Avicenna J Dent Res. 16(4):197-204.
doi: 10.34172/ajdr.1886
Original Article
Comparative Evaluation of Canal Transportation and Centering Ability of ProTaper Next, NeoNiTi, and R-Motion by CBCT Analysis in the Curved Root Canals of Permanent Mandibular First Molar: An In Vitro Study
D. Praveen 1  , Tashmeem Mohammad 1, * , Kalyan Satish R 1 , Kaladhar Amarapu 1 , K. Durga Prasad 1 , Saikiran Bonu 2
, Tashmeem Mohammad 1, * , Kalyan Satish R 1 , Kaladhar Amarapu 1 , K. Durga Prasad 1 , Saikiran Bonu 2
Author information:
1Department of Conservative Dentistry and Endodontics, Vishnu Dental College and Hospital, Bhimavaram, Andhra Pradesh, India – 534201
2Vishnu Dental College and Hospital, Bhimavaram, Andhra Pradesh, India – 534201
Abstract
Background: The success of root canal therapy hinges on various factors, with biomechanical preparation standing out as a crucial step. Equally significant is the meticulous preservation of the canal’s natural shape, as any deviation from it can lead to complications such as canal aberrations or transportation. The aim of the study was to evaluate the canal transportation and canal centering ability of ProTaper Next (PTN), NeoNiTi, and R-Motion (RM) file systems using cone-beam computed tomography (CBCT).
Methods: Thirty human mandibular molar roots with an angle of curvature between 10° and 20° were chosen into three groups of ten samples each from the pool of collected samples that met the inclusion and exclusion criteria, including PTN (group I), NeoNiTi (group II), and RM file systems (group III). To achieve reproducibility of pre- and post-operative CBCT scans and to ease instrumentation, the tooth was placed in a template created using silicon impression material. Using CBCT software, pre- and post-instrumentation pictures were obtained from the apex at three different levels (3 mm, 6 mm, and 9 mm). One-way analysis of variance and post hoc analysis were used to evaluate the amount of transportation and centering ability.
Results: RM demonstrated better canal centering ability than PTN and NeoNiTi at 3 mm and 6 mm, but there was no statistically significant difference in canal transportation between the three groups at levels of 3 mm, 6 mm, and 9 mm from the apex.
Conclusion: PTN, NeoNiTi, and RM all exhibited similar behaviour under the study’s in-vitro conditions in terms of canal transportation and centering ability. However, the RM group outperformed the other systems in terms of both canal transportation and centering ability, with NeoNiTi and PTN systems coming in second and third, respectively.
Keywords: Canal transportation, Canal centering ability, Cone-beam computed tomography, PTN, RM
Copyright and License Information
© 2024 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Praveen D, Mohammad T, Satish RK, Amarapu K, Prasad KD, Bonu S. Comparative evaluation of canal transportation and centering ability of protaper next, neoniti, and r-motion by cbct analysis in the curved root canals of permanent mandibular first molar: an in vitro study. Avicenna J Dent Res. 2024; 16(4):197-204. doi:10.34172/ajdr.1886
Background
As a cornerstone of endodontic therapy, root canal treatment focuses on removing bacteria and debris from the dentin and carefully preparing the canals (1). Root canal instrumentation, a pivotal step in root canal treatment, involves intricate mechanical processes, employing irrigants and medicaments to effectively shape canals. The success of subsequent treatment phases hinges on the precision of this step. It might be difficult to prepare a root canal most effectively, especially in curved canals where there is a greater possibility of procedural errors such as canal transportation (2). Instrumentation is greatly hampered by canal transportation, iatrogenic deviance from the original canal course, especially in curved canals. The incidence of transportation varies across different root canal levels, with the apical region being more susceptible. Various factors, including root canal anatomy complexity, instrumentation techniques, and operator skill, contribute to the occurrence of transportation (3). The prevalence of traditional stainless-steel instruments is hindered by their limited flexibility, often resulting in iatrogenic complications. The field of root canal preparation experienced a historic shift with the development of nickel-titanium (NiTi) instruments, which are distinguished by special features such as shape memory and super flexibility (4). Furthermore, the application of novel techniques guaranteed the continued preservation of the original canal geometry by utilizing a more accurate, centrally aligned rotary file system. The introduction of these systems into endodontics signifies a crucial advancement, aiming at enhancing the efficiency of canal instrumentation, resulting in a faster and more accessible process.
Continuous rotary systems, such as the ProTaper Next (PTN) from Dentsply Maillefer, have been in use for the past 25 years and fall into the category of fifth-generation rotary shaping file systems. Unlike previous rotating NiTi instruments, PTN uses a wave-like mechanism of motion, is distinguished by its offset axis of mass and rotation, and aims to reduce transportation. Utilizing M-Wire technology for enhanced flexibility and cyclic fatigue resistance, PTN features an asymmetric design with advantages such as efficient debris removal coronally and high resistance to cyclic fatigue. It is comprised of five files, namely, X1 (17/0.04), X2 - (25/0.06), X3 - (30/0.07), X4 - (40/0.06), and X5 - (50/0.06). Taper lock and the screw effect can be prevented using varying percentage tapers, which decrease the degree of friction between a file and dentin (5). Research indicates that PTN, in comparison to other file systems such as WaveOne (Dentsply Maillefer), BT-Race (FKG), and ProTaper Universal (Dentsply Maillefer), is linked to lower levels of debris extrusion and less canal transportation (6).
Through the use of wire-cut electrical discharge machining, the NeoNiTi (Orikam) rotary file system is developed with outstanding surface finishing, low residual stresses, and great precision. The system comprises two main components, namely, the orifice opener (NeoNiTi C1) and the single shaping file system (NeoNiTi A1), available in yellow (20/6%), red (25/6%), and black (30/4%) tapers. They are designed with a rectangular cross-section, providing enhanced cutting edges, an abrasive surface, and progressive flexibility (7).
Recently, the development of NiTi alloys and endodontic torque control motors has led to a resurgence of interest in reciprocating motion. The balanced force approach (Roane et al., 1985) gave rise to the idea of reciprocation, which enables hand devices to shape even highly curved canals into larger apical diameters (8). The R-Motion (RM) file system is a recent introduction in endodontics. Because of their smaller core sizes, these file systems are more versatile in design and have optimized file tips and rounded triangular cross-sections with keen cutting edges. The unique design of RM files minimizes the screwing effect, allowing clinicians to maintain higher control efficiency during root canal instrumentation. The files, titled RM G (15/0.03), RM 25 (25/0.06), RM 30 (30/0.04), RM 40 (40/0.04), and RM 50 (50/0.04), show alternate percentage tapers. RM files undergo heating treatment between 32 degrees and 35 degrees Celsius, during which they go through a phase change from martensite to austenite (9).
Considering that there is no literature available on Canal Transportation and Centering Ability comparing NeoNiTi and RM. Accordingly, this study explores two innovative NiTi rotary systems, NeoNiti (continuous rotation) and RM (reciprocation), comparing their shaping abilities, specifically focusing on canal transportation and centering ability in curved root canals. The well-established PTN serves as a benchmark for comparison. Utilizing CBCT, this research seeks to evaluate the anatomical changes in root canals before and after instrumentation. The null hypothesis posits no significant differences among the evaluated NiTi rotary systems for the analyzed parameters.
Materials and Methods
The Institutional Research Committee granted ethical clearance for the study (No. IECVDC/23/PG01/CE/IVT/92).
Sample Size Calculation
A prior study (10) with a P value of less than 0.05 and G*Power software with 80% confidence was the basis for calculating sample size. After calculations, a minimum of 10 teeth were included in each group.
Sample Selection and Methodology
After approval by the Institutional Review Board, 30 intact human permanent mandibular molars, extracted for periodontal reasons, were collected one month prior to the commencement of the study. They included mesiobuccal canals with fully developed apices that had an angle of curvature between 10° and 20° as per the Schneider approach (11) and a minimum length of 19 mm, as selecting this range ensures a focus on canals that present a realistic challenge in clinical practice. Extreme curvatures (either very high or very low) might not represent typical cases encountered by practitioners. The length of 19 mm ensures that the samples are representative of the average size of human teeth and allows for the application of standard endodontic tools and methods. Before being used, every tooth was cleansed, sanitized, and kept in saline at 4 °C. Teeth with immature teeth, fractures, pathological root resorptions, calcifications, or any prior endodontic therapy were eliminated from the investigation. Fractures were clinically evaluated by utilizing the dental operating microscope with 12x magnification. Every single specimen was calibrated to have a length of 13 mm. Calculating the length of the root canal involved advancing a 10-K-file (Mani, Japan) into the canal until it reached the tip of the apex and then deducting 0.5 mm. The specimens were inserted into putty blocks to achieve constant location and divided into three groups (Figure 1A).
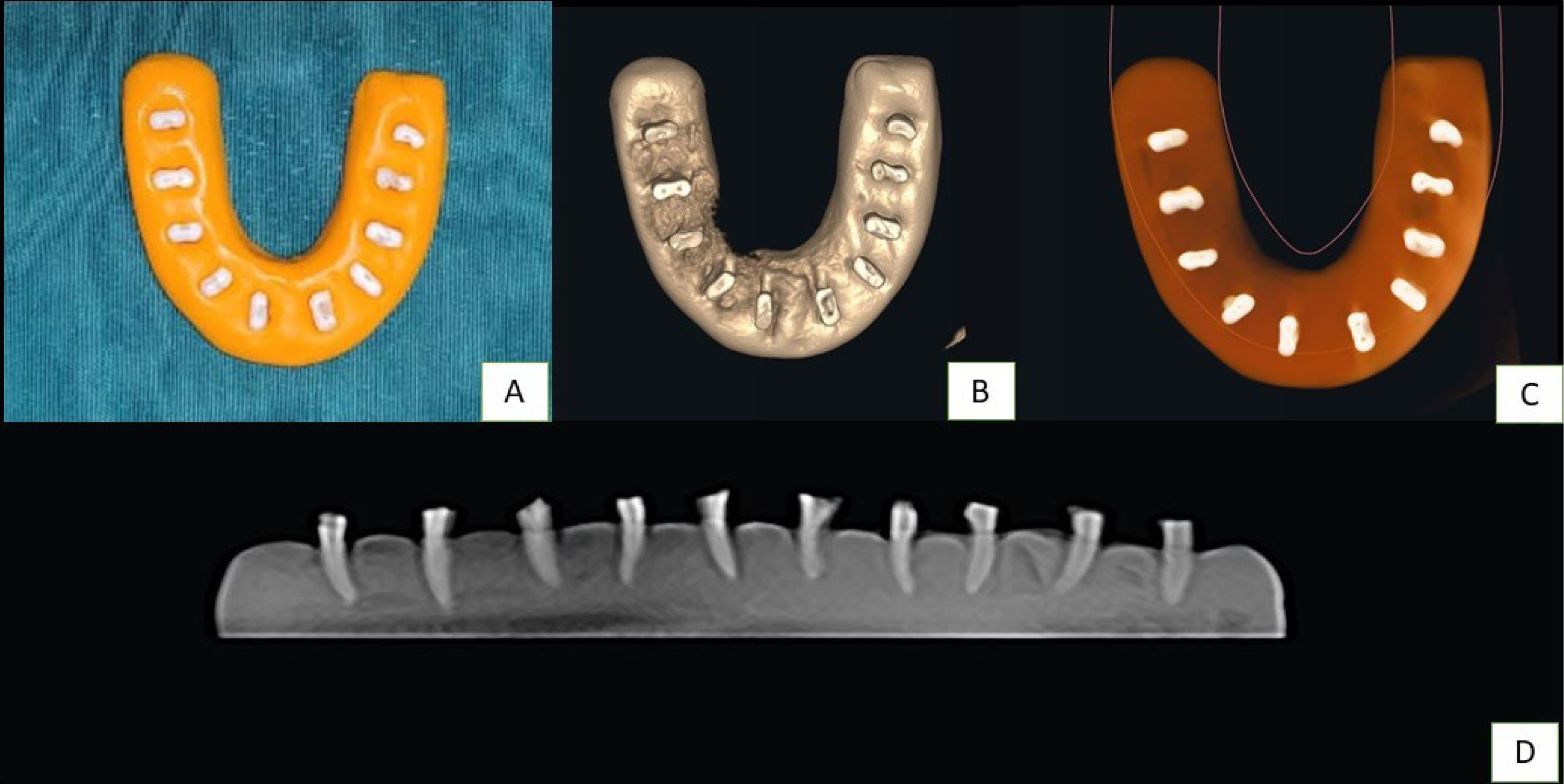
Figure 1.
(A) Samples Stabilized with Silicon Impression Mould, (B-C) Preoperative CBCT Scanning Modalities With Various Filters, and (D) CBCT Scanning of the Samples in Longitudinal Section. Note. CBCT: Cone-beam computed tomography
.
(A) Samples Stabilized with Silicon Impression Mould, (B-C) Preoperative CBCT Scanning Modalities With Various Filters, and (D) CBCT Scanning of the Samples in Longitudinal Section. Note. CBCT: Cone-beam computed tomography
Initial Scanning
To align the occlusal plane of the chin support with the plate, the template is fitted horizontally. Every tooth requires a pre-CBCT scan performed before it is instrumented. To analyze pre- and post-instrumentation data later on using DICOM software, the images were stored on the hard drive of the computer, and 3.0 seconds of exposure were conducted at 2.0 mA and 75 kV (Figure 1B-D).
Final Root Canal Preparation
Initial scans were conducted prior to the instrumentation in each group.
-
Group 1: Canals were shaped with the PTN rotary file system (Dentsply Sirona Ballaigues, Switzerland). The PTN-SX file works as an orifice modifier, and then X1- (17/0.04) and X2- (25/0.06) are used till reaching the working length. Following each instrumentation, irrigation and recapitulation were performed using a 10-K file.
-
Group 2: NeoNiTi (Neolix, Chatres-La-Foret, France) rotary files were employed to sculpt the canals. A sequence of NeoNiTi A1 (20/0.06) and NeoNiTi A1 (25/0.06) and the NeoNiTi C1 orifice modifier are utilized, respectively. With a torque of 4 Ncm and a rotational pace of 300 rpm, files were used in a brushing action. Similar to Group 1, irrigation and recapitulation were performed in this group.
-
Group 3: The RM (FKG Dentaire SA, La Chaux de Fonds, Switzerland) was employed to shape the canals. RM Glider (15/0.03) and RM 25 (25/0.06) were utilized, respectively. With a torque of 4 Ncm and a rotational speed of 500 rpm, files were utilized in a brushing action. Similar to Group 1, irrigation and recapitulation were conducted in this group. All tools and methods used in this study followed the manufacturer’s guidelines. Biomechanical preparation was performed using the appropriate files. The final irrigation was conducted using 0.9% normal saline, 17% ethylenediaminetetraacetic acid, and 3% sodium hypochlorite solution (NaOCl).
Final Scanning and Evaluations
The samples underwent postoperative CBCT scanning using consistent parameters. Pre-instrumentation data were saved, and using CBCT software (Kodak 9000 DICOM Software CS 9000 3D), a comparative analysis was performed with post-instrumentation data (1). Each specimen was illustrated by three axial tomograms (apical third, middle third, and cervical third), which were obtained at the root apex at 3 mm, 6 mm, and 9 mm, respectively.
Evaluation of Canal Transportation
The shortest stretch from the margin of the pre-instrumented canal and the outermost aspect of the root on the mesial and distal aspects was estimated, and the findings were compared with the same measurements created from the instrumented images (Figure 2) (12).This allowed for the determination of the amount of canal transportation using the formula presented by Gambill et al (14).
-
(a1− a2) − (b1− b2)
-
(c1− c2) − (d1− d2)
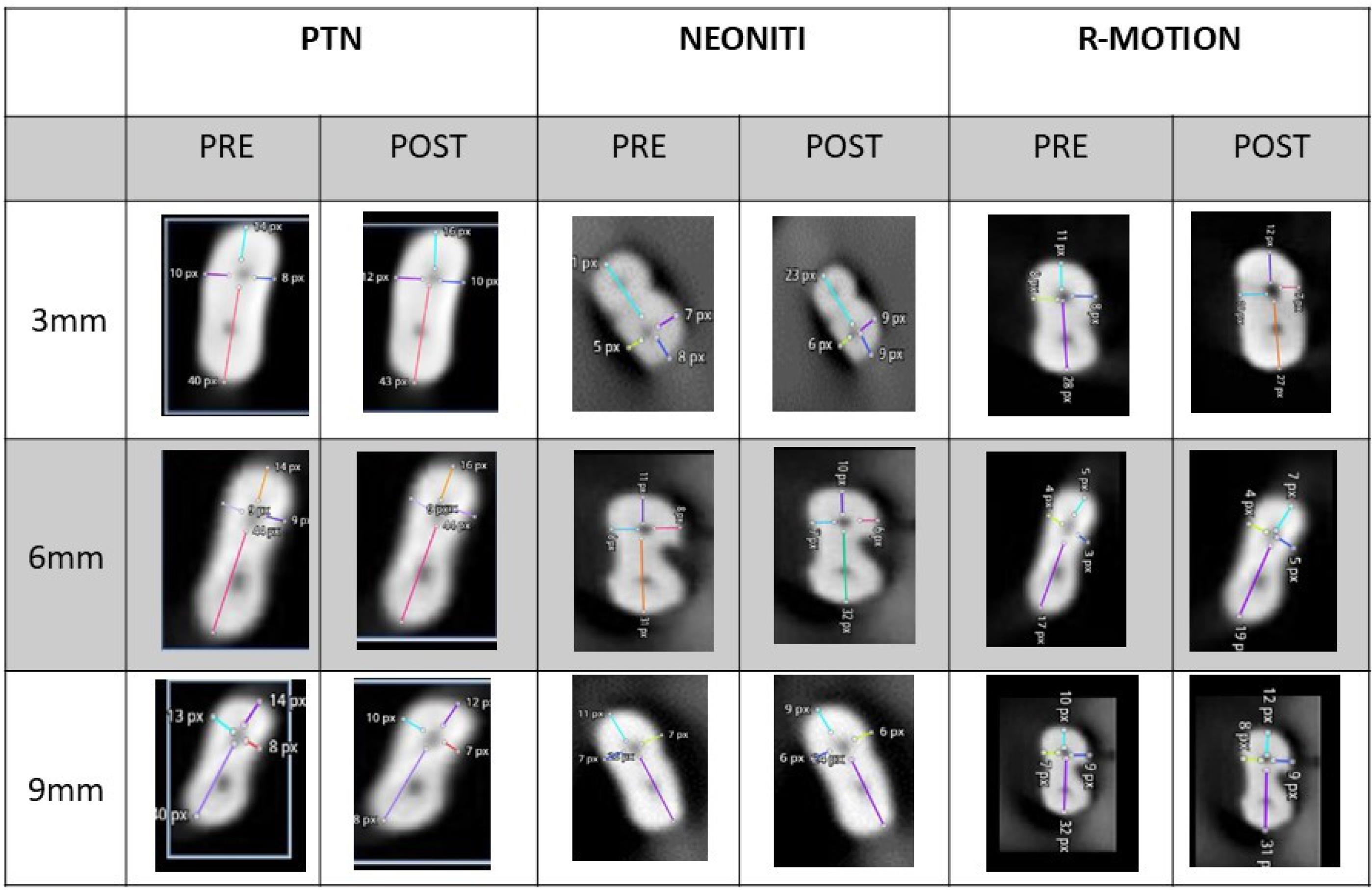
Figure 2.
Pre- and Post-operative CBCT Images for Assessing Canal Transportation. Note. CBCT: Cone-beam computed tomography
.
Pre- and Post-operative CBCT Images for Assessing Canal Transportation. Note. CBCT: Cone-beam computed tomography
Before Instrumentation
a1: The shortest path between the root’s mesial boundaries and the canal
b1: The shortest path between the canal and the distal limits of the root
c1: The shortest path between the canal and the buccal borders of the root
d1: The shortest path between the canal and the lingual borders
After instrumentation
a2: The shortest path between the mesial margins of the root and the canal
b2: The shortest path between the distal boundaries of the root and the canal
c2: The shortest path between the canal and the buccal borders
d2: The shortest path between the canal and the lingual borders
The results of these calculations point out that 0 denotes no canal transportation.
Evaluation of Canal Centering Ability
The ratio (A1 – A2)/(B1 – B2) or (B1 – B2)/(A1 – A2) is used to calculate canal centering ability. A score of one in this formula represents perfect centering. Pre- and post-operative CBCT images for canal centering ability were evaluated using the mentioned formula (Figure 3).
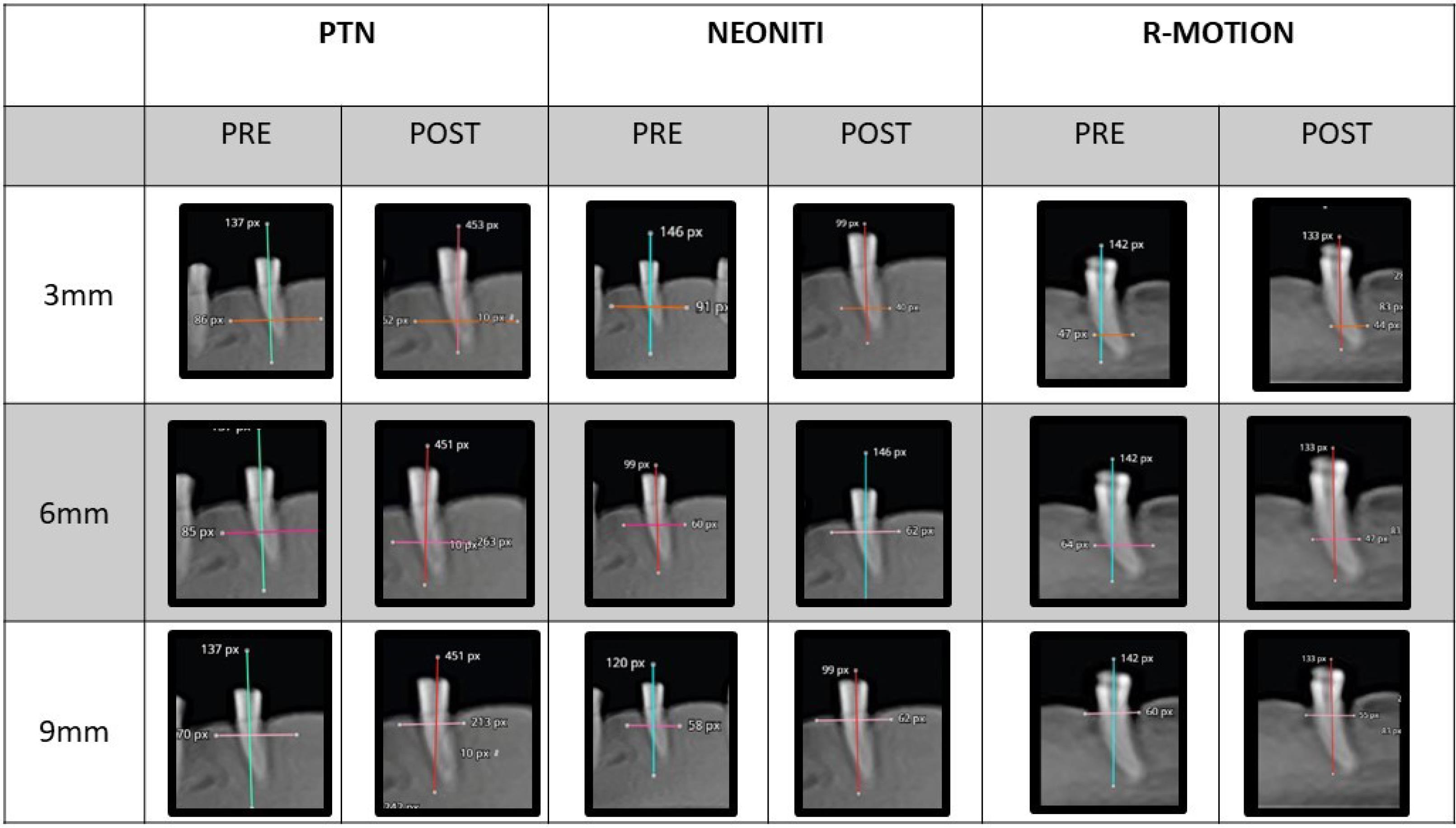
Figure 3.
Pre- and Post-operative CBCT Images for Canal Centring Ability. Note. CBCT: Cone-beam computed tomography
.
Pre- and Post-operative CBCT Images for Canal Centring Ability. Note. CBCT: Cone-beam computed tomography
Statistical Analysis
The obtained data were analyzed using SPSS (Statistical Package for Social Sciences) version 20 software. The confidence interval was set at 95%, and the P value was set at 0.05. Any value equal to or less than was considered to be significant. Canal transportation was assessed using the Kruskal-Wallis test, followed by Tukey’s post hoc test. Centering ability was evaluated using a one-way analysis of variance, followed by Tukey’s post hoc test.
Results
Canal Transportation
The results in Table 1 demonstrate the means ± standard deviations (SD) of canal transportation at 3 distinct apex levels (3 mm, 6 mm, and 9 mm) among the PTN, NeoNiTi, and RM groups. Group I exhibited mean transportation of 0.1 ± 0.18, 0.03 ± 0.24, and - 0.05 ± 0.21 at 3 mm, 6 mm, and 9 mm, respectively, from the apex. For group II, the mean transportation was 0.6 ± 0.17, 0.1 ± 0.11, and - 0.02 ± 0.13 mm at 3 mm, 6 mm, and 9 mm, respectively. At 3 mm, 6 mm, and 9 mm apical region, the mean transportation of Group III was 0.0 ± 0.06, -0.01 ± 0.05, and 0.02 ± 0.12, respectively. No statistically significant difference was detected among these groups for canal transportation at 3 mm, 6 mm, and 9 mm (P > 0.05, Figure 4).
Table 1.
Comparison of Canal Transportation at 3 mm, 6 mm, and 9 mm Among ProTaper Next, NeoNiTi, and R-Motion Groups
|
|
Mean and SD
|
F-value
|
P
-value
|
| 3 mm |
| Group 1 |
0.1 ± 0.18 |
1.132 |
0.337 |
| Group 2 |
0.6 ± 0.17 |
| Group 3 |
0.0 ± 0.06 |
| 6 mm |
| Group 1 |
0.03 ± 0.24 |
0.164 |
0.850 |
| Group 2 |
0.1 ± 0.11 |
| Group 3 |
-0.01 ± 0.05 |
| 9 mm |
| Group 1 |
- 0.05 ± 0.21 |
0.464 |
0.633 |
| Group 2 |
- 0.02 ± 0.13 |
| Group 3 |
0.02 ± 0.12 |
Note. SD: Standard deviation.
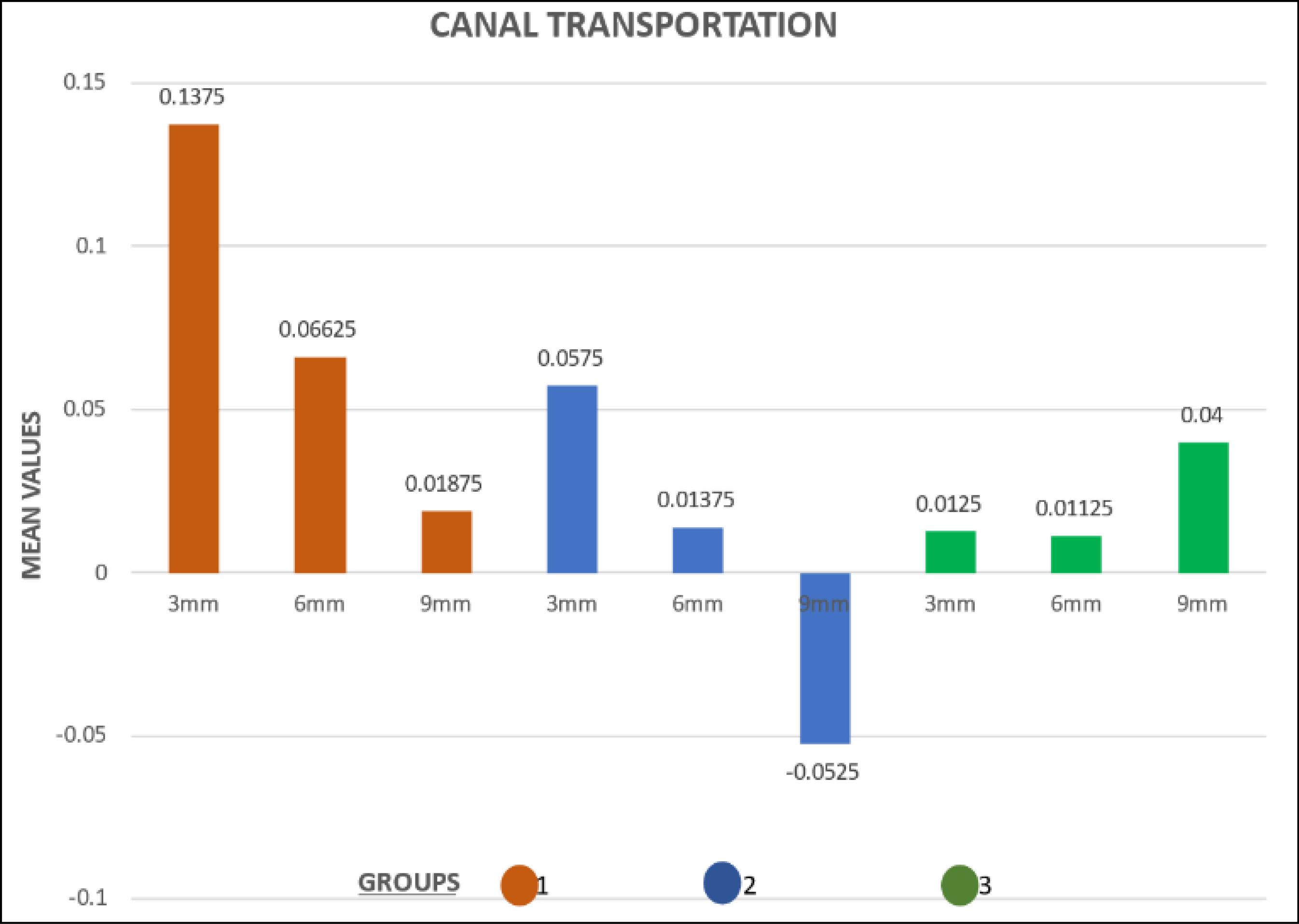
Figure 4.
Comparison of Canal Transportation at 3 mm, 6 mm, and 9 mm
.
Comparison of Canal Transportation at 3 mm, 6 mm, and 9 mm
Canal Centering Ability
Table 2 presents mean and SD values of the canal centering ability at 3 distinct apex levels (3 mm, 6 mm, and 9 mm) among the PTN, NeoNiTi, and RM groups. Group I represented the mean centering ability of 1.64 ± 0.98, 1.37 ± 0.86, and 0.65 ± 0.32 at 3 mm, 6 mm, and 9 mm, respectively, from the apex. For group II, the mean centering ability was 1.5 ± 1.2, 1.48 ± 0.78, and 1.0 ± 0.40 at 3 mm, 6 mm, and 9 mm, respectively. Group III demonstrated mean centering ability of 1.1 ± 0.5, 1.0 ± 0.4, and 1.2 ± 0.83 at 3 mm, 6 mm, and 9 mm, respectively, from the apex. There was a significant difference among the groups (P > 0.05) at 9 mm. No statistically significant difference was observed among these groups at 3 mm and 6 mm (P > 0.05, Figure 5).
Table 2.
Comparison of Canal Centering Ability at 3 mm, 6 mm, and 9 mm Among ProTaper Next, NeoNiTi, and R-Motion Groups
|
|
Mean and SD
|
Test-value
|
P
-value
|
| 3 mm |
| Group 1 |
1.64 ± 0.98 |
0.915 |
0.412 |
| Group 2 |
1.5 ± 1.2 |
| Group 3 |
1.1 ± 0.51 |
| 6 mm |
| Group 1 |
1.37 ± 0.86 |
1.214 |
0.305 |
| Group 2 |
1.48 ± 0.78 |
| Group 3 |
1.0 ± 0.40 |
| 9 mm |
| Group 1 |
0.65 ± 0.32 |
2.740 |
0.083 |
| Group 2 |
1.12 ± 0.63 |
| Group 3 |
1.2 ± 0.83 |
Note. SD: Standard deviation.
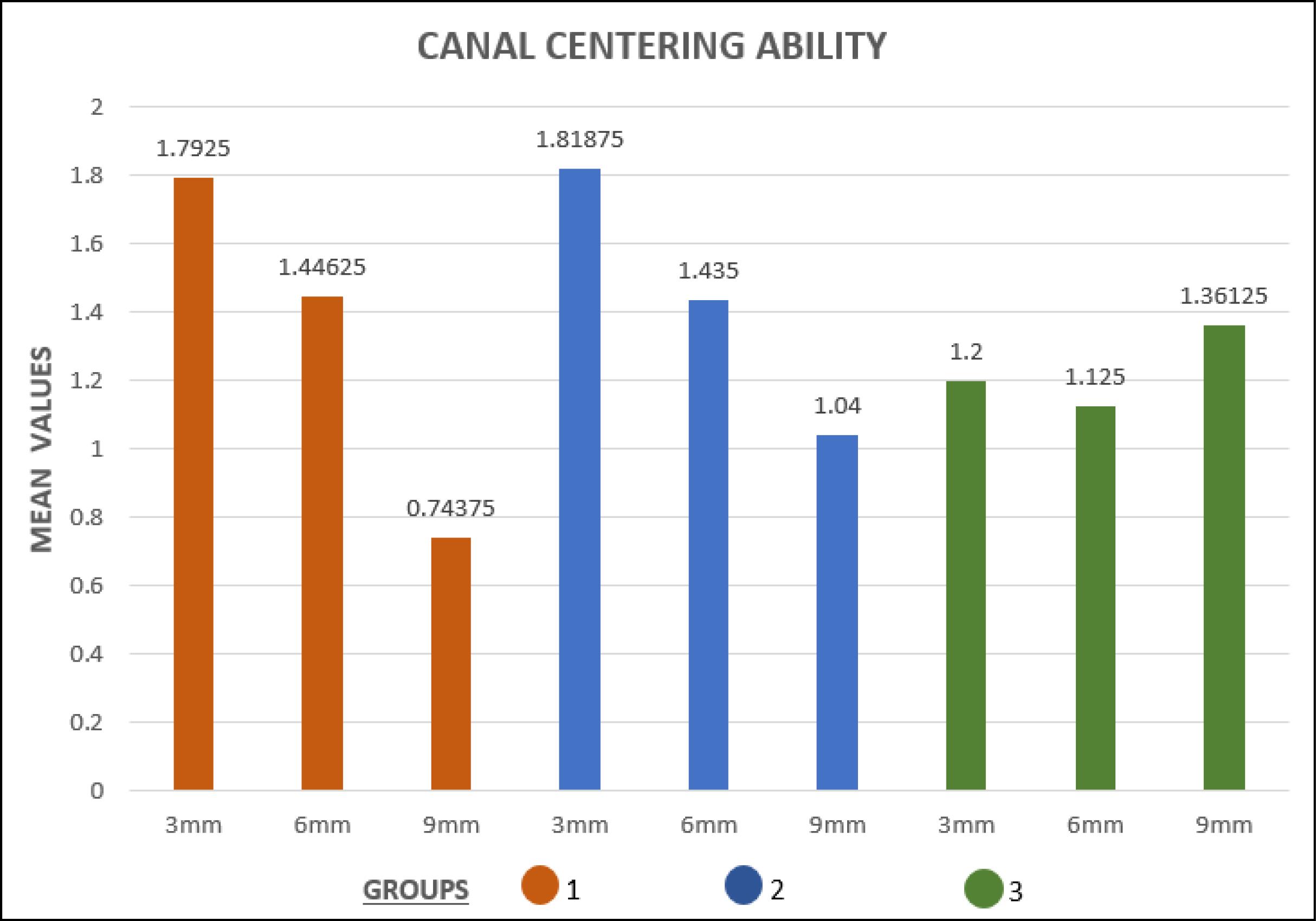
Figure 5.
Comparison of Canal Centering Ability at 3 mm, 6 mm, and 9 mm
.
Comparison of Canal Centering Ability at 3 mm, 6 mm, and 9 mm
Discussion
The major objectives of endodontic therapy are to eradicate microbes and their by-products from the root canal system and to stop infection recurrence. This involves accessing, shaping, cleaning, and ultimately sealing the root canal. A successful treatment necessitates the creation of a meticulously prepared root canal with a smooth, gradually tapered shape that maintains the original anatomy. The canal should narrow progressively from the coronal to the apical end, and the preparation should not exceed its original dimensions. This meticulous preparation allows for effective chemical debridement and subsequent sealing, preventing the possibility of reinfection (2). Root canals often exhibit complex curvatures, making it challenging to shape and clean them effectively. As the degree of curvature increases, the instruments used in these procedures can undergo stress, making it difficult to achieve the desired taper in curved canals. As a result, dentin is frequently removed from the canal walls during cleaning and shaping operations in these types of canals rather than from the original tooth axis in all directions, a phenomenon known as canal transportation (3).
Historically, stainless steel hand files were the standard tools used for root canal instrumentation, but they were associated with procedural errors in curved root canals, such as elbows, zips, danger zones, and canal transportation. To address these issues, NiTi alloy was introduced in endodontics (10), offering greater flexibility and super elasticity. In spite of these benefits, torsional overload and cyclic fatigue have caused NiTi instruments to abruptly separate during root canal instrumentation. To tackle these issues, thermomechanical processing techniques, such as M-wire, R-phase wire, and controlled memory files, have been applied to NiTi instruments to improve their performance. Several approaches have been used to evaluate the performance of root canal instruments and methods (12). Before and after instrumentation, non-destructive technologies, such as computed tomography and CBCT, have been suggested for the assessment of root canals. These methods provide more precise and non-invasive ways to assess root canal preparation by offering repeatable three-dimensional evaluations of the tooth’s internal and external morphology (13).
CBCT was employed in this research to assess and compare the canal transportation and centering ability of three different file systems in the curved mesiobuccal (MB) root canal of permanent mandibular first molars, including PTN (Dentsply, Mallifer), NeoNiTi (Orikam), and RM (FKG, Dentaire, Switzerland).
The three groups in the current investigation did not differ statistically significantly at the apical, middle, or coronal thirds of the canal transportation (P > 0.05). The coronal third’s centering ability did not, however, differ statistically significantly (P > 0.05) across any group.
Among all the experimental groups used in the study, RM (group 3) illustrated lesser canal transportation and more centered preparations. These results and favourable scores obtained by RM (group 3) as these reciprocal systems are designed with thinner core sizes, providing increased flexibility. They feature rounded triangular cross-sections with sharp cutting edges and optimized file tips. The unique design of this file minimizes the screwing effect, allowing clinicians to maintain higher control efficiency during root canal instrumentation, which is in line with the findings of other studies (9,14,15).
Enhanced canal centering ability is one of the distinctive features of reciprocating motion, which was mainly intended to reduce the possibility of root canal abnormalities. The same results were published by Tambe et al, showing that WaveOne files stayed more centrally in the canal and caused less transportation than OneShape and Rotary ProTaper files (16). These results conform to those of studies by Tambe et al and Saber at al evaluating shaping abilities of OneShape, Wave one,and Reciproc file systems (17,18). Likewise Hwang et al, Franco et al, and Maia Filho et al reported that when compared to instruments used in continuous motion,those utilized in reciprocation motion produced the least amount of canal transportation and had the best centering ability (19,20,21).
In line with earlier studies that produced comparable findings, the PTN demonstrated higher transportation in comparison to the other file systems assessed in this research, along with a reduced ability to remain in the canal’s center (21-23). Given that the PTN is designed with progressive tapers, it is less flexible overall and stiffer in particular areas. As the taper advances, the instrument’s flexibility reduces, increasing the probability of canal straightening (24,25). Its offset rectangular cross-section shape could render transportation in curved canals due to its high “screw-in” force (26).
When compared to the RM file findings in this investigation, the NeoNiTi showed better centering ratios and greater transportation values, but still better than the PTN values. These results may be explained by the increased flexibility of NeoNiTi instruments as a result of manufactured methods and controlled memory technology, which allows the file to better negotiate curvatures and respect the anatomy of the canals (27,28).
Given that this study was conducted under in-vitro conditions, a notable limitation is the variability observed in the canals of natural teeth. Therefore, care is required when applying these results to clinical settings. To validate the findings, further in vivo and future studies are required to assess the efficacy of the RM system in other teeth with variable degrees of root curvature in comparison with other rotary systems.
Conclusion
Within the parameters of this study, the following deductions can be made:
-
The data analysis revealed that each system assessed for this study generated different levels of canal transportation during the instrumentation.
-
When it involved canal transportation and centering capabilities, the RM group fared better than the other systems, followed by Neolix and ProTaper Next.
Authors’ Contribution
Conceptualization: D. Praveen.
Data curation: D. Praveen, Tashmeem Mohammad.
Formal analysis: Tashmeem Mohammad, Kalyan Satish R.
Investigation: Tashmeem Mohammad, Kaladhar Amarapu.
Methodology: Tashmeem Mohammad.
Project administration: D. Praveen, Kalyan Satish R.
Resources: Tashmeem Mohammad,D. Praveen.
Software: K. Durga Prasad.
Supervision: D. Praveen.
Validation: Tashmeem Mohammad.
Visualization: D. Praveen.
Writing–original draft: Tashmeem Mohammad, D. Praveen.
Writing–review & editing: Tashmeem Mohammad, D. Praveen.
Competing Interests
There is no conflict of interests to declare.
Ethical Approval
The Institutional Research Committee granted approval under the institution Vishnu Dental College with the ethical clearance number IECVDC/23/PG01/CE/IVT/92.
Funding
Nil.
References
- Schilder H. Cleaning and shaping the root canal. Dent Clin North Am 1974; 18(2):269-96. [ Google Scholar]
- Marzouk AM, Ghoneim AG. Computed tomographic evaluation of canal shape instrumented by different kinematics rotary nickel-titanium systems. J Endod 2013; 39(7):906-9. doi: 10.1016/j.joen.2013.04.023 [Crossref] [ Google Scholar]
- Arora A, Taneja S, Kumar M. Comparative evaluation of shaping ability of different rotary NiTi instruments in curved canals using CBCT. J Conserv Dent 2014; 17(1):35-9. doi: 10.4103/0972-0707.124127 [Crossref] [ Google Scholar]
- Thompson SA. An overview of nickel-titanium alloys used in dentistry. Int Endod J 2000; 33(4):297-310. doi: 10.1046/j.1365-2591.2000.00339.x [Crossref] [ Google Scholar]
- Capar ID, Ertas H, Ok E, Arslan H, Ertas ET. Comparative study of different novel nickel-titanium rotary systems for root canal preparation in severely curved root canals. J Endod 2014; 40(6):852-6. doi: 10.1016/j.joen.2013.10.010 [Crossref] [ Google Scholar]
- Yammine SD, Jabbour EA. Apically extruded debris following programmed over instrumentation of curved canals with three nickel titanium rotary instruments. Eur J Dent 2021; 15(1):20-6. doi: 10.1055/s-0040-1714175 [Crossref] [ Google Scholar]
- Madani Z, Soleymani A, Bagheri T, Moudi E, Bijani A, Rakhshan V. Transportation and centering ability of Neoniti and ProTaper instruments; a CBCT assessment. Iran Endod J 2017; 12(1):43-9. doi: 10.22037/iej.v12i1.12591 [Crossref] [ Google Scholar]
- Roane JB, Sabala CL, Duncanson MG Jr. The “balanced force” concept for instrumentation of curved canals. J Endod 1985; 11(5):203-11. doi: 10.1016/s0099-2399(85)80061-3 [Crossref] [ Google Scholar]
- Mustafa M. Comparative evaluation of canal-shaping abilities of RaceEvo, R-Motion, Reciproc Blue, and ProTaper Gold NiTi rotary file systems: a CBCT study. J Contemp Dent Pract 2021; 22(12):1406-12. doi: 10.5005/jp-journals-10024-3217 [Crossref] [ Google Scholar]
- Delgoshayi N, Abbasi M, Bakhtiar H, Sakhdari S, Ghannad S, Ellini MR. Canal transportation and centering ability of ProTaper and SafeSider in preparation of curved root canals: a CBCT evaluation. Iran Endod J 2018; 13(2):240-5. doi: 10.22037/iej.v13i2.19200 [Crossref] [ Google Scholar]
- Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol 1971; 32(2):271-5. doi: 10.1016/0030-4220(71)90230-1 [Crossref] [ Google Scholar]
- Chole D, Burad PA, Kundoor S, Bakle S, Devagirkar A, Deshpande R. Canal transportation-a threat in endodontics: a review. IOSR J Dent Med Sci 2016; 15(7):64-72. doi: 10.9790/0853-150786472 [Crossref] [ Google Scholar]
- Zhou H, Peng B, Zheng YF. An overview of the mechanical properties of nickel-titanium endodontic instruments. Endod Topics 2013; 29(1):42-54. doi: 10.1111/etp.12045 [Crossref] [ Google Scholar]
- Gambill JM, Alder M, del Rio CE. Comparison of nickel-titanium and stainless steel hand-file instrumentation using computed tomography. J Endod 1996; 22(7):369-75. doi: 10.1016/s0099-2399(96)80221-4 [Crossref] [ Google Scholar]
- Al-Omari TM, Arican B, Ates AA. The effect of different reciprocating angles on debris extrusion produced by R-Motion files–an in vitro study. Saudi Endod J 2024; 14(1):38-43. doi: 10.4103/sej.sej_79_23 [Crossref] [ Google Scholar]
- Aldury LA, Ali AH, Mannocci F. Reciprocation and rotation nickel-titanium file systems’ cyclic fatigue and centering ability in premolars accessed by ultraconservative and traditional access cavities: an in vitro study. Saudi Endod J 2024; 14(1):44-50. doi: 10.4103/sej.sej_80_23 [Crossref] [ Google Scholar]
- Tambe VH, Nagmode PS, Abraham S, Patait M, Lahoti PV, Jaju N. Comparison of canal transportation and centering ability of rotary ProTaper, OneShape system and WaveOne system using cone beam computed tomography: an in vitro study. J Conserv Dent 2014; 17(6):561-5. doi: 10.4103/0972-0707.144605 [Crossref] [ Google Scholar]
- Saber SE, Nagy MM, Schäfer E. Comparative evaluation of the shaping ability of WaveOne, Reciproc and OneShape single-file systems in severely curved root canals of extracted teeth. Int Endod J 2015; 48(1):109-14. doi: 10.1111/iej.12289 [Crossref] [ Google Scholar]
- Hwang YH, Bae KS, Baek SH, Kum KY, Lee W, Shon WJ. Shaping ability of the conventional nickel-titanium and reciprocating nickel-titanium file systems: a comparative study using micro-computed tomography. J Endod 2014; 40(8):1186-9. doi: 10.1016/j.joen.2013.12.032 [Crossref] [ Google Scholar]
- Franco V, Fabiani C, Taschieri S, Malentacca A, Bortolin M, Del Fabbro M. Investigation on the shaping ability of nickel-titanium files when used with a reciprocating motion. J Endod 2011; 37(10):1398-401. doi: 10.1016/j.joen.2011.06.030 [Crossref] [ Google Scholar]
- Maia Filho EM, de Castro Rizzi C, Coelho MB, Santos SF, Costa LM, Carvalho CN. Shaping ability of Reciproc, UnicOne, and ProTaper Universal in simulated root canals. ScientificWorldJournal 2015; 2015:690854. doi: 10.1155/2015/690854 [Crossref] [ Google Scholar]
- Alrahabi M, Alkady A. Comparison of the shaping ability of various nickel-titanium file systems in simulated curved canals. Saudi Endod J 2017; 7(2):97-101. doi: 10.4103/1658-5984.205126 [Crossref] [ Google Scholar]
- Silva EJ, Carapiá MF, Lopes RM, Belladonna FG, Senna PM, Souza EM. Comparison of apically extruded debris after large apical preparations by full-sequence rotary and single-file reciprocating systems. Int Endod J 2016; 49(7):700-5. doi: 10.1111/iej.12503 [Crossref] [ Google Scholar]
- Deepak J, Ashish M, Patil N, Kadam N, Yadav V, Jagdale H. Shaping ability of 5th generation Ni-Ti rotary systems for root canal preparation in curved root canals using CBCT: an in vitro study. J Int Oral Health 2015; 7(Suppl 1):57-61. [ Google Scholar]
- Saber SE, Nagy MM, Schäfer E. Comparative evaluation of the shaping ability of ProTaper Next, iRaCe and Hyflex CM rotary NiTi files in severely curved root canals. Int Endod J 2015; 48(2):131-6. doi: 10.1111/iej.12291 [Crossref] [ Google Scholar]
- Ha JH, Cheung GS, Versluis A, Lee CJ, Kwak SW, Kim HC. ‘Screw-in’ tendency of rotary nickel-titanium files due to design geometry. Int Endod J 2015; 48(7):666-72. doi: 10.1111/iej.12363 [Crossref] [ Google Scholar]
- Turpin YL, Chagneau F, Vulcain JM. Impact of two theoretical cross-sections on torsional and bending stresses of nickel-titanium root canal instrument models. J Endod 2000; 26(7):414-7. doi: 10.1097/00004770-200007000-00009 [Crossref] [ Google Scholar]
- Schäfer E, Dzepina A, Danesh G. Bending properties of rotary nickel-titanium instruments. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003; 96(6):757-63. doi: 10.1016/s1079-2104(03)00358-5 [Crossref] [ Google Scholar]