Avicenna J Dent Res. 17(1):21-26.
doi: 10.34172/ajdr.1931
Original Article
Dysplastic Change Rate in Cases of Actinic Cheilitis: A Retrospective Study of 33 Cases
Soussan Irani Conceptualization, Data curation, Methodology, Writing – original draft, Writing – review & editing, 1, 2, * 
Hamidreza Ghasemi Basir Data curation, Methodology, Writing – review & editing, 3
Iman Habibi Investigation, Writing – review & editing, 4
Author information:
1Oral Pathology Department, Dental Faculty, Dental Research Center, Hamadan University of Medical Sciences, Hamadan, Iran
2Adjunct Senior Lecturer in the School of Medicine and Dentistry, Griffith University, Gold Coast, Q4222, Australia
3Pathology Department, Sina Hospital, Hamadan University of Medical Sciences, Hamadan, Iran
4Oral Pathology Department, Dental Faculty, Hamadan University of Medical Sciences,Hamadan,Iran
Abstract
Background: Chronic lip inflammation is the characteristic feature of actinic cheilitis (AC), a precancerous lesion that can develop into squamous cell carcinoma (SCC). Early detection and education of individuals at higher risk for AC can reduce the likelihood of developing SCC. This retrospective study sought to assess the demographic and clinicopathological attributes of 33 patients diagnosed with AC.
Methods: Thirty-three cases were retrieved from the archive of the Department of Pathology of Sina Hospital, Hamadan, Iran, between 2009 and 2019. All information was recorded from the submission forms, including gender, age, anatomical location of the lesions, size, duration, outdoor occupation, and clinical aspects.
Results: There were 29 males and 4 females. The mean age was 62±14 years. Nine cases of older patients (>62 years) showed mild, moderate, and severe grades of dysplasia (3 cases for each degree). Fisher’s exact test indicated a significant difference between the presence of dysplasia and the age of the patients (P<0.001). In addition, a statistically significant distinction emerged concerning the presence of dysplasia and the size of the lesion (Fisher’s exact test, P<0.001). Likewise, a significant difference was found between the presence of dysplasia and the type of occupation regarding exposure to the sun (P<0.001). Finally, there was a significant difference between the presence of dysplasia and the duration of the disease (Fisher’s exact test, P<0.003).
Conclusion: The clinicopathologic profile observed in the series of patients with AC revealed that patients were more frequently males, aged≤62 years. The predominant clinical features were erythematous and atrophic lesions. However, in cases with dysplasia, ulceration emerged as the most frequent clinical finding. Further research with larger sample sizes is imperative to explore the potential role of smoking and other environmental factors in the development of AC and its potential malignant transformation.
Keywords: Actinic cheilitis, Dysplasia, Lip neoplasms, Precancerous conditions
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Irani S, Ghasemi Basir H, Habibi I. Dysplastic change rate in cases of actinic cheilitis: a retrospective study of 33 cases. Avicenna J Dent Res. 2025;17(1):21-26. doi:10.34172/ajdr.1931
Background
Chronic lip inflammation is the characteristic feature of actinic cheilitis (AC), a precancerous lesion that can develop into squamous cell carcinoma (SCC) (1). The primary causal factor is believed to be prolonged exposure to solar ultraviolet radiation, especially ultraviolet B. SCC development has also been linked to tobacco use and/or alcohol consumption (2). AC has a variety of clinical symptoms, such as swelling, erythematous or white patches, ulcers, crusts, atrophy, pallor, and/or scaly lesions, in addition to dryness (3). On histological examination, the epithelium shows atrophy or hyperplasia, hyperkeratosis, and different grades of dysplasia. Furthermore, an amorphous, basophilic substance known as solar elastosis may be evident in the underlying connective tissue. Malignancy can occur in 3.07%–16.9% of AC cases, according to earlier investigations (4). Early detection and education of individuals at higher risk for AC can reduce the likelihood of developing SCC (1). SCC on the lips has a four times higher metastatic rate than cutaneous SCC (4). The importance of this lesion and its timely diagnosis is highlighted by these findings. This retrospective study seeks to assess the demographic and clinicopathological attributes of 33 patients diagnosed with AC.
Materials and Methods
This was a cross-sectional, retrospective study based on the analysis of the pathology records of patients diagnosed with AC. Thirty-three cases were retrieved from the archive of the Department of Pathology of Sina Hospital, Hamadan, Iran, between 2009 and 2019. All information was recorded from the submission forms, including age (in years), gender, anatomical location of the lesions, size (greatest diameter of the lesion in millimeters), outdoor occupation, duration, and clinical aspects. To validate the prior diagnosis rendered by an anatomical pathologist, an oral and maxillofacial pathologist conducted a comprehensive review of all microscopic slides, meticulously documenting histological attributes. The grading of epithelial dysplasia followed the World Health Organization classification (2017), encompassing categories such as no dysplasia, mild dysplasia, moderate dysplasia, and severe dysplasia (5,6). Statistical analyses were performed employing both Chi-square and Fischer’s exact tests to establish associations. Additionally, the correlation among variables was assessed utilizing Spearman’s test. Statistical significance was determined by a P value less than 0.05 (P ≤ 0.05).
Results
There were 29 males and 4 females. The mean age was 62 years (ranging from 35 to 96 years). Tables 1 and 2 provide details on the demographic and clinical characteristics of 33 cases, respectively.
Table 1.
Demographic Data of 33 Patients With Actinic Cheilitis
|
Clinical Parameters
|
No. (%)
|
| Gender |
|
| All patients |
|
| Male |
29 (87.9) |
| Female |
4 (12.1) |
| Total |
33 |
| Gender |
|
| Cases with dysplasia |
|
| Male |
18 (90) |
| Female |
2 (10) |
| Total |
20 |
| Gender |
|
| Cases without dysplasia |
|
| Male |
11 (84.6) |
| Female |
2 (15.4) |
| Total |
13 |
| Age (y) |
|
| All patients |
|
| Mean age ± SD (range) |
62 ± 14 (35-96) |
| ≤ 62 |
17 (51.5) |
| > 62 |
16 (48.5) |
| Age (y) |
|
| Cases with dysplasia |
|
| ≤ 62 |
11 (55) |
| > 62 |
9 (45) |
| Age (y) |
|
| Cases without dysplasia |
|
| ≤ 62 |
6 (46.1) |
| > 62 |
7 (53.9) |
| Size (mm) |
|
| All patients |
|
| Mean (range) |
6.8 (3-25) |
| ≤ 6.8 |
25 (75.5) |
| > 6.8 |
8 (24.5) |
| Size (mm) |
|
| Cases with dysplasia |
|
| ≤ 6.8 |
14 (70) |
| > 6.8 |
6 (30) |
| Size (mm) |
|
| Cases without dysplasia |
|
| ≤ 6.8 |
11 (84.6) |
| > 6.8 |
2 (15.4) |
| Duration (month) |
|
| All patients |
|
| Mean (range) |
8.5 (1-24) |
| ≤ 8.5 |
17 (51.5) |
| > 8.5 |
16 (48.5) |
| Duration (month) |
|
| Cases with dysplasia |
|
| ≤ 8.5 |
6 (30) |
| > 8.5 |
14 (70) |
| Duration (month) |
|
| Cases without dysplasia |
|
| ≤ 8.5 |
11 (84.6) |
| > 8.5 |
2 (15.4) |
| Outdoor occupation |
|
| All patients |
|
| Yes |
25 (75.7) |
| No |
8 (24.3) |
| Outdoor occupation |
|
| Cases with dysplasia |
|
| Yes |
15 (75) |
| No |
5 (25) |
| Outdoor occupation |
|
| Cases without dysplasia |
|
| Yes |
10 (76.9) |
| No |
3 (23.1 |
| Affected area |
|
| All patients |
|
| Lower lip |
30 (90.9) |
| Upper lip |
3 (9.1) |
| Affected area |
|
| Cases with dysplasia |
|
| Lower lip |
17 (85) |
| Upper lip |
3 (15) |
| Affected area |
|
| Cases without dysplasia |
|
| Lower lip |
13 (100) |
| Upper lip |
0 |
Note. SD: Standard deviation.
Table 2.
Number (%) of Prominent Clinical Presentations of 33 Cases of Actinic Cheilitis and Duration of Lesions
|
Clinical Presentations
|
No. (%)
|
No. of Cases With Duration<8.5 Months
|
No. of Cases With Duration>8.5 Months
|
| All patients |
|
|
|
| White plaques |
11 (33.3) |
4 |
7 |
| Ulceration |
10 (30.3) |
5 |
5 |
| Scaly lesions |
4 (12.1) |
2 |
2 |
| Erythematous and atrophic lesions |
3 (9) |
3 |
0 |
| Areas of pallor |
2 (6) |
2 |
0 |
| Dryness |
2 (6) |
1 |
1 |
| Blurred demarcation of the vermilion border and skin |
1 (3) |
0 |
1 |
| Cases with dysplasia |
|
|
|
| Ulceration |
9 (45) |
4 |
5 |
| White plaques |
8 (40) |
2 |
6 |
| Scaly lesions |
2 (10) |
0 |
2 |
| Blurred demarcation of the vermilion border and skin |
1 (5) |
0 |
1 |
| Areas of pallor |
0 (0) |
0 |
0 |
| Dryness |
0 (0) |
0 |
0 |
| Erythematous and atrophic lesions |
0 (0) |
0 |
0 |
| Cases without dysplasia |
|
|
|
| White plaques |
3 (23.1) |
2 |
1 |
| Erythematous and atrophic lesions |
3 (23.1) |
3 |
0 |
| Scaly lesions |
2 (15.4) |
2 |
0 |
| Areas of pallor |
2 (15.4) |
2 |
0 |
| Dryness |
2 (15.4) |
1 |
1 |
| Ulceration |
1 (7.6) |
1 |
0 |
| Blurred demarcation of the vermilion border and skin |
0 (0) |
0 |
0 |
Nine cases of older patients ( > 62 years) showed mild, moderate, and severe grades of dysplasia (3 cases for each degree). Histologic findings of 33 cases of AC are reported in Table 3.
Table 3.
Histological Findings of 33 Cases of Actinic Cheilitis With or Without Dysplasia
|
Histologic Grading
|
No. (%)
|
Histologic Findings According to the Criteria Used for Diagnosing Dysplasia
|
| Without dysplasia |
13 (39.4) |
Hyperplasia or atrophy, hyperkeratosis, mild inflammatory cell infiltrate, and elastosis (basophilic appearance of underlying connective tissue) |
| Mild dysplasia |
4 (12.1) |
Hyperplasia, hyperkeratosis, and dysplastic changes limited principally to the basal and parabasal layers: Basal cell hyperplasia, loss of basal cell polarity, irregular epithelial stratification, and drop-shaped rete ridges. Basophilic appearance of underlying connective tissue, angiogenesis and vasodilatation, and mild inflammatory cell infiltrate |
| Moderate dysplasia |
6 (18.2) |
Hyperplasia, hyperkeratosis, and dysplastic changes from the basal layer to the midportion of the epithelium: Basal cell hyperplasia, loss of basal cell polarity, irregular epithelial stratification, drop-shaped rete ridges, increased number of mitotic figures, abnormally superficial mitosis, cell and nuclear pleomorphism, hyperchromatism, increasing nuclear, and cytoplasmic ratio. Basophilic appearance of underlying connective tissue, angiogenesis and vasodilatation, and moderate inflammatory cell infiltrate |
| Severe dysplasia |
10 (30.2) |
Hyperplasia, hyperkeratosis, or a thin layer of keratin, and dysplasia changes can be observed from the basal layer to a level above the midpoint of the epithelium: Basal cell hyperplasia, loss of basal cell polarity, irregular epithelial stratification, dyskeratosis, drop-shaped rete ridges, increased number of mitotic figures, abnormally superficial mitosis, increased number and size of nucleoli, and hyperchromatism. Basophilic appearance of underlying connective tissue, angiogenesis and vasodilation, and moderate to severe inflammatory cell infiltrate |
The results of Fisher’s exact test demonstrated a significant difference between the presence of dysplasia and the age of the patients (P < 0.001). In addition, a statistically significant distinction was found concerning the presence of dysplasia and the size of the lesion (Fisher’s exact test, P < 0.001). Similarly, there was a significant difference between the type of occupation regarding exposure to the sun and the presence of dysplasia (P < 0.001). Further, a significant difference was observed between the presence of dysplasia and the duration of the disease (Fisher’s exact test, P < 0.003).
The literature was searched for previous case series. The detailed information of previous studies is provided in Table 4.
Table 4.
Previous Studies on the Clinicopathological Profile of Actinic Cheilitis
|
Gender
|
Age (Years)
|
Most Common Clinical Feature (%)
|
Histological Findings
|
Reference
|
M (81.3%)
F (18.7%) |
62
61.2 |
No data |
Dysplasia: Mild (52%), moderate (23%), severe (12.5%), carcinoma in situ (11.2%), and SCC (1.3%) |
(7) |
M (60; 92.3%)
F (5; 7.4%) |
53.2
51.4 |
Erosion and ulcer (47.7%) |
Dysplasia: Mild: 18 (27.7%), moderate: 20 (30.8%), severe: 16 (24.6%), and SCC: 11 (16.9%) |
(8) |
| M (72.41%) |
75.86% > 40 |
Dryness 29 (100%) |
Dysplasia: Mild (10.34%), moderate (27.59%), and severe (62.07%) |
(9) |
| No data |
No data |
Dryness (100%) |
Dysplasia (100%) |
(10) |
M (30; 75%)
F (10; 25%) |
Overall: 80% ≥ 40, 20% < 40 |
White lesions (55%) |
Without dysplasia (40%): Mild (25%), moderate (27.5%), and severe (7.5%) |
(11) |
M (128; 79.5%)
F (33; 20.5%) |
77.5% ≥ 40
22.5% < 40 |
White lesions (33.6%) |
High risk (39.8%) and low risk (60.2%) |
(12) |
| M (55; 80.9%) |
53.1 |
No data |
Without dysplasia (23.5%): Mild (30.9%), moderate (35.3%), and severe (10.3%) |
(13) |
M (43; 67.2%)
F (21; 32.8%) |
55.1
61.6 |
Loss of mucocutaneous limit (100%) |
Dysplasia: Mild (13.6%), moderate (28.8%), and severe (57.6%) |
(14) |
M (29; 80.6%)
F (7; 19.45) |
Overall:
94.4% ≥ 40, 5.6% < 40 |
Blurred demarcation between lip and skin (88.95) |
Without dysplasia (19.4%), mild (55.6%), moderate (16.7%), and severe (8.3%) |
(15) |
Note. F: Female; M: Male; SCC: Squamous cell carcinoma.
Discussion
AC occurs mainly on the lower lip and is often found in fair-skinned males (1,15). Chronic exposure to ultraviolet radiation is the main risk factor for its development (16). Based on our findings (Table 1), the majority of patients (87.9%) were males, and the lower lip was the primary site of lesions (90.9%). According to a study (16), AC lesions are most prevalent in females (55% vs. 44.6%). The use of lipstick or lip sunscreen may be the reason for the low incidence of AC in women. The majority of outdoor jobs are dominated by males, and men tend to retire later than women. This observation supports the proposed idea that the lower lip, because it is everted, is more susceptible to chronic and direct sunlight exposure than the upper lip. This vulnerability could be attributed to the lower lip’s thinner epithelium, which lacks the robust keratin layer found in the skin (17). The vermilion region of the lip is characterized by its unique characteristics, indicating a reduced presence or absence of the stratum corneum compared to the skin (18).
In agreement with the findings of a prior study, our results demonstrated more dysplastic changes in patients ≤ 62 years old, and there was a significant association between the presence of dysplasia and the age groups (11). However, in a previously published paper, the presence of dysplasia was not related to the age of the patient (9).
In the current series, “white plaque” was the most common clinical presentation (33.3%). Our results are in line with those of a prior paper, showing white plaques (33.6%) as the most frequent clinical feature (11,12). Conversely, loss of lip vermilion delineation was the most prevalent clinical presentation (77.1%) in some previous studies (14,19). Another study reported “dryness” as the most common clinical feature (9). These differences between the findings might be related to the clinical features of AC at the time of diagnosis and biopsy.
In our study series, the most prevalent clinical manifestation observed in cases with dysplasia was ulceration, followed by the presence of white plaques. This finding conforms to the results of the research conducted by Medeiros et al, where ulcers were identified in 100% of patients with moderate to severe cases. Interestingly, white plaques were documented in only 15.4% of individuals with moderate to severe conditions in their study (15). The progression of AC has been postulated to involve the development of focal chronic ulceration over time. Moreover, a prior study indicated a potential correlation between the consumption of pipes or cigarettes and the occurrence of ulcers. This study proposed that repetitive trauma stemming from these habits could potentially predispose the affected area to malignant transformation (20).
Concerning histologic classification, 42.4% of cases in our study showed some degree of dysplasia, and 18.2% of samples demonstrated SCC (18.2%) (Figure 1A-I). Kaugars et al found epithelial dysplasia in 98.7% of the cases. Further, they observed mild epithelial dysplasia and SCC in 52.0% and 1.3% of patients, respectively (7). Markopoulos et al reported mild epithelial dysplasia in 27.7%, while 72.3% showed moderate dysplasia to invasive SCC (8). De Santana Sarmento et al found mild, moderate, and severe dysplasia in 10.34%, 27.59%, and 62.07% of patients, respectively (10). In another study performed by Gonzaga et al, 76.5% of cases were graded as mild, moderate, and severe dysplasia (13). Additionally, Medeiros et al classified 55.6%, 16.7%, and 8.3% of samples as mild, moderate, and severe dysplasia, respectively (15). The variations observed among studies could stem from differences in the histological and cytological parameters considered during the assessment of epithelial dysplasia. In addition, these differences may reflect a delay in diagnosis at each center. Furthermore, in the early stages, some patients might erroneously attribute the lesion to aging, subsequently dismissing it until it progresses to a more advanced state.
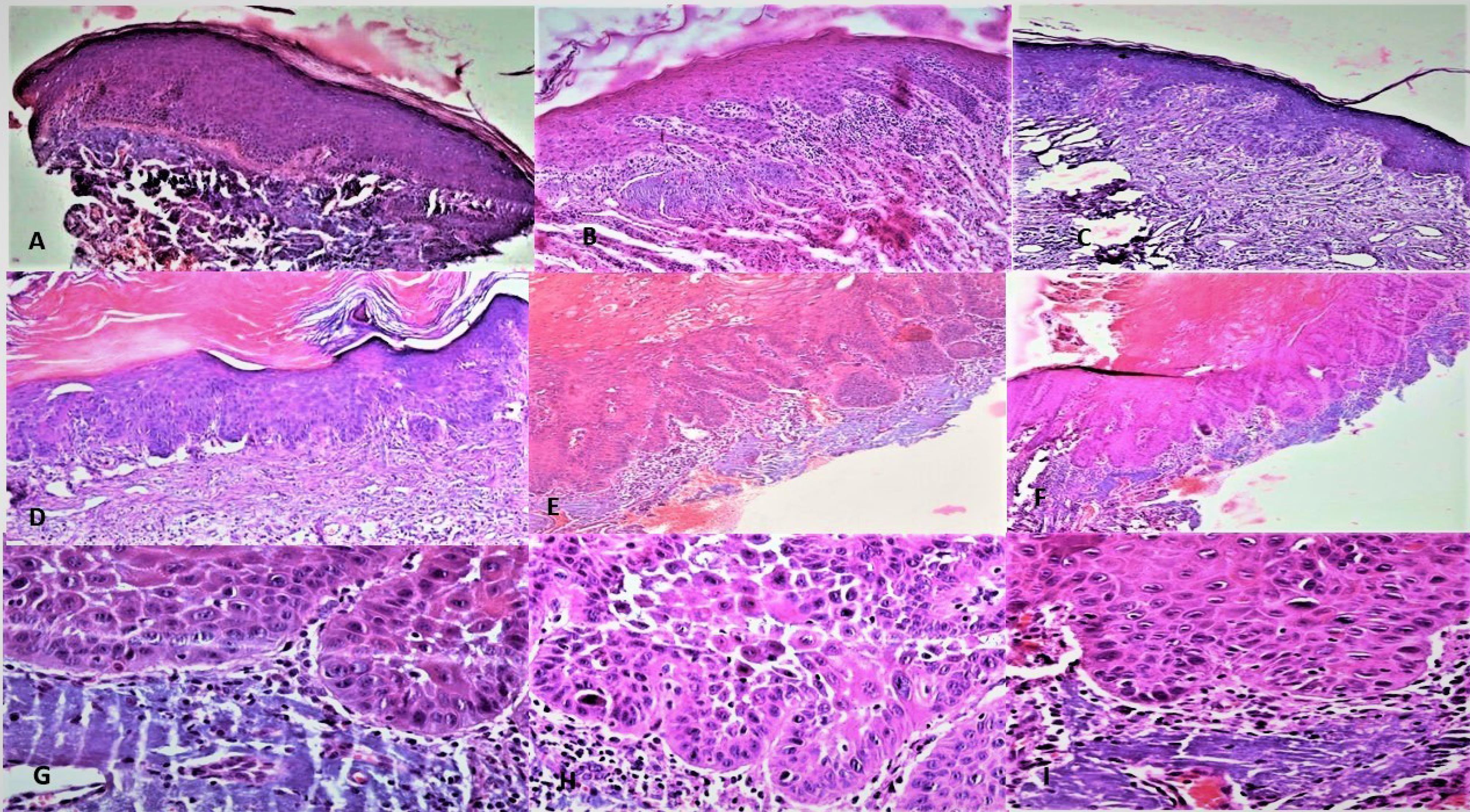
Figure 1.
Histopathological Images Showing Biopsies From Actinic Cheilitis Lesions: (A) Without Dysplasia (X100), (B) Mild Dysplasia and Epithelial Hyperplasia (X100), (C) Mild Dysplasia and Epithelial Atrophy (X100), (D) Moderate Dysplasia and Hyperkeratosis (X100), (E) Severe Dysplasia (X250), (F) Severe Dysplasia (X100), (G) Cellular Atypia (X400), (H) Dyskeratosis and Loss of Epithelial Cell Cohesion (X400), and (I) Cells With Hyperchromatic and Pleomorphic Nuclei (X400). Note. Notice solar elastosis in images
.
Histopathological Images Showing Biopsies From Actinic Cheilitis Lesions: (A) Without Dysplasia (X100), (B) Mild Dysplasia and Epithelial Hyperplasia (X100), (C) Mild Dysplasia and Epithelial Atrophy (X100), (D) Moderate Dysplasia and Hyperkeratosis (X100), (E) Severe Dysplasia (X250), (F) Severe Dysplasia (X100), (G) Cellular Atypia (X400), (H) Dyskeratosis and Loss of Epithelial Cell Cohesion (X400), and (I) Cells With Hyperchromatic and Pleomorphic Nuclei (X400). Note. Notice solar elastosis in images
Within the scope of our current study, a noteworthy correlation emerged between the presence of dysplasia and the duration of the condition. This observation lends credence to the notion that the passage of time plays a substantive role in the progression of AC toward epithelial dysplasia. Given the profound influence that dysplastic changes exert on the potential malignant transformation of pre-cancerous lesions, it is imperative to ascertain the presence and extent of epithelial dysplasia within the sampled specimens. It has been proposed that the first phase of epithelial dysplasia is the damage to the basal cell layer. Later, continued exposure to the sun and other environmental factors can cause acanthosis and hyperkeratosis. The severity of dysplasia is associated with acanthosis, hyperkeratosis, basophilic change of the connective tissue, perivascular inflammation, and inflammation within the connective tissue. The role of inflammation and inflammatory cells in malignant transformation has been documented in prior studies. For example, neutrophils promote cancer development through extracellular matrix remodeling, angiogenesis, promotion of cell migration and invasion, and proliferation of cancer cells (21,22).
Given the substantial propensity of AC to progress into invasive SCC, the early identification of AC significantly enhances the prospects of successful intervention. Notably, reported rates of malignant transformation in AC range from 10% to 30%. Remarkably, a striking 95% of SCC cases affecting the lower lip stem from preexisting AC. Moreover, SCC originating in the lower lip exhibits heightened aggressiveness and an elevated risk of metastasis in contrast to SCC arising on the skin (23,24). Over the past few decades, diverse therapeutic modalities have been explored to manage AC. These encompass procedures such as vermilionectomy, cryotherapy, and topical applications such as imiquimod and 5-fluorouracil (4). In recent times, photodynamic therapy has emerged as a promising avenue for AC treatment. Encouragingly, a comprehensive clinical response has been documented in 68.9% of cases subjected to photodynamic therapy (4,24).
Conclusion
The clinicopathologic profile observed in this study series of patients with AC confirmed that patients were more frequently males aged ≤ 62 years. Erythematous and atrophic lesions were predominant clinical features. However, in cases with dysplasia, ulceration has emerged as the most frequent clinical finding. This suggests a potential role of inflammation in malignant transformation. The results underscore the necessity of educational intervention strategies aimed at raising awareness about the etiology of AC. Nonetheless, this study has certain limitations, particularly the absence of a comprehensive history of smoking in medical records. Accordingly, further research with larger sample sizes is imperative to explore the potential role of smoking and other environmental factors in the development of AC and its potential malignant transformation.
Acknowledgements
The authors would like to thank the Vice-Chancellor for Research and Technology of Hamadan University of Medical Sciences.
Competing Interests
The authors declare that they have no conflict of interests.
Ethical Approval
This study received ethical approval from the Ethics Committee of Hamadan University of Medical Sciences (approval No. IR.UMSHA.REC.1398.043).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
- Irani S. Pre-cancerous lesions in the oral and maxillofacial region: a literature review with special focus on etiopathogenesis. Iran J Pathol 2016; 11(4):303-22. [ Google Scholar]
- Mello FW, Melo G, Modolo F, Rivero ER. Actinic cheilitis and lip squamous cell carcinoma: Literature review and new data from Brazil. J Clin Exp Dent 2019; 11(1):e62-9. doi: 10.4317/jced.55133 [Crossref] [ Google Scholar]
- Warnakulasuriya S, Kujan O, Aguirre-Urizar JM, Bagan JV, González-Moles M, Kerr AR. Oral potentially malignant disorders: a consensus report from an international seminar on nomenclature and classification, convened by the WHO Collaborating Centre for Oral Cancer. Oral Dis 2021; 27(8):1862-80. doi: 10.1111/odi.13704 [Crossref] [ Google Scholar]
- Trager MH, Farmer K, Ulrich C, Basset-Seguin N, Herms F, Geskin LJ. Actinic cheilitis: a systematic review of treatment options. J Eur Acad Dermatol Venereol 2021; 35(4):815-23. doi: 10.1111/jdv.16995 [Crossref] [ Google Scholar]
- El-Naggar AK, Chan JK, Rubin Grandis J, Slootweg PJ. WHO Classification of Head and Neck Tumours. 4th ed. Lyon: International Agency for Research on Cancer; 2017. p. 105.
- Ranganathan K, Kavitha L. Oral epithelial dysplasia: classifications and clinical relevance in risk assessment of oral potentially malignant disorders. J Oral Maxillofac Pathol 2019; 23(1):19-27. doi: 10.4103/jomfp.JOMFP_13_19 [Crossref] [ Google Scholar]
- Kaugars GE, Pillion T, Svirsky JA, Page DG, Burns JC, Abbey LM. Actinic cheilitis: a review of 152 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999; 88(2):181-6. doi: 10.1016/s1079-2104(99)70115-0 [Crossref] [ Google Scholar]
- Markopoulos A, Albanidou-Farmaki E, Kayavis I. Actinic cheilitis: clinical and pathologic characteristics in 65 cases. Oral Dis 2004; 10(4):212-6. doi: 10.1111/j.1601-0825.2004.01004.x [Crossref] [ Google Scholar]
- Cavalcante AS, Anbinder AL, Carvalho YR. Actinic cheilitis: clinical and histological features. J Oral Maxillofac Surg 2008; 66(3):498-503. doi: 10.1016/j.joms.2006.09.016 [Crossref] [ Google Scholar]
- Savage NW, McKay C, Faulkner C. Actinic cheilitis in dental practice. Aust Dent J 2010; 55 Suppl 1:78-84. doi: 10.1111/j.1834-7819.2010.01202.x [Crossref] [ Google Scholar]
- de Santana Sarmento DJ, da Costa Miguel MC, Queiroz LM, Godoy GP, da Silveira EJ. Actinic cheilitis: clinicopathologic profile and association with degree of dysplasia. Int J Dermatol 2014; 53(4):466-72. doi: 10.1111/ijd.12332 [Crossref] [ Google Scholar]
- de Sousa Lopes ML, da Silva Júnior FL, Lima KC, de Oliveira PT, da Silveira ÉJ. Clinicopathological profile and management of 161 cases of actinic cheilitis. An Bras Dermatol 2015; 90(4):505-12. doi: 10.1590/abd1806-4841.20153848 [Crossref] [ Google Scholar]
- Gonzaga AK, Mafra RP, da Silva LP, de Almeida Freitas R, de Souza LB, Pinto LP. Actinic cheilitis: Morphometric parameters and its relationship with the degree of epithelial dysplasia. Acta Histochem 2020; 122(1):151452. doi: 10.1016/j.acthis.2019.151452 [Crossref] [ Google Scholar]
- de Castro Abrantes T, Fonsêca TC, Cabral MG, Agostini M, Benevenuto de Andrade BA, Romañach MJ. Epithelial dysplasia in actinic cheilitis: microscopic study of 70 cases from Brazil. Head Neck Pathol 2021; 15(2):566-71. doi: 10.1007/s12105-020-01250-z [Crossref] [ Google Scholar]
- Medeiros CK, Lopes ML, Silveira É J, Lima KC, Oliveira PT. Actinic cheilitis: proposal of a clinical index. Med Oral Patol Oral Cir Bucal 2022; 27(4):e310-8. doi: 10.4317/medoral.25243 [Crossref] [ Google Scholar]
- Rodriguez-Archilla A, Irfan-Bhatti A. Risk factors for actinic cheilitis: a meta-analysis. J Dent Res Dent Clin Dent Prospects 2021; 15(4):285-9. doi: 10.34172/joddd.2021.047 [Crossref] [ Google Scholar]
- Nicolau SG, Baelus L. Chronic actinic cheilitis and cancer of the lower lip. Br J Dermatol 1964; 76:278-89. doi: 10.1111/j.1365-2133.1964.tb14529.x [Crossref] [ Google Scholar]
- Saxena S, Pankaj AK, Panwar S, Rani A, Chopra J, Rani A. Histological changes at the commissure of the lip on approaching from its cutaneous to the mucosa region in males. Natl J Maxillofac Surg 2021; 12(1):88-92. doi: 10.4103/njms.NJMS_15_20 [Crossref] [ Google Scholar]
- Moreira P, Assaf AV, Cortellazzi KL, Takahama Junior A, Azevedo RS. Social and behavioural associated factors of actinic cheilitis in rural workers. Oral Dis 2021; 27(4):911-8. doi: 10.1111/odi.13610 [Crossref] [ Google Scholar]
- Poitevin NA, Rodrigues MS, Weigert KL, Macedo CL, Dos Santos RB. Actinic cheilitis: proposition and reproducibility of a clinical criterion. BDJ Open 2017; 3:17016. doi: 10.1038/bdjopen.2017.16 [Crossref] [ Google Scholar]
- Irani S. Metastasis to head and neck area: a 16-year retrospective study. Am J Otolaryngol 2011; 32(1):24-7. doi: 10.1016/j.amjoto.2009.09.006 [Crossref] [ Google Scholar]
- Irani S, Dehghan A. Expression of vascular endothelial-cadherin in mucoepidermoid carcinoma: role in cancer development. J Int Soc Prev Community Dent 2017; 7(6):301-7. doi: 10.4103/jispcd.JISPCD_323_17 [Crossref] [ Google Scholar]
- Bakirtzi K, Papadimitriou I, Andreadis D, Sotiriou E. Treatment options and post-treatment malignant transformation rate of actinic cheilitis: a systematic review. Cancers (Basel) 2021; 13(13):3354. doi: 10.3390/cancers13133354 [Crossref] [ Google Scholar]
- Vasilovici A, Ungureanu L, Grigore L, Cojocaru E, Şenilă S. Actinic cheilitis - from risk factors to therapy. Front Med (Lausanne) 2022; 9:805425. doi: 10.3389/fmed.2022.805425 [Crossref] [ Google Scholar]