørstavik). b) Frequency distribution of preoperative and postoperative PAI CBCT index (Estrela scores). Note. PAI: Periapical index; CBCT: Cone beam computed tomography
Cone-Beam Computed Tomography Score Estrela’s
As regards preoperative CBCT scores, 2, 12, and 49 patients scored 3, 4, and 5, respectively. In the 56 follow-up cases, 25, 12, 13, 3, and 3 obtained scores of 0, 1, 2, 3, and 4, respectively, with 8 missing values (Figure 4). Paired t-tests showed a significant improvement in scores, from an average of 4.75 to 1.0536 (P = 0.000). For cases with bone destruction, 30 underwent surgical treatment, and 15 received non-surgical treatment. In surgical decompression, CBCT scores decreased from 5 (with bone destruction) to 4 (no bone destruction) after 18 months. The comparison of surgical and non-surgical groups demonstrated no significant difference in preoperative (P = 0.053) or follow-up (P = 0.229) scores.
Volume of the Lesion
The mean lesion volume significantly decreased from 696.3961 mm³ to 79.7605 mm³ over 18–48 months. A significant positive correlation (r = 0.270, P = 0.044) was noted between preoperative and follow-up volumes. A significant reduction (P < 0.001) in lesion size post-treatment was observed in the non-surgical group (31 cases). Likewise, significant changes were found in lesion size in 24 surgical cases (mean difference = -786.6425 mm³, P = 0.632). Surgical decompression resulted in volume reduction from 1619 mm³ to 663.3 mm³ over 18 months. Paired sample t-tests revealed significant differences in preoperative volumes between groups (P = 0.001), but follow-up volumes represented no significant difference (P = 0.473). The Mann-Whitney U Test confirmed a significant difference in preoperative volumes across treatment categories (P = 0.008), but there was no significant difference in follow-up volumes (P = 0.094), and the null hypothesis could not be rejected based on volume changes (Table 2).
Table 2.
Comparison of Lesion Volume Pre-Treatment and Post-Treatment in Non-Surgical and Periapical Surgery Groups
|
|
Non-Surgical Group
|
Periapical Surgery Group
|
|
Preoperative Volume of the Lesion (mm3)
|
Postoperative Volume of the Lesion (mm3)
|
Preoperative Volume of the Lesion (mm3)
|
Postoperative Volume of the Lesion (mm3)
|
| Mean |
526.6681 |
56.1561 |
841.8377 |
85.9354 |
| Median |
404.65 |
19.01 |
799.5 |
0.965 |
| Standard deviation |
359.39308 |
99.91982 |
466.04564 |
199.64504 |
Modified PENN’s Three-Dimensional Criteria
Non-surgical treatment achieved complete healing in 23 cases, uncertain healing in 8 cases, and limited healing in 1 case. Surgery resulted in complete healing in 24 cases, uncertain healing in 4 cases, and limited healing in 3 cases. Among 44 primary treatments, 35 achieved complete healing; among 20 retreatments, 12 achieved complete healing. Overall, younger patients (13–20 years) had the highest complete healing rate (24 of 28). Of 64 cases, 47, 11, and 6 showed complete, limited, and uncertain healing, respectively (Table 3).
Table 3.
Success Rates According to Modified PENN’S 3D Criteria (n)
|
Variables
|
Non-Surgical Root Canal Treatment
|
Periapical Surgery
|
Surgical Decompression
|
Total
|
|
Complete Healing
|
Limited
|
Uncertain
|
Complete Healing
|
Limited
|
Uncertain
|
Uncertain
|
| Age group |
|
|
|
|
|
|
|
|
| 13–20 |
13 |
2 |
- |
11 |
1 |
1 |
|
28 |
| 21–30 |
9 |
2 |
- |
8 |
- |
2 |
|
21 |
| 31–40 |
1 |
3 |
1 |
4 |
2 |
1 |
|
12 |
| 41–50 |
- |
1 |
- |
1 |
- |
- |
1 |
3 |
| Gender |
|
|
|
|
|
|
|
|
| Female |
10 |
2 |
1 |
8 |
1 |
2 |
- |
24 |
| Male |
13 |
6 |
- |
16 |
2 |
2 |
1 |
40 |
| Etiology |
|
|
|
|
|
|
|
|
| Trauma |
17 |
7 |
- |
23 |
3 |
3 |
1 |
54 |
| Caries |
4 |
- |
1 |
- |
- |
- |
- |
5 |
| Dens invaginatus |
2 |
1 |
- |
1 |
- |
1 |
- |
5 |
| Type of teeth |
|
|
|
|
|
|
|
|
| Mandibular incisors |
- |
2 |
- |
4 |
- |
- |
- |
6 |
| Maxillary central incisors |
19 |
6 |
- |
16 |
3 |
4 |
1 |
49 |
| Maxillary lateral incisors and canines |
- |
- |
- |
3 |
- |
- |
- |
3 |
| Maxillary premolars and molars |
- |
- |
- |
1 |
- |
- |
- |
1 |
| Mandibular molars |
4 |
- |
1 |
- |
- |
- |
- |
5 |
| Type of treatment |
|
|
|
|
|
|
|
|
| Primary root canal treatment |
21 |
6 |
- |
14 |
2 |
1 |
- |
44 |
| Secondary root canal treatment |
2 |
2 |
1 |
10 |
1 |
3 |
1 |
20 |
| Type of obturation |
|
|
|
|
|
|
|
|
| Biodentine as apical plug and thermoplasticized obturation |
17 |
8 |
1 |
24 |
3 |
4 |
1 |
58 |
| BioRoot RCS as a sealer and single cone obturation |
6 |
- |
- |
- |
- |
- |
- |
6 |
| Total |
23 |
8 |
1 |
24 |
3 |
4 |
1 |
64 |
Note. 3D: Three-dimensional.
Discussion
Periapical lesions, which are complex conditions affecting the tooth apex, are primarily due to persistent inflammation or infection of the dental pulp (22). Treatment options for these lesions include non-surgical endodontic treatment, periapical surgery, or extraction tailored to the specific case. Healing begins with inflammation and resolves with immunogen clearance, ideally showing no symptoms and radiographic abnormalities post-treatment (23). Clinical protocols should consider factors influencing the healing process. Non-surgical endodontic treatments often lead to the healing of most periapical lesions. Periapical surgery is preferred if non-surgical treatment is ineffective (24). Similarly, in this study, root canal treatment or retreatment was the primary option, with periapical surgery performed for symptomatic patients or those with bone perforations, and healing was monitored radiographically over 18–48 months.
The inclusion of both surgical and non-surgical endodontic treatments aimed to reflect a comprehensive clinical approach, acknowledging the spectrum of periapical pathologies encountered in practice. In addition, comparing surgical interventions with non-surgical root canal treatments helps assess therapeutic efficacy across different stages of disease progression. While primary and secondary infections are distinct pathophysiologically, consolidating them into a single cohort allowed for the evaluation of overall periapical healing dynamics under non-surgical management. This approach provides a broader understanding of treatment outcomes, considering the inherent variability in endodontic pathology and host responses.
CBCT stands out as a highly reliable method for detecting periapical radiolucency, boasting over 90% sensitivity and specificity (25). Linear measurements of periapical lesions in three spatial planes on CBCT surpass the accuracy of conventional 2D radiographs. Yushkevich et al demonstrated the reliability of ITK-SNAP for brain tumor volume measurement, showcasing its utility as a semi-automatic tool in complex segmentation scenarios where automatic methods may fall short (26). Similarly, in our study, ITK-SNAP was employed to measure periapical lesion volumes preoperatively and during follow-up, establishing its reliability. The use of 3D models of periapical lesions not only aids in patient education but also allows operators to precisely monitor healing in cubic mm, a level of detail unattainable with conventional imaging methods, including IOPA and CBCT.
The success of treatment interventions hinges on critical factors, including lesion size, patient age, symptom manifestation, and tooth vitality (27).Addressing the complexity of achieving complete resolution of periapical lesions while preserving optimal tooth form and function is essential. In this study, the strategic inclusion criteria targeted periapical lesions larger than 10 mm, recognizing the heightened clinical complexities associated with larger lesions. The investigation assessed the applicability and success rates of non-surgical and surgical interventions in managing large periapical pathologies. The analysis of healing outcomes through volume analysis revealed that there were significant preoperative lesion volume differences between the non-surgical root canal treatment and periapical surgery groups, with the latter showing higher volumes. However, there were no significant differences in lesion volumes between the groups in the follow-up. Therefore, the null hypothesis was accepted in this study.
Sodium hypochlorite is widely recognized for its tissue-dissolving ability and potent antimicrobial properties, making it the standard irrigant in endodontics. However, its cytotoxic potential, especially in high concentrations, poses a risk to periapical tissues. Chlorhexidine gluconate 2% was used as a safer alternative due to its strong antimicrobial activity and substantivity, although it lacks tissue-dissolving capabilities (28). Given that microbial reduction is a critical predictor of successful outcomes, chlorhexidine combined with povidone-iodine was chosen to balance disinfection with a reduced risk of tissue irritation.
Ng et al highlighted the importance of creating a fluid-tight seal in non-surgical treatment to prevent reinfection and promote healing—a critical factor in preventing root canal treatment failure (29). In the context of the present study, success can be attributed to the utilization of Biodentine for an apical seal (4–5 mm), thermoplasticized obturation, and composite restoration, providing an effective seal and contributing to increased fracture resistance, especially in teeth with thin dentinal walls. The reported success rates for periapical surgery range from 60% to 91% (30,31). Numerous factors can influence the outcomes of these surgeries, with retrofilling identified as a significant prognostic factor (32,33). In all cases, Biodentine is applied in the apical area, showcasing its non-cytotoxic nature and its capacity to stimulate collagen fiber and fibroblast formation (34). Despite the larger size of periapical lesions in the surgical group compared to the non-surgical group, the presence of Biodentine in the apical area, root-end resection, platelet-rich fibrin, and bone grafts are considered contributing factors to the reduced periapical lesion volume observed in the follow-up. This study underscores the importance of tailored treatment strategies for periapical lesions, highlighting the comparable effectiveness of non-surgical and surgical interventions.
A statistically significant preoperative prognostic factor in the successful healing rate was the patient’s age, with most patients aged 13–17 years experiencing complete healing. Younger patients exhibited a more favorable outcome, aligning with the findings of Liu et al (35). However, our findings contradict those of Saini et al (36), demonstrating that age was not a prognostic factor for the healing process.
According to Torabinejad et al (30), there is a significantly higher success rate for endodontic surgery at 2–4 years (77.8%) compared with non-surgical retreatment for the same follow-up period (70.9%). This finding underlines the efficacy of endodontic surgery in achieving favorable outcomes within the specified time frame, confirming its superiority over non-surgical retreatment. In our study, involving 20 patients (60%) undergoing retreatment procedures, 12 patients achieved complete healing, 3 had limited healing (15%), and 5 had uncertain healing (25%). This underscores the effectiveness of retreatment in resolving persistent intraradicular infections, which conforms to the substantial success rates reported in the literature and the need for periapical surgery for extraradicular infections.
Limitations of the Study
The study’s small sample size and uneven distribution across treatment groups may have affected generalizability. Further studies with larger, more balanced samples are required to validate these results.
In addition, 3D volume analysis is limited by imaging artifacts, operator-dependent segmentation, and thresholding challenges, which can affect accuracy.
Conclusion
Our findings revealed that among the 64 remaining patients, the mean lesion volume decreased significantly from 696.3961 mm³ to 79.7605 mm³ over 18 months to 48 months, indicating treatment efficacy. Initial lesion volumes differed significantly between the non-surgical root canal treatment and periapical surgery groups. Despite the surgical group having a higher mean preoperative volume, there was no statistical significance in periapical lesion healing, as assessed by volume analysis, between the surgical and non-surgical treatment groups. This finding suggests the efficacy of the treatment protocol and underscores the importance of ideal case selection.Additionally, according to modified Penn’s 3D criteria, both non-surgical root canal treatment and periapical surgery are effective in achieving complete healing, with a higher success rate observed in the periapical surgery group. Surgical decompression can be used in rare cases when the periapical lesion extends to important anatomical landmarks, initially reducing the size of the lesion and aiding in future planning for periapical surgery.
Future research with larger, balanced samples is needed to validate these findings and assess long-term outcomes across treatment modalities.
Competing Interests
There is no conflict of interests to declare.
Funding
This study was conducted without external funding or support.
References
- Karamifar K, Tondari A, Saghiri MA. Endodontic periapical lesion: an overview on the etiology, diagnosis and current treatment modalities. Eur Endod J 2020; 5(2):54-67. doi: 10.14744/eej.2020.42714 [Crossref] [ Google Scholar]
- Li X, Kolltveit KM, Tronstad L, Olsen I. Systemic diseases caused by oral infection. Clin Microbiol Rev 2000; 13(4):547-58. doi: 10.1128/cmr.13.4.547 [Crossref] [ Google Scholar]
- Siqueira JF Jr. Aetiology of root canal treatment failure: why well-treated teeth can fail. Int Endod J 2001; 34(1):1-10. doi: 10.1046/j.1365-2591.2001.00396.x [Crossref] [ Google Scholar]
- Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature - part 1 Effects of study characteristics on probability of success. Int Endod J 2007; 40(12):921-39. doi: 10.1111/j.1365-2591.2007.01322.x [Crossref] [ Google Scholar]
- Orstavik D, Kerekes K, Eriksen HM. The periapical index: a scoring system for radiographic assessment of apical periodontitis. Endod Dent Traumatol 1986; 2(1):20-34. doi: 10.1111/j.1600-9657.1986.tb00119.x [Crossref] [ Google Scholar]
- Venskutonis T, Plotino G, Juodzbalys G, Mickevičienė L. The importance of cone-beam computed tomography in the management of endodontic problems: a review of the literature. J Endod 2014; 40(12):1895-901. doi: 10.1016/j.joen.2014.05.009 [Crossref] [ Google Scholar]
- Estrela C, Bueno MR, Azevedo BC, Azevedo JR, Pecora JD. A new periapical index based on computed tomography. J Endod 2008; 34(11):1325-31. doi: 10.1016/j.joen.2008.08.013 [Crossref] [ Google Scholar]
- Ramis-Alario A, Tarazona-Álvarez B, Peñarrocha-Diago M, Soto-Peñaloza D, Peñarrocha-Diago M, Peñarrocha-Oltra D. The study of bone healing after endodontic microsurgery using cone beam computed tomography: a retrospective cohort study. J Clin Exp Dent 2022; 14(8):e652-60. doi: 10.4317/jced.58354 [Crossref] [ Google Scholar]
- Mackiewicz E, Bonsmann T, Kaczor-Wiankowska K, Nowicka A. Volumetric assessment of apical periodontitis using cone-beam computed tomography-a systematic review. Int J Environ Res Public Health 2023; 20(4):2940. doi: 10.3390/ijerph20042940 [Crossref] [ Google Scholar]
- Mosquera-Barreiro C, Ruíz-Piñón M, Sans FA, Nagendrababu V, Vinothkumar TS, Martín-González J. Predictors of periapical bone healing associated with teeth having large periapical lesions following nonsurgical root canal treatment or retreatment: a cone beam computed tomography-based retrospective study. Int Endod J 2024; 57(1):23-36. doi: 10.1111/iej.13993 [Crossref] [ Google Scholar]
- Metska ME, Parsa A, Aartman IH, Wesselink PR, Ozok AR. Volumetric changes in apical radiolucencies of endodontically treated teeth assessed by cone-beam computed tomography 1 year after orthograde retreatment. J Endod 2013; 39(12):1504-9. doi: 10.1016/j.joen.2013.08.034 [Crossref] [ Google Scholar]
- Machut K, Żółtowska A. Plasma rich in growth factors in the treatment of endodontic periapical lesions in adult patients: 3-dimensional analysis using cone-beam computed tomography on the outcomes of non-surgical endodontic treatment using A-PRF + and calcium hydroxide: a retrospective cohort study. J Clin Med 2022; 11(20):6092. doi: 10.3390/jcm11206092 [Crossref] [ Google Scholar]
- Mohammadi Z. Chlorhexidine gluconate, its properties and applications in endodontics. Iran Endod J 2008; 2(4):113-25. [ Google Scholar]
- Dako T, Pop M, Fulop J, Kantor J, Monea M. The use of calcium hydroxide as an intracanal medicament in the treatment of large periapical lesions: a review. Acta Med Transilv 2020; 25(2):58-60. doi: 10.2478/amtsb-2020-0033 [Crossref] [ Google Scholar]
- Pawar AM, Kokate SR, Shah RA. Management of a large periapical lesion using BiodentineTM as retrograde restoration with eighteen months evident follow up. J Conserv Dent 2013; 16(6):573-5. doi: 10.4103/0972-0707.120934 [Crossref] [ Google Scholar]
- Khandelwal A, Jose J, Teja KV, Palanivelu A. Comparative evaluation of postoperative pain and periapical healing after root canal treatment using three different base endodontic sealers - a randomized control clinical trial. J Clin Exp Dent 2022; 14(2):e144-52. doi: 10.4317/jced.59034 [Crossref] [ Google Scholar]
- Tian FC, Bergeron BE, Kalathingal S, Morris M, Wang XY, Niu LN. Management of large radicular lesions using decompression: a case series and review of the literature. J Endod 2019; 45(5):651-9. doi: 10.1016/j.joen.2018.12.014 [Crossref] [ Google Scholar]
- Pradeepa MR, Rahul B, Valliappan CT, Sherwood IA, Gutmann JL, Subramani RP. A simplified and cost-effective targeted endodontic guide for calcified canal negotiation and surgical management. Endodontology 2022; 34(4):293-9. doi: 10.4103/endo.endo_48_22 [Crossref] [ Google Scholar]
- Singh S, Singh A, Singh S, Singh R. Application of PRF in surgical management of periapical lesions. Natl J Maxillofac Surg 2013; 4(1):94-9. doi: 10.4103/0975-5950.117825 [Crossref] [ Google Scholar]
- Basta DG, Abu-Seida AM, El-Batouty KM, Tawfik HM. Effect of combining platelet-rich fibrin with synthetic bone graft on the healing of intrabony defects after apicectomy in dogs with periapical pathosis. Saudi Endod J 2021; 11(3):300-7. doi: 10.4103/sej.sej_191_20 [Crossref] [ Google Scholar]
- Schloss T, Sonntag D, Kohli MR, Setzer FC. A comparison of 2- and 3-dimensional healing assessment after endodontic surgery using cone-beam computed tomographic volumes or periapical radiographs. J Endod 2017; 43(7):1072-9. doi: 10.1016/j.joen.2017.02.007 [Crossref] [ Google Scholar]
- Sundqvist G, Figdor D. Endodontic treatment of apical periodontitis. In: Orstavik D, Pitt Ford TR, eds. Essential Endodontology. Oxford: Blackwell; 1998. p. 242-77.
- Holland R, de Souza V, Nery MJ, de Mello W, Bernabé PF, Otoboni Filho JA. Tissue reactions following apical plugging of the root canal with infected dentin chips A histologic study in dogs’ teeth. Oral Surg Oral Med Oral Pathol 1980; 49(4):366-9. doi: 10.1016/0030-4220(80)90149-8 [Crossref] [ Google Scholar]
- Lin LM, Huang GT, Rosenberg PA. Proliferation of epithelial cell rests, formation of apical cysts, and regression of apical cysts after periapical wound healing. J Endod 2007; 33(8):908-16. doi: 10.1016/j.joen.2007.02.006 [Crossref] [ Google Scholar]
- Patel S, Wilson R, Dawood A, Foschi F, Mannocci F. The detection of periapical pathosis using digital periapical radiography and cone beam computed tomography - part 2: a 1-year post-treatment follow-up. Int Endod J 2012; 45(8):711-23. doi: 10.1111/j.1365-2591.2012.02076.x [Crossref] [ Google Scholar]
- Yushkevich PA, Yang G, Gerig G. ITK-SNAP: an interactive tool for semi-automatic segmentation of multi-modality biomedical images. Annu Int Conf IEEE Eng Med Biol Soc 2016; 2016:3342-5. doi: 10.1109/embc.2016.7591443 [Crossref] [ Google Scholar]
- Nair PN. Pathogenesis of apical periodontitis and the causes of endodontic failures. Crit Rev Oral Biol Med 2004; 15(6):348-81. doi: 10.1177/154411130401500604 [Crossref] [ Google Scholar]
- Salas H, Vieira GC, Palomino I, Valero J, Pacheco-Yanes J, Campello AF. Outcome of endodontic treatment with chlorhexidine gluconate as main irrigant: a case series. Aust Endod J 2020; 46(3):307-14. doi: 10.1111/aej.12401 [Crossref] [ Google Scholar]
- Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature--part 2 Influence of clinical factors. Int Endod J 2008; 41(1):6-31. doi: 10.1111/j.1365-2591.2007.01323.x [Crossref] [ Google Scholar]
- Torabinejad M, Corr R, Handysides R, Shabahang S. Outcomes of nonsurgical retreatment and endodontic surgery: a systematic review. J Endod 2009; 35(7):930-7. doi: 10.1016/j.joen.2009.04.023 [Crossref] [ Google Scholar]
- Mead C, Javidan-Nejad S, Mego ME, Nash B, Torabinejad M. Levels of evidence for the outcome of endodontic surgery. J Endod 2005; 31(1):19-24. doi: 10.1097/01.don.0000133158.35394.8a [Crossref] [ Google Scholar]
- Friedman S. The prognosis and expected outcome of apical surgery. Endod Topics 2005; 11(1):219-62. doi: 10.1111/j.1601-1546.2005.00187.x [Crossref] [ Google Scholar]
- Ricucci D, Siqueira JF Jr. Diagnosis and management of root canal treatment failures. Endod Topics 2010; 22(1):1-35. [ Google Scholar]
- Chong BS, Riahi R, Mair LH. A study of the factors influencing the success of root canal treatment. Endod Dent Traumatol 1996; 12(1):10-6. [ Google Scholar]
- Liu SQ, Chen X, Wang XX, Liu W, Zhou X, Wang X. Outcomes and prognostic factors of apical periodontitis by root canal treatment and endodontic microsurgery-a retrospective cohort study. Ann Palliat Med 2021; 10(5):5027-45. doi: 10.21037/apm-20-2507 [Crossref] [ Google Scholar]
- Saini A, Nangia D, Sharma S, Kumar V, Chawla A, Logani A. Outcome and associated predictors for nonsurgical management of large cyst-like periapical lesions: a CBCT-based prospective cohort study. Int Endod J 2023; 56(2):146-63. doi: 10.1111/iej.13860 [Crossref] [ Google Scholar]