Avicenna J Dent Res. 17(2):84-89.
doi: 10.34172/ajdr.2111
Original Article
Failure Rates of Two Types of Mini-Screws as Orthodontic Anchors
Nasrin Farhadian Conceptualization, Methodology, Project administration, Supervision, Validation, Visualization, Writing – review & editing, 1, 2
Amirfarhang Miresmaeili Methodology, Project administration, Supervision, Validation, Visualization, Writing – review & editing, 1, 2
Anahita Morovat Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Validation, Visualization, Writing – original draft, Writing – review & editing, 1, 2, *
Behnaz Alafchi Formal analysis, Methodology, Software, Validation, Visualization, 3
Author information:
1Dental Research Center, Avicenna Institute of Clinical Sciences, Avicenna Health Research Institute, Hamadan University of Medical Sciences, Hamadan, Iran
2Department of Orthodontic, Dental School, Hamadan University, Hamadan, Iran
3Department of Biostatistics, School of Public Health, Hamadan University of Medical Sciences, Hamadan, Iran
Abstract
Background: In orthodontic treatments, mini-screws are used when absolute anchorage is required for tooth movement. In daily clinical practice, it is common to observe mini-screws loosening after implantation. The aim of this clinical trial was to compare the failure rates of Iranian and Korean mini-screws utilized as orthodontic anchorage.
Methods: In this study, 74 patients requiring anchorage with mini-screws in the upper jaw were randomly divided into study and control groups receiving Iranian (Poyanteb Company) and Korean (the JEIL brand) mini-screws, respectively. The patients were evaluated for stability or failure of the mini-screws at one week and then at one-, two-, and three-month intervals. Any degree of mobility was considered a failure. The data were analyzed using repeated measures ANOVA, Bonferroni post hoc test, and t test.
Results: There were no significant differences in the stability of Iranian and JEIL brand screws when compared at intervals of one week, one month, two months, and three months (P>0.05). Additionally, no significant differences were found when assessing the stability of Iranian and JEIL brands with 35 mini-screws in the buccal area. Finally, an examination of 39 mini-screws from both brands in the palatal region of the maxilla revealed no statistical differences.
Conclusion: In comparing Iranian and JEIL brand mini-screws, no significant difference was observed in the failure rate, with both demonstrating adequate efficiency and stability. Therefore, to reduce costs for patients, Iranian brands can be utilized effectively.
Keywords: Mini-screw, Orthodontic, Mobility
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Farhadian N, Miresmaeili A, Morovat A, Alafchi B. Failure rates of two types of mini-screws as orthodontic anchors. Avicenna J Dent Res. 2025;17(2):84-89. doi:10.34172/ajdr.2111
Background
Successful orthodontic treatment is built on the foundation of anchorage control, with absolute anchorage being the most preferred due to its ability to remain stationary during tooth movement. Mini-screws are popular due to their ease of implantation and removal, minimal tissue invasion, and minimal constraints on placement locations in the alveolar bone.
The use of intraosseous anchorage devices in orthodontics is widely prevalent. These devices have multiple applications, including molar distalization, incisor intrusion, and crossbite correction (1). They can be broadly categorized into osteointegrated (2) implants and mechanically retained implants, such as mini-screws (3). Due to their ease of placement and removal, high efficiency as anchorage devices, and acceptable patient compliance, mini-screws have garnered significant attention in orthodontic treatment (4-6).
Mini-screws must remain stable during the application of orthodontic forces without significant displacement in order to be effective and functional. However, the stability of mini-screws is one of their challenges, as their function is not based on osseointegration, such as implants; rather, only the threaded portion mechanically locks into the bone (1,5). Several factors influence the stability and success of mini-screws, particularly in the early stages. These factors can be classified into two main groups (host-related and screw-related). Host-related factors include bone quality, bone mass, cortical bone thickness, and the patient’s age, while screw-related factors encompass the length, diameter, and design (cylindrical and conical) of the mini-screws (6). Enhancing the diameter and length of mini-screws reduces their failure rates; however, this also increases the risk of contact with adjacent tooth roots (7,8). Additionally, enhancing the surface roughness of mini-screws contributes to greater stability within the bone (9).
Numerous studies have examined the success and failure rates of mini-screws during orthodontic treatment, reporting success rates ranging from 75% to over 90% (10-12). A systematic review study reported a failure rate of 13.5% for mini-screws (1), indicating that while mini-screws are sufficiently successful for clinical use, predicting treatment outcomes is not straightforward (13-15).
Today, various mini-screws, primarily made from titanium, are available for use in orthodontic treatment. Different commercial companies produce mini-screws with varying characteristics (e.g., length, diameter, design, and surface roughness). Recently, some companies in Iran have begun manufacturing titanium mini-screws similar to foreign models. However, there is limited information regarding these Iranian mini-screws as well as their stability and efficacy. The overall cost of these mini-screws has significantly increased, given the recent surge in currency prices over the past few years. Therefore, Iranian mini-screws can serve as a viable alternative to more expensive foreign counterparts if they possess suitable characteristics.
This study aims to compare the failure rates of Iranian and Korean (JEIL) mini-screws.
Materials and Methods
Trial Design
The study design and ethical considerations were approved by the Dental School of Hamadan University of Medical Sciences (identifier: IRCT20120215009014N479). In this double-blind clinical trial, 74 patients needing bone anchorage with mini-screws in the palatal or buccal area of the maxilla were selected from those referred to Hamadan Dental School.
Participants, Eligibility Criteria, and Settings
The patients had to be between 15 and 30 years old, and the placement of the mini-screw was part of their orthodontic treatment. Pregnant women, smokers, patients taking medications affecting bone metabolism, insufficient space between tooth roots, and the presence of a frenum in the buccal area of the mini-screw placement site were excluded from the study (6).
Before placing the mini-screws, periapical radiographs were taken to ensure adequate space between the mini-screw and the tooth root. Once written informed consent was obtained, patients were randomly divided into two groups. The study group received Iranian mini-screws (Poyanteb Company, Iran, Hamadan), and Korean mini-screws were utilized for the control group. The mini-screws of the self-drilling and self-tapping types, each measuring 8 mm in length and 1.6 mm in diameter, were inserted. Randomization was performed based on the age and gender of the patients using block randomization.
First, the patients were asked to brush their teeth and rinse their mouths with chlorhexidine mouthwash (for 45 seconds). Then, 20% lidocaine anesthesia was injected at the relevant site before placing the mini-screw. Subsequently, each mini-screw was placed perpendicularly to the bone using a manual driver at a predetermined site so that the threads of the screws were not visible. Periapical radiographs were taken again from each patient (6). The mini-screws were inserted by trained orthodontic postgraduate students.
Force application was performed immediately after loading the mini-screws with a force equivalent to 100–150 g with the Ni-Ti coil spring. The patients were then scheduled to return to the clinic for follow-up appointments one week later, followed by visits at one-month, two-month, and three-month intervals as part of their regular treatment. Any degree of mobility was considered a failure (15). A checklist was created for collecting patient data, including date of placement, age, gender, and placement site of the mini-screws (6,15).
Statistical Analysis
The collected data were analyzed using repeated measures analysis of variance, Bonferroni post hoc test, t test, and SPSS software (version 24), with a significance level of 0.05.
Results
This clinical trial, lasting for 3 months, included 74 patients (25 males and 49 females aged 15–30 years) with a total of 74 mini-screws inserted as orthodontic anchorage (Table 1). Overall, 78.4% of the mini-screws did not become lost. About 26.1% of Iranian and 25% of JEIL mini-screws inserted in palatal, and 14.3% of Iranian and 19% of JEIL mini-screws inserted in buccal failed after implantation (Figure 1A). Screws inserted in older patients showed greater stability compared to those in younger patients (Figure 1B).
Table 1.
Distribution of Mini-Screw Placements
|
Variables
|
Gender
|
Age (y)
|
Mini-screws
|
Screw Location
|
|
Female
|
Male
|
20>
|
20-25
|
25<
|
Iranian
|
JEIL
|
Palate
|
Buccal
|
| Frequency (%) |
49 |
25 |
37 |
28 |
9 |
37 |
37 |
39 |
35 |
| 66.2 |
33.8 |
50 |
37.8 |
12.2 |
50 |
50 |
52.7 |
47.3 |
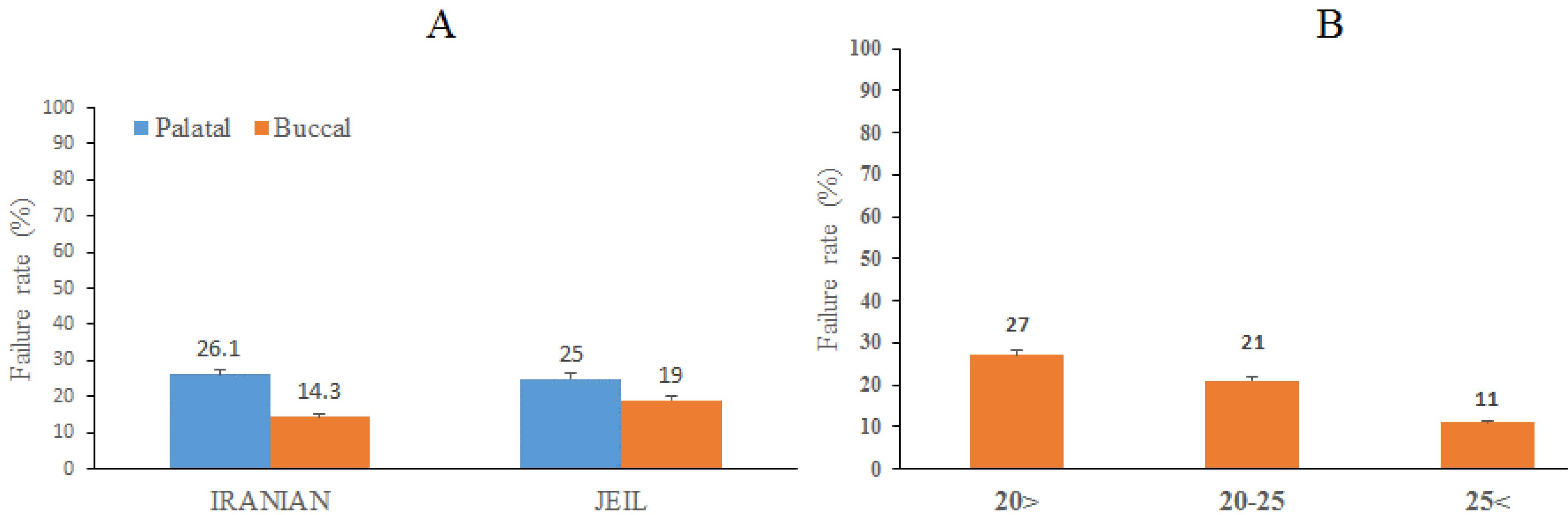
Figure 1.
Distribution of Failure Rates of Iranian and JEIL Mini-screws: (A) Percentage of Stability and Failure Rates of Iranian and JEIL Mini-Screws and (B) Percentage of Distribution of Failure Rates of Total Mini-Screws in Relation to Age
.
Distribution of Failure Rates of Iranian and JEIL Mini-screws: (A) Percentage of Stability and Failure Rates of Iranian and JEIL Mini-Screws and (B) Percentage of Distribution of Failure Rates of Total Mini-Screws in Relation to Age
Based on the comparison of the stability of Iranian mini-screws with JEIL brand screws at one-week, one-month, two-month, and three-month intervals, Iranian screws revealed no significant differences with Korean ones (P > 0.05, Table 2).
Table 2.
Stability Comparison of Iranian Mini-Screws and JEIL Brand at One-Week, One-Month, Two-Month, and Three-Month Intervals
|
Time
|
Number
|
Iranian
|
Number
|
JEIL
|
P
Value
|
|
Mobility
|
Immobility
|
Mobility
|
Immobility
|
| Week 1 |
37 |
1 (2.7) |
36 (97.3) |
37 |
0 (0.0) |
37 (100.0) |
0.50 |
| Month 1 |
36 |
3 (8.1) |
33 (89.2) |
37 |
4 (10.8) |
33 (89.2) |
0.516 |
| Month 2 |
33 |
4 (10.8) |
29 (78.4) |
33 |
3 (8.1) |
30 (81.1) |
0.50 |
| Month 3 |
29 |
0 (0) |
29 (78.4) |
30 |
1 (2.7) |
29 (78.4) |
0.508 |
No statistical difference was observed in the examination of 39 mini-screws from the Iranian and JEIL brands in the palatal region of the maxilla (Table 3).
Table 3.
Comparison of Stability of Iranian and JEIL Brand Mini-Screws in the Palatal Area of the Maxilla
|
Time
|
Iranian
|
JEIL
|
P
Value
|
|
Mobility
|
Immobility
|
Mobility
|
Immobility
|
| Week 1 |
0 (0.0) |
23 (100.0) |
0 (0.0) |
16 (100.0) |
- |
| Month 1 |
2 (8.7) |
21 (91.3) |
2 (12.5) |
14 (87.5) |
0.70 |
| Month 2 |
4 (19.05) |
17 (80.95) |
2 (14.3) |
12 (85.7) |
0.93 |
| Month 3 |
0 (0.0) |
17 (100.0) |
0 (0.0) |
12 (100.0) |
- |
The P value in the evaluation of 35 mini-screws from the JEIL and Iranian brands on the buccal side was greater than 0.05 (Table 4).
Table 4.
Stability Comparison of Iranian and JEIL Mini-Screws in the Buccal Area of the Maxilla
|
Time
|
Iranian
|
JEIL
|
P
Value
|
|
Mobility
|
Immobility
|
Mobility
|
Immobility
|
| Week 1 |
1 (7.1) |
13 (92.9) |
0 (0.0) |
21 (100.0) |
0.21 |
| Month 1 |
1 (7.6) |
12 (92.4) |
2 (9.54) |
19 (90.46) |
0.66 |
| Month 2 |
0 (0.0) |
12 (100.0) |
1 (5.20) |
18 (94.80) |
1.00 |
| Month 3 |
0 (0.0) |
12 (100.0) |
1 (5.48) |
17 (94.52) |
0.71 |
Discussion
This study provides valuable insights into the stability of mini-screws in orthodontics, comparing Iranian screws with the JEIL brand. The findings revealed no significant differences between Iranian and Korean screws initially. However, the mobility of mini-screws in both brands increased over time. This difference may be attributed to various factors, including manufacturing quality, cortical bone density and thickness, and the patient’s age (16).
In our analysis, the failure rate of JEIL and Iranian mini-screws was 21.6%. Success rates for mini-screws have been reported to range from 0% to 100%. Notably, only one study reported a 0% success rate for a particular type of mini-screw (17). Most studies, however, have recorded success rates above 80% (18). In this study, the success rates for both mini-screws ranged from 80% to 90%, which is consistent with previous findings (19). The variability in reported success rates can be attributed to differing success criteria across studies and the diverse characteristics of study samples. Factors such as patient age, gender, smoking habits, anatomic placement, dentoalveolar abnormalities, oral hygiene, type of mini-screw, and handling factors (e.g., surgical placement, force application, duration of loading, and type of orthodontic movement) all contribute to the differences observed in success rates (12). Long-term stability may be influenced by factors such as loading conditions and biological healing processes (20). Previous studies have shown that the initial stability of mini-screws is crucial, but long-term stability also depends on factors such as bone quality and placement techniques (16,21). For instance, the Dual Top Screw System (JEIL, Korea) used in our study showed significantly better primary stability compared to a similar system with the same dimensions, known as the Tomas Pin (Dentaurum, Germany) (22).
The failure rate of JEIL mini-screws placed in the buccal and palatal areas of the upper jaw was 19% and 25%, respectively, whereas, for Iranian mini-screws, it was 14.3% and 26.1%, respectively. Our findings are in line with those of other research involving 9–384 palatal implants or mini-screws, with follow-up periods ranging from 2 to 35.6 months, where failure risk varied from 0.0% to 26.1% (23). In another study, the success rate of orthodontic mini-implants was 89.8%, with an average loading period of 8.1 months. Soft-tissue infections were reported in 6.3–33.3% of cases, while screw mobility ranged from 3.1% to 20.8%, depending on the anatomical location. Screw mobility was notably higher in the buccal fold compared to the palate (P = 0.034) (24). Gurdan and Szalma demonstrated that mini-screws measuring 1.6 mm × 8 mm inserted in the buccal fold often loosen under immediate load, while those placed in the palate typically provide excellent skeletal anchorage (24).
In the palatal region, both brands showed similar stability over short-term periods. However, over longer periods, the JEIL brand performed better. The differences were minor, making it difficult to definitively conclude the superiority of one brand over the other. When comparing buccal mini-screws, the JEIL brand represented less mobility than the Iranian brand in the short-term periods (one week and one month). In longer time frames (two and three months), this difference gradually diminished, and by the three-month mark, the mobility of JEIL brand screws was greater than that of the Iranian brand. However, this difference was not statistically significant. One analysis found that the failure rate of mini-screws placed in the maxilla was 11.0% (95% confidence interval [CI]: 8.8–13.7), while the failure rate for those placed in the mandible was 16.5% (95% CI: 11.6–22.7) (25). The higher failure rate in the mandible may be due to greater bone density, the availability of cortical bone around the mini-screws, and the narrower vestibule compared to the maxilla (26). Watanabe et al also concluded that the failure rate of mini-screws placed in the maxilla was significantly lower than that in the mandible (27). This may explain the lower failure percentage observed in the current study. Conversely, the results of Alharbi et al indicated that jaw involvement does not affect failure rates (1).
Age was found to negatively correlate with the likelihood of mini-screw loosening, implying greater stability in screws placed in older patients compared to younger ones. This finding aligns with the results of the study by Xin et al, indicating a negative correlation between age and the progressive susceptibility of mini-screws to loosening (28). A meta-analysis by Hong et al also demonstrated significant differences in success rates between individuals over and under 20 years old (29). Alharbi et al noted an 8.60% failure rate for mini-screws in young patients (under 18 years) compared to 11.20% in adults (over 18 years) (1). Overall, studies using age cutoffs of > 20, 20–25, or 25 < years consistently showed higher mini-screw stability in older subjects. Miyawaki et al reported an 80% success rate for patients under 20 years old compared to 85–88% for those over 20, although these differences were not statistically significant (17). These results are consistent with those of other studies that used classification criteria of 18, 20, or 35 years, demonstrating greater mini-screw stability in older individuals (28). Some researchers attributed this issue to higher bone quality, bone quantity, and cortical bone thickness in older patients (7,30).
In the study performed by Geshay et al, the failure rate of loaded mini-screws was 32.9% (6), which is higher than the failure rate of Iranian mini-screws in the current study. This discrepancy may be attributed to differences in the length of the mini-screws (31). Tseng et al observed a 100% success rate when using 12 mm long screws (32). However, other studies suggested that while longer mini-screws can enhance stability, they also carry a higher risk of root damage. Therefore, screws of 6–8 mm in length are recommended for safe usage, a guideline adhered to in our study as well (33). Pan et al investigated the primary stability of mini-screws made of different materials with a diameter of 2 mm. They measured the resonance frequency of screws made of titanium alloy, with lengths of 10 mm and 12 mm, when inserted into bone with a cortical thickness of 2 mm. Measurements were taken at insertion depths of 2.2 mm and 6 mm (34). The results showed no significant difference in stability between mini-implants made of different materials. However, insertion depth played a critical role in stability. Deeper insertion not only improves outcomes but also reduces the stress between the bone and the mini-implant surface caused by tipping movements during screw insertion (35). The Screw System Dual Top used in our study demonstrated significantly better primary stability compared to a similar system, the Tomas Pin (Dentaurum, Germany), which has a diameter of 1.6 mm and a length of 8–10 mm (22). Miyawaki et al found that mini-screws with a diameter of 1.0 mm or less are susceptible to mobility and failure (17). Other researchers have reported similar results, noting only minimal improvements with slight increases in diameter. Consequently, they recommend avoiding mini-screws with diameters smaller than 1.3 mm (18).
This study had several limitations, including the small number of patients, the lack of long-term success assessments (6 months to 1 year), and the absence of matching groups based on age and bone density. One important reason for the failure of mini-screw placement and the occurrence of mobility is insufficient bone density (36,37). Bone density differs between the upper and lower jaws and at buccal and lingual/palatal surfaces in individuals. It is also different among individuals based on age and gender (38). Therefore, the lack of determining bone density prior to conducting this study may have impacted the results.
Conclusion
In any ideal treatment, the goal is to reduce the failure rate and increase the success rate of the treatment. Additionally, the economic feasibility and accessibility of the treatment should also be taken into consideration. Given the continuous rise in currency prices in recent years, the cost of imported mini-screws has shown a significant increase. Accordingly, attention has shifted toward domestically produced mini-screws, provided that they possess the necessary functionality and durability over time, as a suitable alternative to foreign models at a lower cost. In comparing both mini-screws used in this study, the Iranian mini-screws demonstrated no significant difference in failure rate and exhibited suitable performance and stability. Thus, Iranian brands can be utilized to reduce costs for patients.
Acknowledgments
This study was adapted from a research project submitted to Hamadan University of Medical Sciences (No. 140303292700).
Competing Interests
The authors declare that there is no conflict of interests.
Ethical Approval
The study was approved by the Ethics Committee of Hamadan University of Medical Sciences (identifier: IRCT20120215009014N479).
Funding
The study was funded by the Vice-Chancellor for Research and Technology, Hamadan University of Medical Sciences (No. 140303292700).
References
- Alharbi F, Almuzian M, Bearn D. Miniscrews failure rate in orthodontics: systematic review and meta-analysis. Eur J Orthod 2018; 40(5):519-30. doi: 10.1093/ejo/cjx093 [Crossref] [ Google Scholar]
- Weber D, Handel S, Dunham D. Use of osseointegrated implants for orthodontic anchorage. J Clin Orthod 2017; 51(7):406-10. [ Google Scholar]
- Nanda R, Uribe FA, Yadav S. Temporary Anchorage Devices in Orthodontics E-Book: Temporary Anchorage Devices in Orthodontics E-Book. Elsevier Health Sciences; 2019.
- Favero L, Brollo P, Bressan E. Orthodontic anchorage with specific fixtures: related study analysis. Am J Orthod Dentofacial Orthop 2002; 122(1):84-94. doi: 10.1067/mod.2002.124870 [Crossref] [ Google Scholar]
- Kau CH, English JD, Muller-Delgardo MG, Hamid H, Ellis RK, Winklemann S. Retrospective cone-beam computed tomography evaluation of temporary anchorage devices. Am J Orthod Dentofacial Orthop 2010;137(2):166.e1-166.e5. doi: 10.1016/j.ajodo.2009.06.019.
- Geshay D, Campbell P, Tadlock L, Schneiderman E, Kyung HM, Buschang P. Stability of immediately loaded 3 mm long miniscrew implants: a feasibility study. Dental Press J Orthod 2021; 26(1):e2119155. doi: 10.1590/2177-6709.26.1.e2119155.oar [Crossref] [ Google Scholar]
- Chen YJ, Chang HH, Huang CY, Hung HC, Lai EH, Yao CC. A retrospective analysis of the failure rate of three different orthodontic skeletal anchorage systems. Clin Oral Implants Res 2007; 18(6):768-75. doi: 10.1111/j.1600-0501.2007.01405.x [Crossref] [ Google Scholar]
- Cha JY, Kil JK, Yoon TM, Hwang CJ. Miniscrew stability evaluated with computerized tomography scanning. Am J Orthod Dentofacial Orthop 2010; 137(1):73-9. doi: 10.1016/j.ajodo.2008.03.024 [Crossref] [ Google Scholar]
- Dalessandri D, Salgarello S, Dalessandri M, Lazzaroni E, Piancino M, Paganelli C. Determinants for success rates of temporary anchorage devices in orthodontics: a meta-analysis (n > 50). Eur J Orthod 2014; 36(3):303-13. doi: 10.1093/ejo/cjt049 [Crossref] [ Google Scholar]
- Lim JE, Lim WH, Chun YS. Quantitative evaluation of cortical bone thickness and root proximity at maxillary interradicular sites for orthodontic mini-implant placement. Clin Anat 2008; 21(6):486-91. doi: 10.1002/ca.20671 [Crossref] [ Google Scholar]
- Al-Thomali Y, Basha S, Mohamed RN. Effect of surface treatment on the mechanical stability of orthodontic miniscrews. Angle Orthod 2022; 92(1):127-36. doi: 10.2319/020721-111.1 [Crossref] [ Google Scholar]
- Chen Y, Kyung HM, Zhao WT, Yu WJ. Critical factors for the success of orthodontic mini-implants: a systematic review. Am J Orthod Dentofacial Orthop 2009; 135(3):284-91. doi: 10.1016/j.ajodo.2007.08.017 [Crossref] [ Google Scholar]
- Crismani AG, Bertl MH, Celar AG, Bantleon HP, Burstone CJ. Miniscrews in orthodontic treatment: review and analysis of published clinical trials. Am J Orthod Dentofacial Orthop 2010; 137(1):108-13. doi: 10.1016/j.ajodo.2008.01.027 [Crossref] [ Google Scholar]
- Reynders R, Ronchi L, Bipat S. Mini-implants in orthodontics: a systematic review of the literature. Am J Orthod Dentofacial Orthop 2009;135(5):564.e1-564.e19. doi: 10.1016/j.ajodo.2008.09.026.
- Lee Y, Choi SH, Yu HS, Erenebat T, Liu J, Cha JY. Stability and success rate of dual-thread miniscrews. Angle Orthod 2021; 91(4):509-14. doi: 10.2319/083020-756.1 [Crossref] [ Google Scholar]
- Santiago RC, de Paula FO, Fraga MR, Picorelli Assis NM, Vitral RW. Correlation between miniscrew stability and bone mineral density in orthodontic patients. Am J Orthod Dentofacial Orthop 2009; 136(2):243-50. doi: 10.1016/j.ajodo.2007.08.031 [Crossref] [ Google Scholar]
- Miyawaki S, Koyama I, Inoue M, Mishima K, Sugahara T, Takano-Yamamoto T. Factors associated with the stability of titanium screws placed in the posterior region for orthodontic anchorage. Am J Orthod Dentofacial Orthop 2003; 124(4):373-8. doi: 10.1016/s0889-5406(03)00565-1 [Crossref] [ Google Scholar]
- Topouzelis N, Tsaousoglou P. Clinical factors correlated with the success rate of miniscrews in orthodontic treatment. Int J Oral Sci 2012; 4(1):38-44. doi: 10.1038/ijos.2012.1 [Crossref] [ Google Scholar]
- Watanabe K, Lee S, Lee D, Zheng F, Kyung HM, Kim DG. Evaluation of clinical parameters for the stability of 2 types of miniscrews. Am J Orthod Dentofacial Orthop 2022; 161(3):437-44. doi: 10.1016/j.ajodo.2020.09.035 [Crossref] [ Google Scholar]
- Motoyoshi M, Uemura M, Ono A, Okazaki K, Shigeeda T, Shimizu N. Factors affecting the long-term stability of orthodontic mini-implants. Am J Orthod Dentofacial Orthop 2010;137(5):588.e1-588.e5. doi: 10.1016/j.ajodo.2009.05.019.
- Wilmes B, Su YY, Drescher D. Insertion angle impact on primary stability of orthodontic mini-implants. Angle Orthod 2008; 78(6):1065-70. doi: 10.2319/100707-484.1 [Crossref] [ Google Scholar]
- Wilmes B, Drescher D. Impact of bone quality, implant type, and implantation site preparation on insertion torques of mini-implants used for orthodontic anchorage. Int J Oral Maxillofac Surg 2011; 40(7):697-703. doi: 10.1016/j.ijom.2010.08.008 [Crossref] [ Google Scholar]
- Reynders RM, Isaia L. Failure rates of palatal implants or mini-screws for orthodontic anchorage. Evid Based Dent 2019; 20(1):9-11. doi: 10.1038/s41432-019-0010-0 [Crossref] [ Google Scholar]
- Gurdan Z, Szalma J. Evaluation of the success and complication rates of self-drilling orthodontic mini-implants. Niger J Clin Pract 2018; 21(5):546-52. doi: 10.4103/njcp.njcp_105_17 [Crossref] [ Google Scholar]
- Stanford N. Mini-screws success rates sufficient for orthodontic treatment. Evid Based Dent 2011; 12(1):19. doi: 10.1038/sj.ebd.6400777 [Crossref] [ Google Scholar]
- Lim HJ, Eun CS, Cho JH, Lee KH, Hwang HS. Factors associated with initial stability of miniscrews for orthodontic treatment. Am J Orthod Dentofacial Orthop 2009; 136(2):236-42. doi: 10.1016/j.ajodo.2007.07.030 [Crossref] [ Google Scholar]
- Watanabe H, Deguchi T, Hasegawa M, Ito M, Kim S, Takano-Yamamoto T. Orthodontic miniscrew failure rate and root proximity, insertion angle, bone contact length, and bone density. Orthod Craniofac Res 2013; 16(1):44-55. doi: 10.1111/ocr.12003 [Crossref] [ Google Scholar]
- Xin Y, Wu Y, Chen C, Wang C, Zhao L. Miniscrews for orthodontic anchorage: analysis of risk factors correlated with the progressive susceptibility to failure. Am J Orthod Dentofacial Orthop 2022; 162(4):e192-202. doi: 10.1016/j.ajodo.2022.07.013 [Crossref] [ Google Scholar]
- Hong SB, Kusnoto B, Kim EJ, BeGole EA, Hwang HS, Lim HJ. Prognostic factors associated with the success rates of posterior orthodontic miniscrew implants: a subgroup meta-analysis. Korean J Orthod 2016; 46(2):111-26. doi: 10.4041/kjod.2016.46.2.111 [Crossref] [ Google Scholar]
- Lee SJ, Ahn SJ, Lee JW, Kim SH, Kim TW. Survival analysis of orthodontic mini-implants. Am J Orthod Dentofacial Orthop 2010; 137(2):194-9. doi: 10.1016/j.ajodo.2008.03.031 [Crossref] [ Google Scholar]
- Abdalla KL, Ali Mahmood TM. The effect of different orthodontic mini-implant brands and geometry on primary stability (an in vitro study). Heliyon 2023; 9(9):e19858. doi: 10.1016/j.heliyon.2023.e19858 [Crossref] [ Google Scholar]
- Tseng YC, Hsieh CH, Chen CH, Shen YS, Huang IY, Chen CM. The application of mini-implants for orthodontic anchorage. Int J Oral Maxillofac Surg 2006; 35(8):704-7. doi: 10.1016/j.ijom.2006.02.018 [Crossref] [ Google Scholar]
- Deguchi T, Nasu M, Murakami K, Yabuuchi T, Kamioka H, Takano-Yamamoto T. Quantitative evaluation of cortical bone thickness with computed tomographic scanning for orthodontic implants. Am J Orthod Dentofacial Orthop 2006;129(6):721.e7-721.e12. doi: 10.1016/j.ajodo.2006.02.026.
- Pan CY, Chou ST, Tseng YC, Yang YH, Wu CY, Lan TH. Influence of different implant materials on the primary stability of orthodontic mini-implants. Kaohsiung J Med Sci 2012; 28(12):673-8. doi: 10.1016/j.kjms.2012.04.037 [Crossref] [ Google Scholar]
- Büchter A, Wiechmann D, Koerdt S, Wiesmann HP, Piffko J, Meyer U. Load-related implant reaction of mini-implants used for orthodontic anchorage. Clin Oral Implants Res 2005; 16(4):473-9. doi: 10.1111/j.1600-0501.2005.01149.x [Crossref] [ Google Scholar]
- Hung E, Oliver D, Kim KB, Kyung HM, Buschang PH. Effects of pilot hole size and bone density on miniscrew implants’ stability. Clin Implant Dent Relat Res 2012; 14(3):454-60. doi: 10.1111/j.1708-8208.2010.00269.x [Crossref] [ Google Scholar]
- Samrit V, Kharbanda OP, Duggal R, Seith A, Malhotra V. Bone density and miniscrew stability in orthodontic patients. Aust Orthod J 2012; 28(2):204-12. [ Google Scholar]
- Migliorati M, Benedicenti S, Signori A, Drago S, Barberis F, Tournier H. Miniscrew design and bone characteristics: an experimental study of primary stability. Am J Orthod Dentofacial Orthop 2012; 142(2):228-34. doi: 10.1016/j.ajodo.2012.03.029 [Crossref] [ Google Scholar]