Avicenna J Dent Res. 17(2):79-83.
doi: 10.34172/ajdr.2037
Original Article
Assessment of the Prevalence and Characteristics of Periradicular Radiolucency Around the Mandibular Third Molar in Cone-Beam Computed Tomography Images
Bahareh Hekmat Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing, 1, * 
Adisa Hosseinzadeh Data curation, Funding acquisition, Validation, Visualization, 2
Author information:
1Department of Oral and Maxillofacial Radiology, School of Dentistry, Zanjan University of Medical Sciences, Zanjan, Iran
2Dentist, Private Practitioner, Zanjan, Iran
Abstract
Background: Mandibular third molar periradicular radiolucencies (MPRs) are typically positioned buccally or superiorly to the mandibular canal and are regarded as predictive indicators for paresthesia. This radiographic manifestation can resemble various jaw lesions, and it is imperative for dental professionals to possess a comprehensive understanding of the prevalence and characteristics associated with these radiographic appearances in dental imaging. Accordingly, this study aimed to investigate the prevalence and characteristics of MPRs observed on cone-beam computed tomography (CBCT) images to identify distinguishing features and associations that may have clinical relevance.
Methods: This cross-sectional study evaluated 235 CBCT images to investigate the prevalence and characteristics of radiolucency around the mandibular third molar (MPRs) among patients attending an oral and maxillofacial radiology center in Zanjan in 2023. Data regarding the types of radiolucency surrounding the mandibular third molar, their specific locations, and the age and gender of the patients were systematically recorded. The Chi-square test was employed to assess the association between the prevalence of MPRs and qualitative nominal variables (e.g., gender), as well as continuous quantitative variables (e.g., age). The obtained data were analyzed using SPSS 26, with a significance level set at P<0.05.
Results: A total of 235 CBCT radiographs were examined, comprising 141 (60%) women and 94 (40%) men, with ages ranging from 16 to 81 years. Overall, 23 cases of MPRs were identified among the reviewed CBCT images.
Conclusion: The findings indicated a low prevalence of MPRs within the studied population. Furthermore, there was no statistically significant association between the prevalence of MPRs and gender. The majority of MPR cases were unilateral, and the results demonstrated no instances of bone expansion or tooth root resorption.
Keywords: Cone-beam computed tomography, Radicular, Mandibular
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Hekmat B, Hosseinzadeh A. Assessment of the prevalence and characteristics of periradicular radiolucency around the mandibular third molar in cone-beam computed tomography images. Avicenna J Dent Res. 2025;17(2):79-83. doi:10.34172/ajdr.2037
Background
Mandibular periradicular radiolucencies (MPRs) were first defined by Bohay et al as an oval radiolucency with well-defined margins and a sclerotic border located distally to the roots of the mandibular third molar. No association was observed between this radiolucency and the oral cavity or the periodontal ligament (PDL) space in panoramic radiographs. The lamina dura and PDL space were also normal (1). MPRs present as a round to oval radiolucent area with well-defined margins and a sclerotic border, with an average diameter ranging from 6.1 to 8.7 mm. It is typically located laterally to the root and often superior to the mandibular canal (2-4). This radiolucent manifestation, which is part of the anatomical structures, can mimic certain jaw lesions such as paradental cysts, pericoronitis, Stafne cysts, pathological periapical inflammation, and pathological dental follicles (5,6). An impacted tooth has not erupted into the dental arch within the expected scheduled time. Teeth often remain impacted due to insufficient space, typically when the length of the alveolar arch is shorter than the dental arch. Factors contributing to improper eruption direction include interference from adjacent teeth, dense covering bone, excessive soft tissue, and genetic disorders. The mandibular third molar is the most commonly impacted tooth in the jaws. Indications for removing an impacted tooth include the prevention of periodontal disease, tooth decay, pericoronitis, root resorption, the formation of odontogenic cysts and tumors, treatment of facial pain of unknown origin, prevention of jaw fractures, facilitating orthodontic treatment, the presence of impacted teeth under prosthetics, and ideal periodontal restoration. The most common cyst around the mandibular third molar is the dentigerous cyst, and ameloblastoma is the most common tumor (7-9). The surgical extraction of an impacted mandibular third molar is a common procedure in dental practice. To minimize postoperative complications, the surgeon must have information about the impacted third molar, such as root shape, root position, and the relationship between the inferior alveolar canal and the roots. Several radiographic indicators can increase the likelihood of injury to the inferior alveolar nerve, including root darkening, canal deviation, disruption of the cortical borders, and apex proximity to the canal, which are the best predictors of future sensory-nerve damage. Recent studies have identified MPRs as predictive indicators for nerve injury (10-13). Panoramic imaging is usually considered the standard diagnostic tool for preoperative evaluation; however, this imaging method has limitations, such as horizontal and vertical magnification, image distortion, overlap, and the presentation of a 2-dimensional (2D) image of a 3D structure, as well as the influence of patient positioning on image quality (6,14). Cone-beam computed tomography (CBCT) was first introduced in 2001, after which researchers focused on the ability of this technique to diagnose maxillofacial issues. Today, CBCT is widely used in dentistry to obtain 3D images of the jaws. This imaging method provides high-resolution images and accurate scans in three dimensions (coronal, sagittal, and axial), with a resolution of less than 1 mm and lower radiation doses to the patient compared to conventional computed tomography (6). When MPRs are located mesially or distally relative to the third molar, they can be detected in panoramic images. However, the accuracy of panoramic imaging is significantly reduced when positioned between the roots of teeth (15,16). Despite the few studies so far conducted on the identification and description of MPRs in CBCT, this radiographic appearance can mimic certain jaw lesions such as paradental cysts, pericoronitis, Stafne cysts, pathological periapical inflammation, and pathological dental follicles. In this study, the specific objective is to investigate the prevalence and characteristics of MPRs observed on CBCT images, focusing on identifying distinguishing features and associations that may have clinical relevance. This is guided by the hypothesis that MPRs could be predictive of certain anatomical or clinical conditions, potentially informing diagnostic approaches.
Materials and Methods
In this cross-sectional study, 235 CBCT radiographs were evaluated to assess the prevalence and characteristics of periradicular radiolucency around the mandibular third molar (MPRs) in patients who visited an oral and maxillofacial radiology center in Zanjan in 2023. The sample size of 235 CBCT images was chosen based on preliminary assessments to ensure a statistically meaningful analysis. Further, a power analysis was conducted, confirming that this sample size was sufficient for identifying statistically significant patterns in the context of MPR prevalence and characteristics (9).
These radiographs were obtained for various clinical indications. Patients with advanced bone resorption, paradental cysts, or pathological changes were excluded to prevent potential confounding factors that could bias the study outcomes toward these specific pathologies. Demographic information regarding the age and gender of the patients was collected from the medical history taken at the time of CBCT imaging. All images were captured using a New Tom 3G CBCT scanner (Quantitative Radiology, Verona, Italy; 6-inch FOV, 0.25 mm voxel size, 10.65 mA, and 84 kVp).
The images were observed by an oral and maxillofacial radiologist on a 20-inch monitor (LG, Seoul, Korea) in a semidark room for the presence of MPRs, the presence of MPRs on one or both sides, the positioning of the third molar, its relationship to the mandibular canal, and thinning of the cortical margins. They were also checked for the position of MPRs relative to the mandibular canal and the third molar, the relationship to the root apex, the presence of surrounding bone swelling, and root resorption of the mandibular third molar (Figure 1).
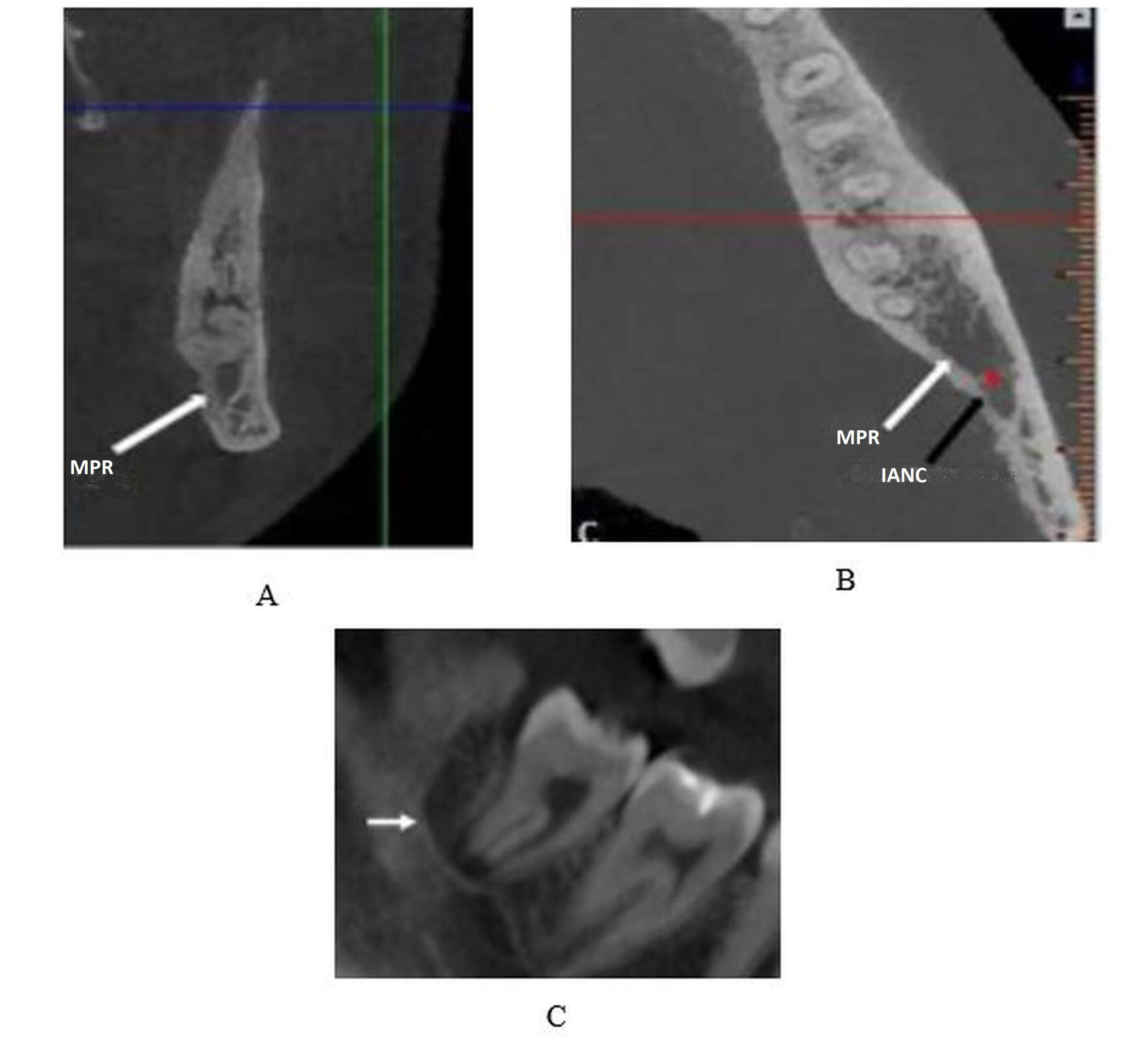
Figure 1.
Cross-sectional (A), Axial (B), and Panoramic-Like (C) Cone-Beam Computed Tomography Scans Showing an Oval Homogeneous Hypodense Structure on the Distal of the Third Mandibular Molar
.
Cross-sectional (A), Axial (B), and Panoramic-Like (C) Cone-Beam Computed Tomography Scans Showing an Oval Homogeneous Hypodense Structure on the Distal of the Third Mandibular Molar
The radiologists evaluated the images in the axial, coronal, and sagittal planes by scrolling the mouse and assessed the cross-sectional images with a slice thickness of 1 mm and intervals of 2 mm. The observers were allowed to adjust the density and contrast of the images and to use a magnification tool. For intra-observer reliability, one radiologist re-evaluated the images two weeks later.
This information was documented in a checklist. The data were analyzed using SPSS software, version 22. The weighted κ coefficient was also calculated to determine the level of intra-observer agreement. The chi-square test was employed to determine the association between the prevalence of MPRs and qualitative nominal (e.g., gender) and continuous quantitative (e.g., age) variables. A significance level of P < 0.05 was considered statistically significant in this study.
The chi-square test assumptions were thoroughly verified before analysis. Additionally, effect sizes and confidence intervals were calculated alongside P values to provide a clearer understanding of the findings’ clinical implications.
Results
For intra-observer reliability, one radiologist re-evaluated the images two weeks later. The weighted kappa coefficient was 0.93, showing perfect agreement.
The CBCT radiographic images of 235 individuals, including 141 females (60%) and 94 males (40%) with an age range of 16–81 years (mean age 33.4 years), were examined in this study. The prevalence of MPRs in the CBCT images was 23 cases, of which 17 (73.9%) were female and 6 (26.1%) were male. The Chi-square test was used to assess the association between gender and the prevalence of MPRs. The results indicated that there was no significant relationship between the prevalence of MPRs and gender (P = 0.15, Table 1).
Table 1.
Prevalence of MPRs Based on Gender
|
|
|
Without MPRs
|
With MPRs
|
Significance Level
|
| Gender, No. (%) |
Female |
124(58.5) |
17 (73.9) |
0.15 |
| Male |
77 (41.5) |
6 (26.1) |
| Total, No. (%) |
212 (100) |
23 (100) |
|
Note. MPR: Mandibular third molar.
Out of the 23 MPRs observed in CBCT images, 14 (60.9%) were round, and 9 (39.1%) were oval. Six (69.6%) MPRs were unilateral, while 7 (30.4%) were bilateral. Out of the 23 cases of MPRs detected in CBCT images, 13 (56.5%), 7 (30.4%), and 3 (13%) involved the mandibular third molar in distoangular, mesioangular, and vertical positions, respectively (Table 2).
Table 2.
Characteristics and Position of MPRs
|
Characteristics and Position
|
Number (%)
|
Total
|
| Shape |
Round |
14 (60.9) |
23 (100) |
| Oval |
9 (39.1) |
| Position |
Unilateral |
16 (69.6) |
23 (100) |
| Bilateral |
7 (30.4) |
| The position of the mandibular third molar |
Distoangular |
13 (56.5) |
23 (100) |
| Mesioangular |
7 (30.4) |
| Vertical |
3 (13) |
Note. MPR: Mandibular third molar.
Out of the 23 cases of MPRs observed in CBCT images, 11 (47.8%) were in contact with the mandibular canal, 18 (78.3%) showed thinning of cortical margins, and 10 (43.5%) were associated with the root apex. No bone expansion or root resorption was observed in any of the cases (Table 3).
Table 3.
Association of MPRs With Adjacent Anatomical Structures
|
|
Number (%)
|
Total
|
| Contact with the mandibular canal |
Yes |
11 (47.8) |
23 (100) |
| No |
12 (52.2) |
| Thinning of cortical margins |
Yes |
18 (78.3) |
23 (100) |
| No |
5 (21.7) |
| Association with the root apex |
Yes |
10 (43.5) |
23 (100) |
| No |
13 (56.5) |
| Bone expansion/root resorption |
Yes |
0 (0) |
23 (100) |
| No |
23 (100) |
Note. MPR: Mandibular third molar.
Discussion
Radiolucencies adjacent to the mandibular third molar with a vital pulp, which are not of endodontic origin, are part of normal anatomical structures. Therefore, it is crucial for dentists to distinguish between MPRs and pathologies associated with the mandibular third molar, as patients with pathological lesions may require advanced imaging or surgical procedures (17). In this study, 235 CBCT images were reviewed to determine the prevalence and characteristics of MPRs. Out of the 235 CBCT images examined, 23 demonstrated MPRs, resulting in an MPR prevalence of 9.8%, which is consistent with the results of previous studies. However, in the study performed by Ahire et al, this rate was reported as 14.5%. This difference could be due to variations in imaging methods, as the present study used CBCT imaging, which is more accurate than panoramic radiography (8,12,16). Of the 23 CBCTs with MPRs, 17 belonged to females while 6 belonged to males; however, there was no significant association between the prevalence of MPRs and gender. Currently, studies on mandibular MPRs generally demonstrate no statistically significant gender-based differences in their prevalence. While such data may suggest minor variations in occurrence between genders, most findings highlight the lack of statistical significance, reinforcing the idea that gender is not a major factor influencing MPRs. These observations are crucial for understanding the characteristics of MPRs and their differentiation from pathological lesions (2,3). In this study, 56.52% of MPRs were associated with distoangular impacted third molars, which aligns with the findings of previous studies (3,14,15). However, in a study by Yalcin and Artas, the highest prevalence of MPRs was found in vertically impacted third molars (4). This difference could be due to the use of various classification methods for third molar positioning.
About 52.2% of MPRs did not contact the inferior alveolar canal, which is in line with the findings of Yalcin and Artas. However, in the study by Kapila et al, panoramic images showed that MPRs contacted the inferior alveolar canal in 59.52% of cases. This discrepancy may be attributed to differences in imaging techniques and the higher accuracy of CBCT in determining the relationship of MPRs with surrounding anatomical structures (4,18). In 73.9% of cases, MPRs were positioned distobuccally relative to the third molar, which is consistent with the results of Sekerci et al and Nascimento et al (3,15). Ahire et al, studying panoramic images, noted that MPRs were most often positioned distally relative to the third molar, attributed to the limitations of panoramic radiography in determining the bucco-lingual positioning of structures (9). In the present study, in more than half of the cases, MPRs were not connected to the root apex, and no bone swelling was observed around the MPRs, which conforms to the findings of previous studies (2,3,15). As demonstrated in our study and previous investigations, MPRs are not pathologic because they do not cause bone expansion or root resorption. MPRs do not usually affect the lamina dura or the PDL space. It is believed that MPRs are spontaneously resolved after tooth extraction since MPRs are not detected on radiographs of patients with extracted third molars. Cortical margin thinning around MPRs in mandibular third molars was documented in 78.3% of cases in this study, consistent with the results of previous research (15,17). Khojastepour et al reported that the lingual cortex was perforated in 75% of MPR cases (11). This discrepancy may stem from different classification methods for estimating the thickness of the lingual plate in the above study. Based on previous studies, CBCT is considered the preferred method for examining odontogenic cysts and other mandibular lesions. In panoramic images, the radiolucent area behind the third molar can be misleading due to density differences caused by the opacity of the tooth compared to the surrounding bone, potentially resulting in visual errors that may lead observers to misinterpret the radiolucent area as MPRs. However, such visual errors are not present in CT and CBCT images (1). This study’s limitations include its cross-sectional nature and potential observer bias in assessing CBCT images, which could influence the findings. Additionally, the study findings were compared with both supportive and contrasting literature to contextualize the results and highlight areas for further research.
Conclusion
Dental clinicians must be acquainted with radiolucencies adjacent to mandibular third molars in order to differentiate them from the common pathological lesions in this region and avoid unnecessary surgical procedures.
Acknowledgments
We would like to extend our sincere gratitude to Dr. Shahram Arsang Jang for their invaluable guidance and support throughout this study.
Competing Interests
The authors do not have any financial interest in the companies whose materials were included in this study.
Ethical Issues
This study was approved by the Ethics Committee of Zanjan University of Medical Sciences, Zanjan, Iran (IR.ZUMS.REC.1400.276).
Funding
Self funded. This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Bohay RN, Mara TW, Sawula KW, Lapointe HJ. A preliminary radiographic study of mandibular para-radicular third molar radiolucencies. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004; 98(1):97-101. doi: 10.1016/j.tripleo.2004.02.083 [Crossref] [ Google Scholar]
- Bağcı N, Pamukcu U, Toprak M, Peker İ. Awareness-knowledge level and practice of two dentistry specialties dentists regarding juxta-apical radiolucency. J Stomatol 2024; 77(1):55-62. doi: 10.5114/jos.2024.136151 [Crossref] [ Google Scholar]
- Sekerci AE, Sahman H, Kutalmış Buyuk S, Sisman Y, Demirbuga S. Cone beam computed tomography appearance of mandibular para-radicular third molar radiolucencies: prevalence, characteristics and a review of the literature. Int Res J Basic Clin Stud 2015; 3(1):29-34. doi: 10.14303/irjbcs.2014.050 [Crossref] [ Google Scholar]
- Yalcin ED, Artas A. Juxta-apical radiolucency and relations with surrounding structures on cone-beam computed tomography. Br J Oral Maxillofac Surg 2020; 58(3):309-13. doi: 10.1016/j.bjoms.2019.12.004 [Crossref] [ Google Scholar]
- Neville BW, Damm DD, Allen CM, Chi AC. Oral and Maxillofacial Pathology-E-Book. Elsevier Health Sciences; 2015.
- Mallya S, Lam E. White and Pharoah’s Oral Radiology E-Book: Principles and Interpretation: Second South Asia Edition E-Book. India: Elsevier Health Sciences; 2019.
- Al-Khateeb TH, Bataineh AB. Pathology associated with impacted mandibular third molars in a group of Jordanians. J Oral Maxillofac Surg 2006; 64(11):1598-602. doi: 10.1016/j.joms.2005.11.102 [Crossref] [ Google Scholar]
- Miloro M, Ghali GE, Larsen PE, Waite PD. Peterson’s Principles of Oral and Maxillofacial Surgery. London: BC Decker; 2004.
- Ahire BS, Bhoosreddy AR, Bhoosreddy S, Shinde MR, Pandharbale AA, Kunte VR. Radiographic assessment of agenesis, impaction, and pararadicular radiolucencies in relation with third molar in Nashik city of Maharashtra. J Dent Allied Sci 2016; 5(1):3-6. doi: 10.4103/2277-4696.185185 [Crossref] [ Google Scholar]
- Harada N, Vasudeva SB, Joshi R, Seki K, Araki K, Matsuda Y. Correlation between panoramic radiographic signs and high‐risk anatomical factors for impacted mandibular third molars. Oral Surg 2013; 6(3):129-36. doi: 10.1111/ors.12025 [Crossref] [ Google Scholar]
- Khojastepour L, Ghasemi M, Rasti S, Hasani M. Evaluation of juxta-apical radiolucency as a risk factor for inferior alveolar nerve damage: a cone-beam computed tomography (CBCT) study. Shiraz E Med J 2020; 21(10):e93330. doi: 10.5812/semj.93330 [Crossref] [ Google Scholar]
- Hasani M, Razavi N, Haghnegahdar A, Zarifi M. Evaluating the presence of paresthesia in patients with juxta-apical radiolucency after third molar surgery: a case-control study. Rea Sq [Preprint]. February 22, 2021. Available from: https://www.researchsquare.com/article/rs-220280/v1.
- Gilvetti C, Haria S, Gulati A. Is juxta-apical radiolucency a reliable risk factor for injury to the inferior alveolar nerve during removal of lower third molars?. Br J Oral Maxillofac Surg 2019; 57(5):430-4. doi: 10.1016/j.bjoms.2018.11.022 [Crossref] [ Google Scholar]
- Şallı GA, Özcan İ, Pekiner FN. Prevalence of pneumatization of the articular eminence and glenoid fossa viewed on cone-beam computed tomography examinations in a Turkish sample. Oral Radiol 2020; 36(1):40-6. doi: 10.1007/s11282-019-00378-1 [Crossref] [ Google Scholar]
- Nascimento EH, Costa Oenning AC, Freire BB, Gaêta-Araujo H, Haiter-Neto F, Freitas DQ. Comparison of panoramic radiography and cone beam CT in the assessment of juxta-apical radiolucency-an answer to Letter to Editor. Dentomaxillofac Radiol 2018; 47(8):20180246. doi: 10.1259/dmfr.20180246 [Crossref] [ Google Scholar]
- Dalton J, Mahoney M, Savage N. Computed tomography appearance of mandibular para-radicular third molar radiolucencies. Dentomaxillofac Radiol 2011; 40(1):47-52. doi: 10.1259/dmfr/16606307 [Crossref] [ Google Scholar]
- Salemi F, Foroozandeh M, Mirzaee M, Farhadian M, Makateb P, Mostafapour M. Appearance of mandibular para-radicular third molar radiolucencies on cone-beam computed tomography. Contemp Clin Dent 2021; 12(2):128-32. doi: 10.4103/ccd.ccd_156_20 [Crossref] [ Google Scholar]
- Kapila R, Harada N, Araki K, Sano T, Goto TK. Evaluation of juxta-apical radiolucency in cone beam CT images. Dentomaxillofac Radiol 2014; 43(5):20130402. doi: 10.1259/dmfr.20130402 [Crossref] [ Google Scholar]