Avicenna J Dent Res. 16(4):218-224.
doi: 10.34172/ajdr.1795
Original Article
Comparison of the Efficacy of Gluma, Colgate Sensitive Pro-Relief Toothpaste, and 980 nm Diode Laser on Dentinal Tubule Occlusion: An in Vitro Study
Mahshad Noori Barkestani 1  , Arash Azizi 2, Pantea Amiri 3, Shirin Lawaf 4, *
, Arash Azizi 2, Pantea Amiri 3, Shirin Lawaf 4, *
Author information:
1Department of Periodontics, School of Dentistry, Hamadan University of Medical Sciences, Hamadan, Iran
2Oral Medicine Department, Faculty of Dentistry, Tehran University of Medical Sciences, Islamic Azad University, Tehran, Iran
3General Dentist, Faculty of Dentistry, Tehran University of Medical Sciences, Islamic Azad University, Tehran, Iran
4Prosthodontics Department, Faculty of Dentistry, Tehran University of Medical Sciences, Islamic Azad University, Tehran, Iran
Abstract
Background: Dentin hypersensitivity is a common issue among dental patients. There exist different treatments, including gels, solutions, toothpastes, and lasers. This study compared the effectiveness of Gluma, Colgate Sensitive Pro-Relief toothpaste, and 980 nm diode laser on dentinal tubule occlusion.
Methods: In this experimental study, 40 premolar teeth without caries, fractures, restorations, or root canal treatments were chosen for analysis. The enamel of the samples was removed using a bur, and then the samples were prepared and divided into four groups. Three treatments were applied to three groups of teeth, and the fourth group was considered the control group. The number of occluded, semi-occluded, and open dentinal tubules in the samples was calculated using field emission scanning electron microscopy, and the results were reported as percentages. Statistical analyses were then performed using Kolmogorov-Smirnov, one-way analysis of variance (ANOVA), and Tamhane tests.
Results: The results showed that the number of occluded dentinal tubules was 90.3%±8.23, 74.4%±11.62, 67.60%±10.62, and 15.03%±3.39 in the laser, Gluma, toothpaste, and control groups, respectively. The differences between the three treatment groups and the control group were significant (P<0.05). All three different treatments significantly occluded dentinal tubules.
Conclusion: Based on the findings, the 940 nm laser could effectively reduce dentin sensitivity.
Keywords: Dentinal tubules, Dentin sensitivity, Gluma desensitizer, Lasers
Copyright and License Information
© 2024 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Noori Barkestani M, Azizi A, Amiri P, Lawaf S. Comparison of the efficacy of Gluma, Colgate sensitive pro-relief toothpaste, and 980 nm diode laser on dentinal tubule occlusion: an in vitro study. Avicenna J Dent Res. 2024; 16(4):218-224. doi:10.34172/ajdr.1795
Background
It is common for patients to visit the dentist due to dental hypersensitivity (DH) (1), which is explained by short and sharp pain and is caused by the exposure of dentin to different stimuli, such as heat (2). DH does not involve any other pathology or defect (3). Dentin sensitivity happens when the external layer of the tooth (enamel) is lost due to various reasons, such as erosion leaving the dentin exposed to the oral environment. Non-carious cervical lesions, which can cause tooth sensitivity, occur when the enamel in the cervical part of the tooth is lost for reasons unrelated to caries. The common areas for non-carious cervical lesions are the buccal cervical area of the canines and the premolars of the two arches (4). The frequency of dentin sensitivity has been stated differently in various studies, due to differences in population, habits, diet, and research methods (5). Dentists reported the prevalence of sensitivity in their patients to be about 10%–25%, which is considered a serious problem for 1%. Its prevalence is higher in female individuals, with the age range of 20‒50, but it is more common in the age of 30‒40 (6).
Although many treatment options have been suggested for tooth sensitivity, none of them have effectively reduced sensitivity (7). Factors such as abrasion, wedge-shaped defects, periodontal atrophy, (8) trauma, bleaching, acid in food, incorrect brushing, bad oral hygiene habits, gum recession, and even removing orthodontic appliances can cause tooth sensitivity (9). The sensitivity of dentin to stimuli is not an issue as long as it is covered by protective tissues such as enamel. Electron microscope analysis reveals that the quantity of dentin tubules is eight times greater in sensitive dentin compared to insensitive dentin. Additionally, the wall of the tubules in sensitive dentin is thicker (10).
There are several theories about dentin sensitivity, including the transducer theory, the gate-control and vibration theory, and the hydrodynamic theory (11). The hydrodynamic theory is the most conventional theory explaining dentin hypersensitivity. It has been shown that dentin hypersensitivity is due to the movement of dentinal fluid. According to this theory, dentin tubules are exposed to the pulp and the environment, and mechanical, osmotic, and evaporative stimuli stimulate the dentinal fluid and ultimately cause pain and sensitivity (12). Various agents have been used for DH, including dental sealers (fluoride varnish and bonding), protein precipitants (silver nitrate), tubule occluding agents (sodium fluoride, stannous fluoride, and bioactive glass), and nerve desensitizers (potassium nitrate) (13). Further, various lasers, such as Nd:YAG, Er:YAG, CO2 and diode, have been utilized to treat dental sensitivity (14). There are several treatments for DH, but there is still no substance or treatment that effectively and irreversibly reduces pain (15).
The Gluma desensitizer is an adhesive system made of 5% glutaraldehyde and 35% hydroxyl ethyl methacrylate (HEMA) (16). Glutaraldehyde coagulates proteins and amino acids in dental tubules, obstructing dentinal tubules, and is a useful antiseptic (16). HEMA can also effectively block dentinal tubules and increase the permeability of glutaraldehyde into dentinal tubules (17).
Colgate Sensitive Pro-Relief toothpaste contains 8% arginine as an active ingredient (18). The Pro-Argin system is based on occluding dentinal tubules. It contains arginine, bicarbonate-pH buffer, and calcium carbonate, which serves as a source of calcium. A layer of calcium that coats the tooth surface forms when arginine is combined with calcium carbonate at physiological pH, closing dentinal tubules and stopping liquid leakage (19). The diode laser is a low-intensity laser employed to treat hypersensitivity (20). Low-level laser energy has been demonstrated to significantly reduce inflammation and decrease DH (21).
This study aims to compare three treatments to determine which treatment further helps occlude dentinal tubules due to its importance and prevalence in patients with teeth hypersensitivity.
Materials and Methods
In this in vitro experimental study, ten samples in each of the four groups were considered the minimum sample size according to a study by Joshi et al (22) using the one-way analysis of variance (ANOVA) Power Analysis feature of PASS 11 software, assuming an alpha of 0.05, a beta of 0.2, a standard deviation of 0.077, and an effect size of 0.57.
Forty premolar teeth were selected from newly extracted teeth for orthodontic purposes in people aged 12–25 years (Figure 1). Teeth with caries, restoration, endodontic treatment, fracture, wear, and anomalies were excluded from the study (23). Soft and hard tissue remnants were removed by Gracey curette 5/6 (HU-Friedy-USA) (24). Teeth were polished with fluoride-free pumice powder (Maquira, Brazil) using a rubber cap attached to a handpiece for 10 seconds, rinsed in distilled water for 15 seconds, and dried. They were restored in a 10% formalin solution at room temperature (25). The prepared samples were coded and randomly divided into 4 groups, including 3 treatment groups and 1 control group, each comprising 10 teeth. The enamel part of the samples in midline buccal (2 × 2 mm with 2 mm thickness) was removed by diamond fissure bur (Teeskavan, Iran). Then, a 12-blade flat conical carbide bur No. 135 (Vanetti Dia Tessin, Swiss) was used (Figure 2) to flatten the cutting surface (26). Next, the prepared samples were put in the ethylenediamine tetraacetic acid (EDTA) 17% (Nikdarman, Iran) solution for 1 minute to remove the smear layer and expose dentinal tubules to it. After immersing for 1 minute in the sodium hypochlorite solution, the samples were rinsed once more with distilled water. The distilled water was then utilized to store the samples (27).

Figure 1.
The Teeth Used in This Research
.
The Teeth Used in This Research
Figure 2.
Sharpened Teeth With an Area of 2 × 2 × 2
.
Sharpened Teeth With an Area of 2 × 2 × 2
Overall, 40 samples were randomly divided into four groups:
-
Group A (1-10 samples): Control group.
-
Group B (11-20 samples): Gluma desensitizer (Heraeus-Kulzer-Hanau, Germany) was applied to the minimum amount of one drop with the tip of the applicator on the wet dentin surface in the mid-buccal cervical area of the prepared teeth for 60 seconds, and the samples were left for 30 seconds. Then, the dental air spray nozzle was gently taken on them to dry (28). The criteria of Gluma drying on the surface were its disappearance from the surface and the surface not being shiny. Subsequently, the samples were washed for 10 seconds in distilled water (22).
-
Group C (21-30): The samples were washed with pea-sized Colgate Sensitive Pro-Relief toothpaste (USA) with the bristles at a 90-degree angle to the samples. This procedure was performed for 2 minutes per day for 14 days (29).
-
Group D (31-40): The samples received irradiation with a 980 nm diode laser (Dr. Smile, Italy) with 0.5-watt power for 15 seconds continuously, 3 times with an interval of 24 hours (4). The laser was irradiated tangentially on the mid-buccal cervical region of the sample in the form of rapid apicoronal and mesiodistal movements (4).
Dentin Analysis Through Field Emission Scanning Electron Microscopy
Before preparing the samples for placement in the Field Emission Scanning Electron Microscopy (FE-SEM) (Nikon-Japan), the crowns of the teeth were cut from the roots by a diamond bur No. 008 (Teeskavan, Iran) (30). The samples were washed and coated with a thin layer of gold (1000 angstrom) under a vacuum in a sputtering apparatus to improve conductivity (31). The microscope settings were set to 10 kV voltage and 5000 magnifications (32). Photomicrographs were randomly taken from the cervical midline of the buccal surface of the teeth (Figures 3-4). A total of 5000 dentinal tubules, whether open or closed tubules (both completely and partially closed), were manually counted from the photomicrographs. The tubules that were completely closed were considered fully closed tubules, while those with a reduced diameter but open in the center were considered semi-closed tubules (22).
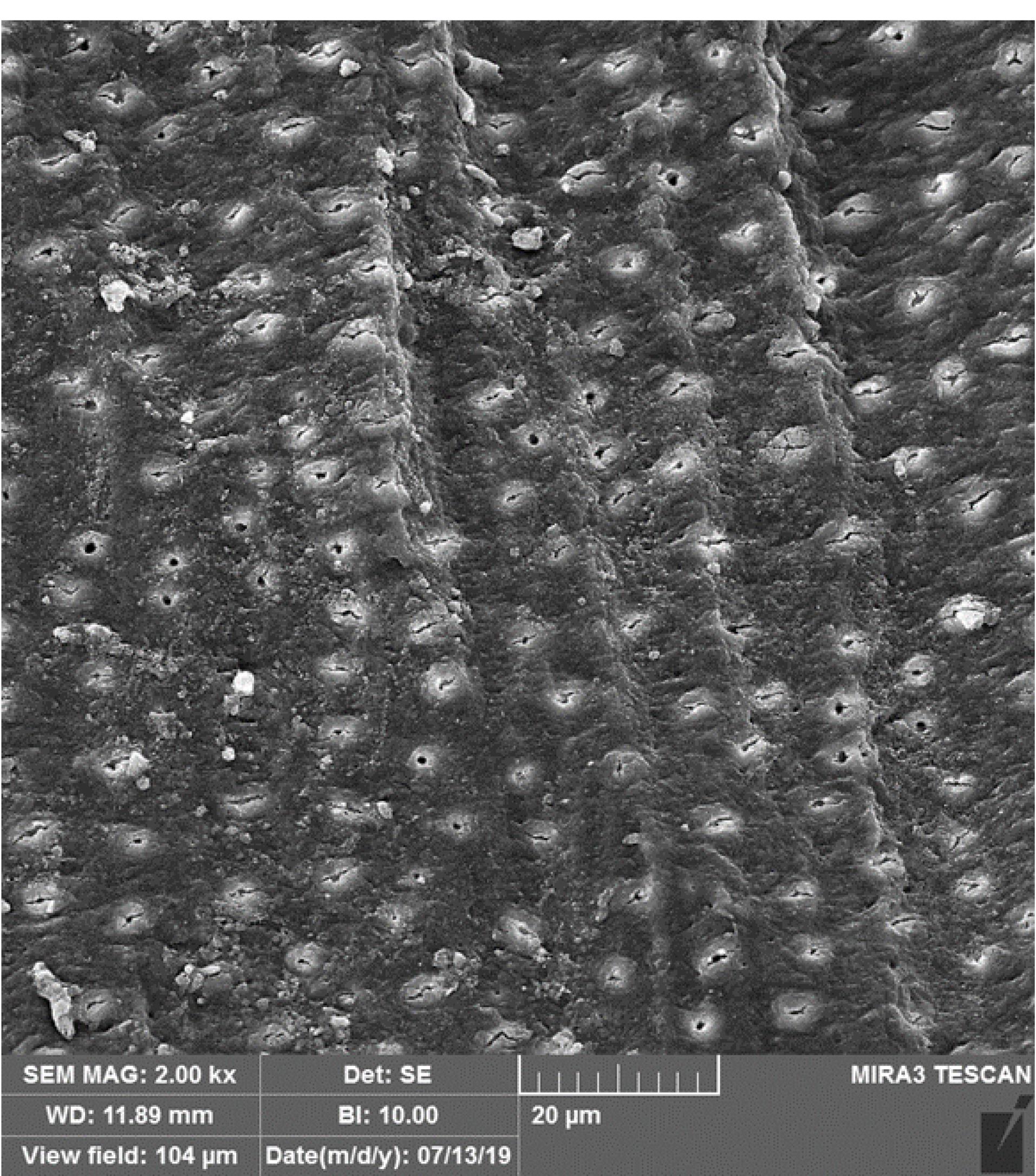
Figure 3.
Photomicrograph Taken From One of the Gluma Group Samples With Closed Tubules at 2000 Magnification
.
Photomicrograph Taken From One of the Gluma Group Samples With Closed Tubules at 2000 Magnification
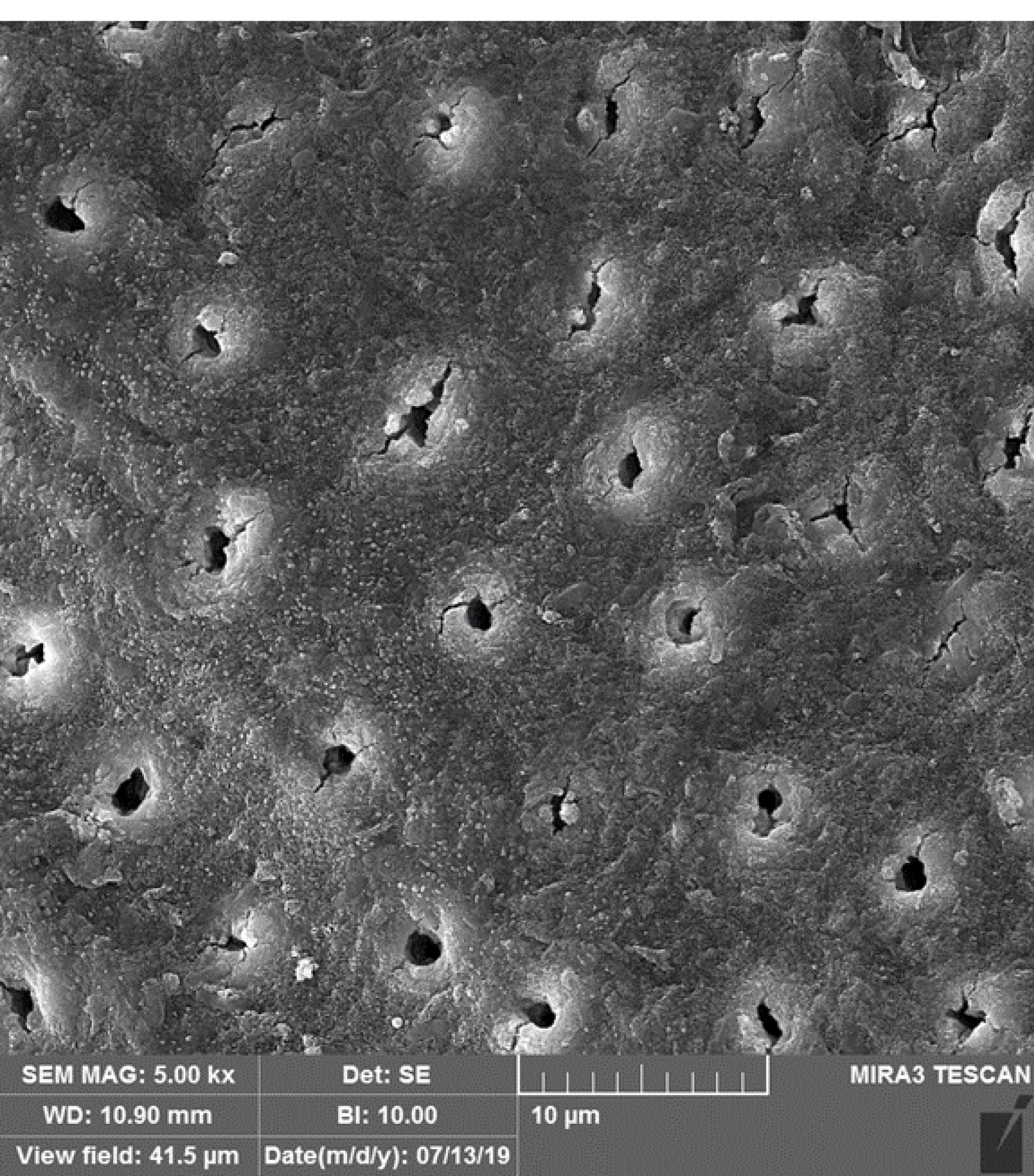
Figure 4.
Photomicrograph Taken From One of the Gluma Group Samples With Closed Tubules at 5000 Magnification
.
Photomicrograph Taken From One of the Gluma Group Samples With Closed Tubules at 5000 Magnification
The results were expressed as percentages and analyzed statistically in four groups by Kolmogorov-Smirnov, one-way ANOVA, and Tamhane tests.
Results
According to Table 1, the highest average of occluding dentinal tubules was in the 980 nm diode laser, with 90.3 ± 8.23%, followed by Gluma, Colgate Sensitive Pro-Relief toothpaste, and the control groups, with 74.4 ± 11.62%, 67.6 ± 10.62%, and 15.03 ± 3.39, respectively. The data were analyzed by the Kolmogorov-Smirnov test, and it was proved that the data distribution was normal (P > 0.05, Table 1).
Table 1.
Statistical Characteristics of Occluding Dentinal Tubules Rate in the Studied Groups
|
Groups
|
Numbers
|
Minimum
|
Maximum
|
Mean
|
Standard Deviation
|
| Control |
Percentage |
10 |
8.60 |
20.00 |
15.0300 |
3.39936 |
| Variable |
10 |
| Gluma |
Percentage |
10 |
61.00 |
100.00 |
74.4000 |
11.62564 |
| Variable |
10 |
| Colgate toothpaste |
Percentage |
10 |
50.00 |
77.00 |
67.6000 |
10.62701 |
| Variable number |
10 |
| 980 nm diode laser |
Percentage |
10 |
75.00 |
100.00 |
90.3000 |
8.23340 |
| Variable number |
10 |
Therefore, the data were analyzed using a one-way ANOVA test (Table 2). According to the results, the P value was less than 0.05 in all groups; thus, there was a significant difference in the distribution in all groups (P < 0.05).
Table 2.
One-way ANOVA Statistic
|
|
Sum of Squares
|
df.
|
Mean Square
|
F
|
Significance
|
| Between groups |
31920.787 |
3 |
10640.262 |
129.984 |
0.000 |
| Within groups |
2946.901 |
36 |
81.858 |
|
|
| Total |
34867.688 |
39 |
|
|
|
Note. df: Degree of freedom; ANOVA: Analysis of variance.
The groups were then compared two by two by post-hoc tests, and finally, the Tamhane test was performed due to the different data distribution in this study.
Based on the findings (Table 3), a significant difference was found in the four groups regarding occluding dentinal tubules (P < 0.05). Nonetheless, there was no significant difference between the Gluma and toothpaste groups (P > 0.05). However, a significant difference was observed between the 980 nm diode laser and Gluma and toothpaste groups (P < 0.05).
Table 3.
Descriptive information table of mean difference and standard error with a 95% confidence interval
|
Groups
|
Mean Difference
(I-J)
|
Standard Error
|
Significance
|
95% Confidence Interval
|
|
Lower Bound
|
Upper Bound
|
| Control |
Gluma |
-59.37000* |
3.83029 |
0.000 |
-71.7281 |
-47.0119 |
| Toothpaste |
-52.57000* |
3.52830 |
0.000 |
-63.8858 |
-41.2542 |
| Laser |
-75.27000* |
2.81682 |
0.000 |
-84.1208 |
-66.4192 |
| Gluma |
Control |
59.37000* |
3.83029 |
0.000 |
47.0119 |
71.7281 |
| Toothpaste |
6.80000 |
4.98085 |
0.716 |
-7.9224 |
21.5224 |
| Laser |
-15.90000 |
4.50494 |
0.016 |
-29.3820 |
-2.4180 |
| Colgate toothpaste |
Control |
52.57000 |
3.52830 |
0.000 |
41.2542 |
63.8858 |
| Gluma |
-6.80000 |
4.98085 |
0.716 |
-21.5224 |
7.9224 |
| Laser |
-22.70000 |
4.25114 |
0.000 |
-35.3486 |
-10.0514 |
| 980 nm diode laser |
Control |
75.27000* |
2.81682 |
0.000 |
66.4192 |
84.1208 |
| Gluma |
15.90000 |
4.50494 |
0.016 |
2.4180 |
29.3820 |
| Toothpaste |
22.70000 |
4.25114 |
0.000 |
10.0514 |
35.3486 |
The results revealed a significant difference between the control group and the other three treatment groups (P < 0.05), indicating the effectiveness of the treatment groups in occluding dentinal tubules. The Gluma group was more effective than the Colgate Sensitive Pro-Relief toothpaste, and the 980 nm diode laser was the most effective. However, there was no significant difference between the Gluma and Colgate Sensitive Pro-Relief toothpaste groups (P > 0.05).
Discussion
Dentin hypersensitivity is a prevalent problem and a clinical condition characterized by brief, sharp pains caused by various stimuli, such as touch, heat, osmotic, or chemical stimuli (33). It occurs when a stimulus leads to fluid movement in the dentinal tubules (the hydrodynamic theory), which then causes neural activity in the pulpal areas of the dentin, producing a pain impulse transmission (34). Desensitizing treatments may work on depolarizing the dental nerves or closing the dentin tubules (35). So far, various treatment methods, such as laser treatment/desensitizing gels, as well as solutions and pastes containing various compounds (e.g., fluoride, potassium nitrate, and oxalate), have been provided to reduce tooth sensitivity. DH is multifactorial in etiology; however, exposure of dentin to the oral environment is believed to be the main cause (36). Some people are at higher risk for DH, including people who brush too hard, patients with periodontal disease, bulimic patients, people with xerostomia, people who consume a lot of acidic food and drinks, older adults who have gingivitis, and people who chew tobacco (37). Considering that tooth sensitivity is a common and painful oral condition that irritates patients, new treatments are constantly being developed to alleviate these symptoms (32). Colgate Sensitive Pro-Relief toothpaste, Gluma desensitizer, and 980 nm diode laser are among the therapeutic methods for occluding dentin tubules, the effects of which have undergone investigation. After an evidence-based search, several studies using treatment methods, including laser, were obtained, the results of which can be useful in occluding dentinal tubules and treating DH (34,35).
Kara et al indicated thatDH is more common in young and middle-aged people because tubule diameter decreases in old people. Thus, teeth extracted from people aged 12‒25 for orthodontic purposes were used in their study (38).
Similar to our study, Reddy et al compared the 980 nm diode laser with desensitizing toothpaste in occluding dentinal tubules. Their result revealed that the 980 nm diode laser was more effective than toothpaste (39).
Al-Khafaji et al found that diode lasers with a wavelength between 800 nm and 980 nm have little absorption in water and hydroxyapatite. This poor absorption of laser energy by the dentin causes heat aggregation and a slow increase in the temperature of the dentin surface. This temperature rise denatures the matrix and changes its shape, thus sealing tubules in low-power lasers (40). In this study, changes in SEM photomicrographs were observed after using a low-power laser, which can be mentioned as one of the main reasons for the success and superiority of lasers over other treatment methods. In the study by Al-Khafaji et al, the SEM analysis revealed that the higher power of the laser led to a greater effect of the laser on the dentin surface due to the higher energy absorbed to the extent that irreversible damage was observed on the surface of the tubules with a laser with a power of 3 W. High-power lasers melt and recrystallize the matrix on the dentin surface, while low-power lasers act directly on nerve endings in the pulp and cause changes in nerve conduction. Therefore, using low-power lasers in in-vivo studies will probably show a better effect.
Liu et al concluded that structural changes in the dentin are caused by the laser energy. The absorption of energy causes the crystalline structure and melting by the mineral part of the dentin, which includes carbonate and phosphate. The mechanism of operation of the 980 nm laser is similar to that of the 1064 nm Nd:YAG laser, as both lasers are located near the infrared region of the electromagnetic spectrum (41).
Jena et al found that when a laser beam hits the surface of a target tissue, there are four ways in which the energy of light may be affected, including reflection, transmission, absorption, or scattering. Tissue changes are primarily due to absorbed energy. Hence, in laser treatment, determining the right parameters for achieving satisfactory results in a manner free from thermal damage to the pulp, fractures, and carbonization is of paramount importance (16).
According to Corona et al, the use of laser therapy with appropriate settings can provoke physiological cell functions (2). The laser can provoke sclerotic dentin construction and thus improve the internal closure of dentinal tubules. The stimulation of odontoblasts, the formation of irregular tertiary dentin, and the sealing of dentinal tubules may reduce pain in DH (31). Therefore, in this study, a low-power laser with a power of 0.5 W was used to obtain the most changes with the least damage to the pulp.
Reddy et al reported that Pro-Argin toothpaste and Novamin had a significant effect on closing dentinal tubules in comparison with the control group (39), which is consistent with the results of our study. Toothpaste can seal dentin tubules after seven days of daily brushing (39).
Arginine and calcium carbonate with dentin-like deposits containing calcium phosphate accelerate the tubule’s closure (39). Davari et al indicated that the mechanism of the Pro-Argin system is based on the closure of dentinal tubules (6). Dentin morphological changes and tubule closure in the present study by toothpaste were due to the contents of arginine and calcium carbonate and their effects on the tubules.
Yilmaz et al found that Gluma decreased sensitivity and showed a significant difference with the control group (13). Accordingly, it is recommended that dentists apply Gluma on the prepared dentin surface to reduce post-preparation hypersensitivity. Schupbach et al demonstrated that after applying Gluma in the lumen of dentinal tubules in contact with the tubule walls, numerous transverse walls were formed with a depth of 200 mm. They hypothesized that fluid flow in dentin is affected by the formation of a septum. Moreover, due to its high water solubility, HEMA could promote glutaraldehyde entry into the tubules, where glutaraldehyde leads to serum protein stabilization in the dentinal fluid and occlusion of the tubules. Desensitizers can infiltrate tubules and reduce reactivity through forming a dentin seal on the tubule surface, without the need for light curing such as Gluma, or binding proteins and crystals in dentin tubules (41).
Based on the photomicrograph from FE-SEM, the effects of three treatments (Gluma, Colgate Sensitive Pro-Relief toothpaste, and 980 nm diode laser) on the morphology and topography of the tubules were distinct in the present study. It was observed that the laser led to surface destruction of the tubules, while other substances (Gluma and Colgate Sensitive Pro-Relief toothpaste) plugged dentinal tubules and left a smoother surface that did not deviate from the original topography of the tubules. Laser’s effects on the denaturation of a dentine organic matrix into an amorphous form might explain surface changes due to their influence (40). Gluma and Colgate Sensitive Pro-Relief toothpaste only caused a mechanical obstruction of the tubules (39). Suppose a laser-treated tooth requires a restorative treatment that needs open dentinal tubules and penetration of resin in the future. In that case, these treatments may be difficult due to the closure or destruction of the surface of the dentin tubules.
Conclusion
In the current study, the effects of the three treatment methods (Glioma, Colgate Sensitive Pro-Relief toothpaste, and 980 nm diode laser) on tubule morphology and topography were different. The 980 nm diode laser caused SEM photomicrograph changes and destruction of tubules, with minimal pulp damage, while Gluma and Colgate Sensitive Pro-Relief toothpaste blocked dentinal tubules and created a smoother surface.
According to the study results, the 980 nm diode laser appears more effective than the other two treatments. However, all three methods result in the closure or destruction of dentin tubules, making restorative treatments challenging due to the need to open dentin tubes for resin penetration.
Author’s Contribution
Conceptualization: Mahshad Noori Barkestani.
Data curation: Pantea Amiri.
Formal analysis: Arash Azizi.
Investigation: Mahshad Noori Barkestani.
Methodology: Arash Azizi.
Project administration: Mahshad Noori Barkestani.
Supervision: Shirin Lawaf.
Validation: Shirin Lawaf.
Visualization: Pantea Amiri.
Writing–original draft: Arash Azizi, Pantea Amiri.
Writing–review & editing: Mahshad Noori Barkestani, Shirin Lawaf.
Competing Interests
The authors declare that they have no conflict of interests.
Ethical Approval
The study was approved by the Ethics Committee of Tehran Azad University of Medical Sciences (No. IR.IAU.PS.Rec.1398.049).
Funding
None.
References
- Peden JW. Dental hypersensitivity. J West Soc Periodontol Periodontal Abstr 1977; 25(2):75-83. [ Google Scholar]
- Corona SA, Nascimento TN, Catirse AB, Lizarelli RF, Dinelli W, Palma-Dibb RG. Clinical evaluation of low-level laser therapy and fluoride varnish for treating cervical dentinal hypersensitivity. J Oral Rehabil 2003; 30(12):1183-9. doi: 10.1111/j.1365-2842.2003.01185.x [Crossref] [ Google Scholar]
- Femiano F, Femiano R, Lanza A, Festa MV, Rullo R, Perillo L. Efficacy of diode laser in association to sodium fluoride vs Gluma desensitizer on treatment of cervical dentin hypersensitivity A double-blind controlled trial. Am J Dent 2013; 26(4):214-8. [ Google Scholar]
- Holland GR, Narhi MN, Addy M, Gangarosa L, Orchardson R. Guidelines for the design and conduct of clinical trials on dentine hypersensitivity. J Clin Periodontol 1997; 24(11):808-13. doi: 10.1111/j.1600-051x.1997.tb01194.x [Crossref] [ Google Scholar]
- Lawaf S, Jalalian E, Roshan R, Azizi A. Effect of GLUMA desensitizer on the retention of full metal crowns cemented with Rely X U200 self-adhesive cement. J Adv Prosthodont 2016; 8(5):404-10. doi: 10.4047/jap.2016.8.5.404 [Crossref] [ Google Scholar]
- Davari A, Ataei E, Assarzadeh H. Dentin hypersensitivity: etiology, diagnosis and treatment; a literature review. J Dent (Shiraz) 2013; 14(3):136-45. [ Google Scholar]
- Abdelkarim-Elafifi H, Parada-Avendaño I, Arnabat-Domínguez J. Parameters used with diode lasers (808-980 nm) in dentin hypersensitivity management: a systematic review. J Lasers Med Sci 2022; 13:e3. doi: 10.34172/jlms.2022.03 [Crossref] [ Google Scholar]
- Liu Y, Gao J, Gao Y, Xu S, Zhan X, Wu B. In vitro study of dentin hypersensitivity treated by 980-nm diode laser. J Lasers Med Sci 2013; 4(3):111-9. [ Google Scholar]
- Biagi R, Cossellu G, Sarcina M, Pizzamiglio IT, Farronato G. Laser-assisted treatment of dentinal hypersensitivity: a literature review. Ann Stomatol (Roma) 2015; 6(3-4):75-80. doi: 10.11138/ads/2015.6.3.075 [Crossref] [ Google Scholar]
- Gholami GA, Fekrazad R, Esmaiel-Nejad A, Kalhori K. An evaluation of the occluding effects of Er;Cr:YSGG, Nd:YAG, CO₂ and diode lasers on dentinal tubules: a scanning electron microscope in vitro study. Photomed Laser Surg 2011; 29(2):115-21. doi: 10.1089/pho.2009.2628 [Crossref] [ Google Scholar]
- Daliri F, Azizi A, Goudarzi M, Lawaf S, Rahimi A. In vitro comparison of the effect of photodynamic therapy with curcumin and methylene blue on Candida albicans colonies. Photodiagnosis Photodyn Ther 2019; 26:193-8. doi: 10.1016/j.pdpdt.2019.03.017 [Crossref] [ Google Scholar]
- West NX, Lussi A, Seong J, Hellwig E. Dentin hypersensitivity: pain mechanisms and aetiology of exposed cervical dentin. Clin Oral Investig 2013; 17 Suppl 1:S9-19. doi: 10.1007/s00784-012-0887-x [Crossref] [ Google Scholar]
- Yilmaz NA, Ertas E, Orucoğlu H. Evaluation of five different desensitizers: a comparative dentin permeability and SEM investigation in vitro. Open Dent J 2017; 11:15-33. doi: 10.2174/1874210601711010015 [Crossref] [ Google Scholar]
- Vazirizadeh Y, Azizi A, Lawaf S. Comparison of the efficacy of 940-nm diode laser, Gluma, and 5% sodium fluoride varnish in dentinal tubule occlusion. Lasers Dent Sci 2022; 6(1):63-70. doi: 10.1007/s41547-021-00139-6 [Crossref] [ Google Scholar]
- Rizzante FA, Maenosono RM, Palma-Dibb RG, Duarte MA, Ishikiriama SK. Evaluation of dentinal permeability reduction provided by different desensitizing treatments. RSBO 2014; 11(3):215-3. doi: 10.21726/rsbo.v11i3.850 [Crossref] [ Google Scholar]
- Jena A, Kala S, Shashirekha G. Comparing the effectiveness of four desensitizing toothpastes on dentinal tubule occlusion: a scanning electron microscope analysis. J Conserv Dent 2017; 20(4):269-72. doi: 10.4103/jcd.Jcd_34_17 [Crossref] [ Google Scholar]
- Patil AR, Varma S, Suragimath G, Abbayya K, Zope SA, Kale V. Comparative evaluation of efficacy of iontophoresis with 033% sodium fluoride gel and diode laser alone on occlusion of dentinal tubules. J Clin Diagn Res 2017; 11(8):ZC123-6. doi: 10.7860/jcdr/2017/29428.10526 [Crossref] [ Google Scholar]
- Kumar S, Rupesh PL, Daokar SG, Yadao AK, Ghunawat DB, Sayed SS. Effect of desensitising laser treatment on the bond strength of full metal crowns: an in vitro comparative study. J Int Oral Health 2015; 7(7):36-41. [ Google Scholar]
- Miglani S, Aggarwal V, Ahuja B. Dentin hypersensitivity: recent trends in management. J Conserv Dent 2010; 13(4):218-24. doi: 10.4103/0972-0707.73385 [Crossref] [ Google Scholar]
- Saluja M, Grover HS, Choudhary P. Comparative morphologic evaluation and occluding effectiveness of Nd:YAG, CO2 and diode lasers on exposed human dentinal tubules: an invitro SEM study. J Clin Diagn Res 2016; 10(7):ZC66-70. doi: 10.7860/jcdr/2016/18262.8188 [Crossref] [ Google Scholar]
- Chu CH, Lo EC. A review of sodium fluoride varnish. Gen Dent 2006; 54(4):247-53. [ Google Scholar]
- Joshi S, Gowda AS, Joshi C. Comparative evaluation of NovaMin desensitizer and Gluma desensitizer on dentinal tubule occlusion: a scanning electron microscopic study. J Periodontal Implant Sci 2013; 43(6):269-75. doi: 10.5051/jpis.2013.43.6.269 [Crossref] [ Google Scholar]
- Patano A, Malcangi G, De Santis M, Morolla R, Settanni V, Piras F. Conservative treatment of dental non-carious cervical lesions: a scoping review. Biomedicines 2023; 11(6):1530. doi: 10.3390/biomedicines11061530 [Crossref] [ Google Scholar]
- Pantuzzo ÉS, Cunha FA, Abreu LG, Esteves Lima RP. Effectiveness of diode laser and fluoride on dentin hypersensitivity treatment: a randomized single-blinded clinical trial. J Indian Soc Periodontol 2020; 24(3):259-63. doi: 10.4103/jisp.jisp_478_19 [Crossref] [ Google Scholar]
- D’Amario M, Di Carlo M, Jahjah A, Mauro S, Natale S, Capogreco M. Ozone and laser effects on dentin hypersensitivity treatment: a randomized clinical study. J Endod 2024; 50(5):554-61. doi: 10.1016/j.joen.2024.02.007 [Crossref] [ Google Scholar]
- Rezazadeh F, Dehghanian P, Jafarpour D. Laser effects on the prevention and treatment of dentinal hypersensitivity: a systematic review. J Lasers Med Sci 2019; 10(1):1-11. doi: 10.15171/jlms.2019.01 [Crossref] [ Google Scholar]
- Yahya G, AlAlwi A, Shurayji F, Baroom W, Rajeh M, AbdelAleem N. Effectiveness of sodium fluoride varnish and/or diode laser in decreasing post-bleaching hypersensitivity: a comparative study. Saudi Dent J 2022; 34(1):62-7. doi: 10.1016/j.sdentj.2021.09.024 [Crossref] [ Google Scholar]
- Acharya AB, Chandrashekar A, Thakur S. A short term comparative evaluation of the efficacy of diode laser with desensitizing toothpastes and mouthwashes in the treatment of dentinal hypersensitivity. J Clin Exp Dent 2022; 14(3):e229-34. doi: 10.4317/jced.59063 [Crossref] [ Google Scholar]
- Jomaa K, Abdul-Hak M, Almahdi WH, Al Namly MR, Hanafi L. Efficacy of 810 nm and 650 nm diode laser alone and in combination with sodium fluoride gel in treating dentin hypersensitivity: a split-mouth randomized clinical study. Cureus 2023; 15(1):e33489. doi: 10.7759/cureus.33489 [Crossref] [ Google Scholar]
- Meng Y, Huang F, Wang S, Huang X, Lu Y, Li Y. Evaluation of dentinal tubule occlusion and pulp tissue response after using 980-nm diode laser for dentin hypersensitivity treatment. Clin Oral Investig 2023; 27(8):4843-54. doi: 10.1007/s00784-023-05114-y [Crossref] [ Google Scholar]
- Gojkov-Vukelic M, Hadzic S, Zukanovic A, Pasic E, Pavlic V. Application of diode laser in the treatment of dentine hypersensitivity. Med Arch 2016; 70(6):466-9. doi: 10.5455/medarh.2016.70.466-469 [Crossref] [ Google Scholar]
- Koppolu P, Qamar Z, Abdul NS, Shenoy M, Reddy RN, Kakti A. Noncarious cervical lesion pretreated using antimicrobial photodynamic therapy and diode laser in reducing dentin hypersensitivity bonded to different restorative material: valuation of bond values and invitro dye leakage. Photodiagnosis Photodyn Ther 2022; 39:102885. doi: 10.1016/j.pdpdt.2022.102885 [Crossref] [ Google Scholar]
- Patil CL, Pol DG, Gaikwad RP. Comparative evaluation of use of a diode laser and electrode application with and without two dentinal tubule occluding agents in the management of dentinal hypersensitivity - a clinical study. J Indian Soc Periodontol 2020; 24(6):535-40. doi: 10.4103/jisp.jisp_523_19 [Crossref] [ Google Scholar]
- El Mobadder M, Namour A, Namour M, Dib W, El Mobadder W, Maalouf E. Dentinal hypersensitivity treatment using diode laser 980 nm: in vivo study. Dent J (Basel) 2019; 7(1):5. doi: 10.3390/dj7010005 [Crossref] [ Google Scholar]
- Hasani Tabatabaei M, Chiniforush N, Hashemi G, Valizadeh S. Efficacy comparison of Nd:YAG laser, diode laser and dentine bonding agent in dentine hypersensitivity reduction: a clinical trial. Laser Ther 2018; 27(4):265-70. doi: 10.5978/islsm.27_18-OR-24 [Crossref] [ Google Scholar]
- Azizi A, Mousavian S, Taheri S, Lawaf S, Gonoudi E, Rahimi A. Comparison of the antimicrobial efficacy of photodynamic therapy with two mediators against Lactobacillus acidophilus in vitro. Photodiagnosis Photodyn Ther 2018; 21:357-62. doi: 10.1016/j.pdpdt.2018.01.014 [Crossref] [ Google Scholar]
- Suri I, Singh P, Shakir QJ, Shetty A, Bapat R, Thakur R. A comparative evaluation to assess the efficacy of 5% sodium fluoride varnish and diode laser and their combined application in the treatment of dentin hypersensitivity. J Indian Soc Periodontol 2016; 20(3):307-14. doi: 10.4103/0972-124x.181243 [Crossref] [ Google Scholar]
- Kara HB, Cakan U, Yilmaz B, Inan Kurugol P. Efficacy of diode Laser and Gluma on post‐preparation sensitivity: a randomized split‐mouth clinical study. J Esthet Restor Dent 2016; 28(6):405-11. doi: 10.1111/jerd.12230 [Crossref] [ Google Scholar]
- Reddy GV, Akula S, Malgikar S, Babu PR, Reddy GJ, Josephin JJ. Comparative scanning electron microscope analysis of diode laser and desensitizing toothpastes for evaluation of efficacy of dentinal tubular occlusion. J Indian Soc Periodontol 2017; 21(2):102-6. doi: 10.4103/jisp.jisp_153_17 [Crossref] [ Google Scholar]
- Al-Khafaji ZR, Awazli LG, Al-Maliky MA. Sealing effect of diode laser 940 nm on the dentinal tubules (in vitro study). Int J Sci Nat 2017; 8(3):583-7. [ Google Scholar]
- Schüpbach P, Lutz F, Finger WJ. Closing of dentinal tubules by Gluma desensitizer. Eur J Oral Sci 1997; 105(5 Pt 1):414-21. doi: 10.1111/j.1600-0722.1997.tb02138.x [Crossref] [ Google Scholar]