Avicenna J Dent Res. 16(2):63-69.
doi: 10.34172/ajdr.1785
Original Article
Investigating the Relationship Between Parenting Styles and Levels of Social Anxiety and Dental Anxiety in Adolescents
Forough Amirabadi 1  , Fatemeh Roshan 2, Fatemeh Akhavan Fard 3, *
, Fatemeh Roshan 2, Fatemeh Akhavan Fard 3, *
Author information:
1Department of Pediatric Dentistry, Oral and Dental Diseases Research Center, Dental School, Zahedan University of Medical Sciences, Zahedan, Iran
2General Dentist, Zahedan University of Medical Sciences, Zahedan, Iran
3Post Graduate Student of Pediatric Dentistry, Zahedan University of Medical Sciences, Zahedan, Iran
Abstract
Background: Dental anxiety is a challenge faced by dental professionals when treating young children and adolescents. It is caused by several complex factors. This study aimed to investigate the association between different parenting styles and the levels of social anxiety and dental anxiety in adolescents.
Methods: The present cross-sectional study was conducted on 126 adolescents aged 12-19 and their mothers at a private pediatric dental clinic in Zahedan in 2021. The convenience sampling method was used to select participants. The Dental Anxiety Scale (DAS) and Beck Anxiety Inventory (BAI) were employed to measure dental anxiety and social anxiety, respectively. Mothers completed the Baumrind Parenting Styles Questionnaire. Statistical analyses included variance tests, post hoc (Tukey) tests, Pearson’s correlation coefficient, and multiple linear regression analysis.
Results: According to the findings of this study, the number of mothers with permissive, authoritarian, and authoritative parenting styles was 4 (3.2%), 9 (7.1%), and 113 (89.7%), respectively. The means±standard deviations (SD) of dental anxiety in the authoritative, permissive, and authoritarian parenting styles were 45.80±28.0%, 45.31±11.83%, and 35.42±18.49%, respectively. In addition, the mean scores±SD of social anxiety in the authoritative, permissive, and authoritarian parenting styles were 22.61±17.71%, 48.81±5.24%, and 38.72 ±11.93%, respectively. According to the results, social anxiety and maternal parenting styles were significant and influential factors in dental anxiety in adolescents (P<0.001).
Conclusion: This study highlights the significant relationship between dental anxiety, social anxiety, and parenting styles in adolescents. Addressing social anxiety and understanding the impact of parenting styles can help reduce dental anxiety. Interventions should prioritize creating a supportive environment and attending to psychological well-being alongside dental care.
Keywords: Dental anxiety, Parent, Adolescents, Psychometric, Pediatric dentistry
Copyright and License Information
© 2024 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Amirabadi F, Roshan F, Akhavan Fard F. Investigating the relationship between parenting styles and levels of social anxiety and dental anxiety in adolescents. Avicenna J Dent Res. 2024; 16(2):63-69. doi:10.34172/ajdr.1785
Background
Anxiety disorders are among the most common mental health disorders affecting children and adolescents worldwide, with a prevalence rate ranging from 4.7% to 9.1% (1). The prevalence rate of anxiety disorders among Iranian children and adolescents varies, ranging from 6.8% in Saravan to 85% in Bandar Abbas (2). Social anxiety disorder is one of the most significant anxiety disorders, characterized by intense and persistent fear of one or more social or performance situations, along with excessive avoidance of these situations (1). Such conditions can have detrimental effects on children’s emotional and social development, leading to decreased performance in various areas of their lives (3).
Dental fear, also known as dental anxiety, refers to a patient’s mental state characterized by concern, unease, or extreme apprehension specifically related to dental care or visits to a dental clinic. In the case of children, dental fear or anxiety disorder, referred to as children’s dental fear or children’s dental anxiety, encompasses observable behaviors associated with dental phobia or anxiety in children, such as decreased cooperation, diminished compliance, and even resistance to treatment. The prevalence of dental fear/anxiety was found to be between 10% and 20% in various countries. Dental fear/anxiety has emerged as a prevalent issue among children and adolescents globally (4).
Anxiety related to dental interventions, particularly dental environments, can distress many patients. Highly anxious patients tend to overestimate the pain associated with dental interventions. They also tend to report higher levels of pain experienced after treatment. This issue is a common problem for both adolescents and adults (5). The fear of dentistry in individuals is a phenomenon caused by multiple complex factors. The three main groups of causative factors include individual factors (related to the individual’s maturity and temperament), external factors (related to the individual’s parents and siblings), and factors related to the dental group (6). Various studies have identified numerous factors that contribute to the development of dental fear. Some of the most important factors include age, psychological development of the individual, gender, general fears, parental anxiety, socioeconomic status of the family, the individual’s preparation at home before dental visits, peer influence, parental styles, and the like (6‒8).
Parenting styles refer to the various approaches and methods employed by parents to raise their children, emerging from customary interactions between parents and their reactions to their children’s conduct (9). Baumrind created a framework consisting of three distinct parenting styles (10). One of these styles is the authoritarian parenting style, characterized by high demands and low responsiveness from parents, resulting in less favorable outcomes in child behavior. In contrast, the authoritative style, characterized by both high control and high warmth, as well as the permissive style, characterized by low control but high warmth, were found to be associated with more positive child behavior outcomes (9-11).
Considering the importance of investigating the influential factors of anxiety and the necessity of effective management of these factors, as well as the limited research in the field of dental anxiety, particularly among adolescents, it is crucial to pay serious attention to several points. Adolescence represents a fundamental stage of growth characterized by increased independence and significant decision-making. Moreover, this period can expose individuals to various anxiety disorders, including dental anxiety. By focusing on this specific age group, the primary aims of our study were to identify distinct contributing factors to dental anxiety during this developmental stage and provide insights into targeted interventions. Considering that no research has been conducted on the relationship between parenting styles and social and dental anxiety in adolescents in Zahedan and that research in this field is limited in Iran, our research was performed to investigate the relationship between parenting styles, social anxiety, and dental anxiety among adolescents who sought treatment at a specialized pediatric and adolescent dental clinic in 2021.
Materials and Methods
This descriptive-analytical cross-sectional study was conducted on adolescents aged 12‒19 who visited a private pediatric clinic in Zahedan. The sample size for this study was determined using the formula for sample size calculation for two means testing. By utilizing the data from the study by Pop-Jordanova et al (4) and considering a significance level (α) of 0.05, a power of 80%, and a margin of error of 10%, a total of 126 adolescents and their mothers were included in the study. A convenience sampling method was used to select the participants.
If the mothers agreed to participate in the study and consented to their child’s participation, a written informed consent form was obtained from them. The inclusion criteria for the study included age between 12 and 19 years, willingness and consent to participate, no history of mental or psychological disorders, no medical conditions that could limit cognitive development, no history of dental or surgical phobia, and no chronic medical problems. Any significant deficiencies in completing the questionnaire or withdrawing from participation during the study for any reason would lead to the individual’s exclusion from the study. In such cases, another individual was replaced to ensure that the desired sample size would be completed.
Three questionnaires were used in this study. The first questionnaire assessed parenting styles (the Baumrind Parenting Styles Questionnaire), which was completed by the mothers. The second questionnaire was the Dental Anxiety Scale (DAS) to measure dental anxiety, and the third questionnaire was the Beck Anxiety Inventory (BAI) to evaluate adolescent social anxiety. The second and third questionnaires were completed by the adolescents before leaving the clinic. It should be noted that in the first session, only visits, counseling, and oral health education were offered to the adolescents. The questionnaire was completed by the person after leaving the doctor’s room and in the reception hall of the office. Completing the anxiety questionnaire at the clinic allowed the adolescents to better express their true feelings and emotions. The time required to complete the questionnaires was approximately 15 minutes. The questionnaires were administered and supervised by a dental intern in the clinic waiting area, and any necessary explanations were provided to reduce errors.
To assess parenting styles, the Baumrind Parenting Styles Questionnaire was completed by the mothers. This questionnaire measures three parenting styles, including permissive, authoritarian, and authoritative parenting styles, across 30 items on a 6-point Likert-type scale (1–6). Questions related to each style were asked, and scores ranging from 1 (completely disagree) to 6 (completely agree) were assigned to each question. The total scores for each style were determined, and the style with the highest score was considered the dominant parenting style.
The DAS was used to assess dental anxiety. This questionnaire includes four items related to different dental procedures, namely, internal feelings during dental examination sessions, expectations from treatment at the dental clinic, tooth drilling, and scaling. The questionnaire consists of 10 questions, including demographic variables, along with four questions regarding dental anxiety. As regards the scoring of the questionnaire, anxiety scores ranged from 0 to 5 for each question, resulting in a total score of 0–20. The scoring ranges were 0–4 (normal), 5–8 (mild anxiety), 9–12 (moderate anxiety), and 13–16 (severe anxiety) (12). The validity and reliability of this questionnaire have been confirmed in Iran (13).
The BAI, a self-reporting inventory developed by Beck et al, consists of 21 multiple-choice items designed to assess the severity of anxiety symptoms in both adults and adolescents. The level of anxiety based on the BAI can be categorized as minimal anxiety (0–7), mild anxiety (8–15), moderate anxiety (16–25), and severe anxiety (30–63) (14). The BAI was culturally adapted for use in the Iranian context (15). All scores obtained for the three styles, dental anxiety, and social anxiety were converted into percentages for better comparison. This study was conducted from February 2021 to April 2021.
Data Analysis
The data were analyzed using SPSS software (version 26). Descriptive statistics, including means and standard deviations (SD), were utilized to summarize the data. The analysis of variance (ANOVA) and post hoc (Tukey) tests were used to compare dental anxiety and social anxiety according to parenting styles. Pearson’s correlation coefficient was also employed to determine the relationship between dental and social anxiety and parenting style scores. Additionally, a multiple linear regression analysis was utilized to examine the impacts of parenting styles and demographic variables on dental anxiety and social anxiety in adolescents. A significance level of 0.05 was considered in all tests.
Results
Overall, 126 adolescents aged 12–19 years (mean age = 15 years) and their mothers were included in this study. Among the participants, 81 (63.5%) were female, and 46 (36.5%) were male. The number of people in the family was 5 or more in 65.1% of cases and 3 or 4 in 34.9% of cases. In addition, 95% of the adolescents were first-, second-, or third-born children of the family. In terms of the frequency of dental visits among the adolescents, 58% had visited the dentist more than three times. Among the mothers included in the study, 63.5% were in the age group of 30–49 years, and 36.5% were 50 years and older. Additionally, 66.7% and 33.3% of the mothers were housewives and employed, respectively. About 33.3% of the mothers had a high school diploma, and 4.8% were illiterate.
Mothers’ scores related to authoritative, authoritarian, and permissive parenting styles in this study were reported as 73.20 ± 11.0%, 40.38 ± 11.82%, and 47.45 ± 9.87%, respectively. Based on the dominant score, 113 people (89.7%) had an authoritative parenting style. Further, the number of mothers with permissive and authoritarian parenting styles was 4 (3.2%) and 9 (7.1%), respectively. The scores obtained from the dental anxiety and social anxiety questionnaires based on the mothers’ parenting styles are presented in Table 1. In the authoritarian style, the dental anxiety score was the lowest, while in the authoritative style, it was the highest; there was no significant difference between the two styles. The social anxiety score was the highest and lowest in the permissive and authoritative styles, respectively. A significant difference was found between the authoritative and authoritarian styles (P = 0.03) and between the authoritative and permissive styles (P = 0.01).
Table 1.
Scores of Dental and Social Anxiety Questionnaires Based on Maternal Parenting Style
|
Anxiety
|
Style
|
Mean
|
SD
|
P
Value*
|
| DAS |
Authoritative1 |
45.80 |
28.01 |
1 & 2 = 0.51
1 & 3 = 0.99
2 & 3 = 0.82 |
| Authoritarian2 |
35.42 |
18.49 |
| Permissive3 |
45.31 |
11.83 |
| BAI |
Authoritative1 |
22.62 |
17.71 |
1 & 2 = 0.03
1 & 3 = 0.01
2 & 3 = 0.58 |
| Authoritarian2 |
38.27 |
19.93 |
| Permissive3 |
48.81 |
5.24 |
Note. ANOVA: Analysis of variance; SD: Standard deviation; DAS: Dental Anxiety Scale; BAI: Beck Anxiety Inventory. *ANOVA and Tukey’s tests.
Out of 126 adolescents, 36 individuals (28.6%) were classified as having normal dental anxiety. Dental anxiety was reported as moderate, mild, and severe in 44 (34.9%), 34 (27.0%), and 12 (9.5%) individuals, respectively. In terms of social anxiety, 32 adolescents (25.4%) had no anxiety or very low levels of anxiety. Social anxiety was reported as mild, moderate, and severe in 40 (31.7%), 27 (21.4%), and 27 (21.4%) individuals, respectively. Figures 1 and 2 illustrate the levels of dental anxiety and social anxiety based on maternal parenting styles. The results indicated that for most adolescents, those raised with authoritative parenting styles (37.2%) had higher levels of dental anxiety, while those raised with authoritarian (55.6%) and permissive parenting styles (75.0%) had higher levels of mild dental anxiety (Figure 1). In terms of social anxiety, adolescents raised with an authoritative style (35.5%) and the lowest percentage (15.9%) of adolescents raised with an authoritative style had mild and severe levels of anxiety, respectively. However, in an authoritarian parenting style, 55.6% had higher levels of severe anxiety, and no adolescent had mild anxiety. In addition, all four adolescents (100%), who had mothers with permissive parenting styles, reported high levels of social anxiety (Figure 2).
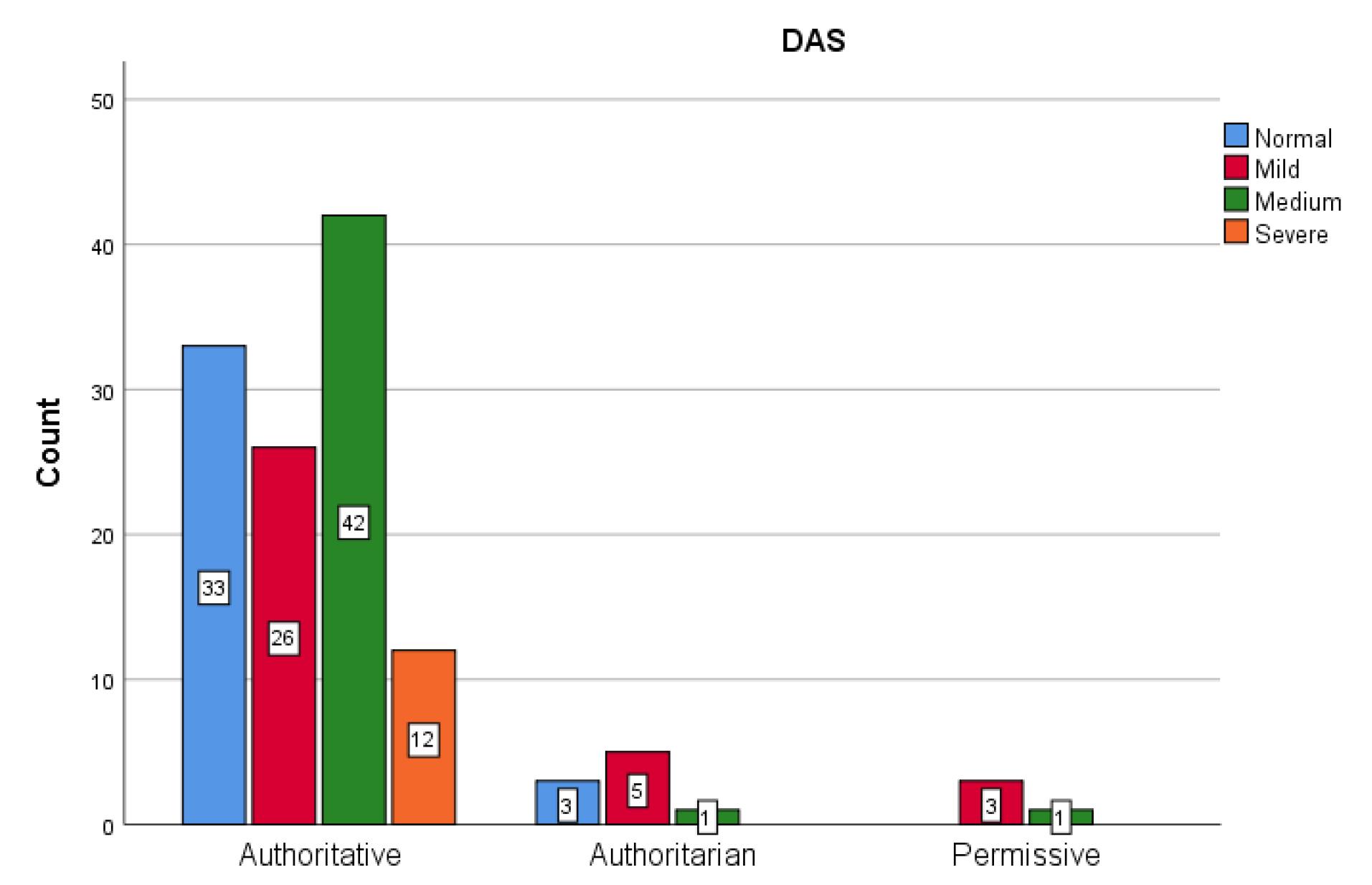
Figure 1.
Dental Anxiety Levels in Relation to Maternal Parenting Style
.
Dental Anxiety Levels in Relation to Maternal Parenting Style
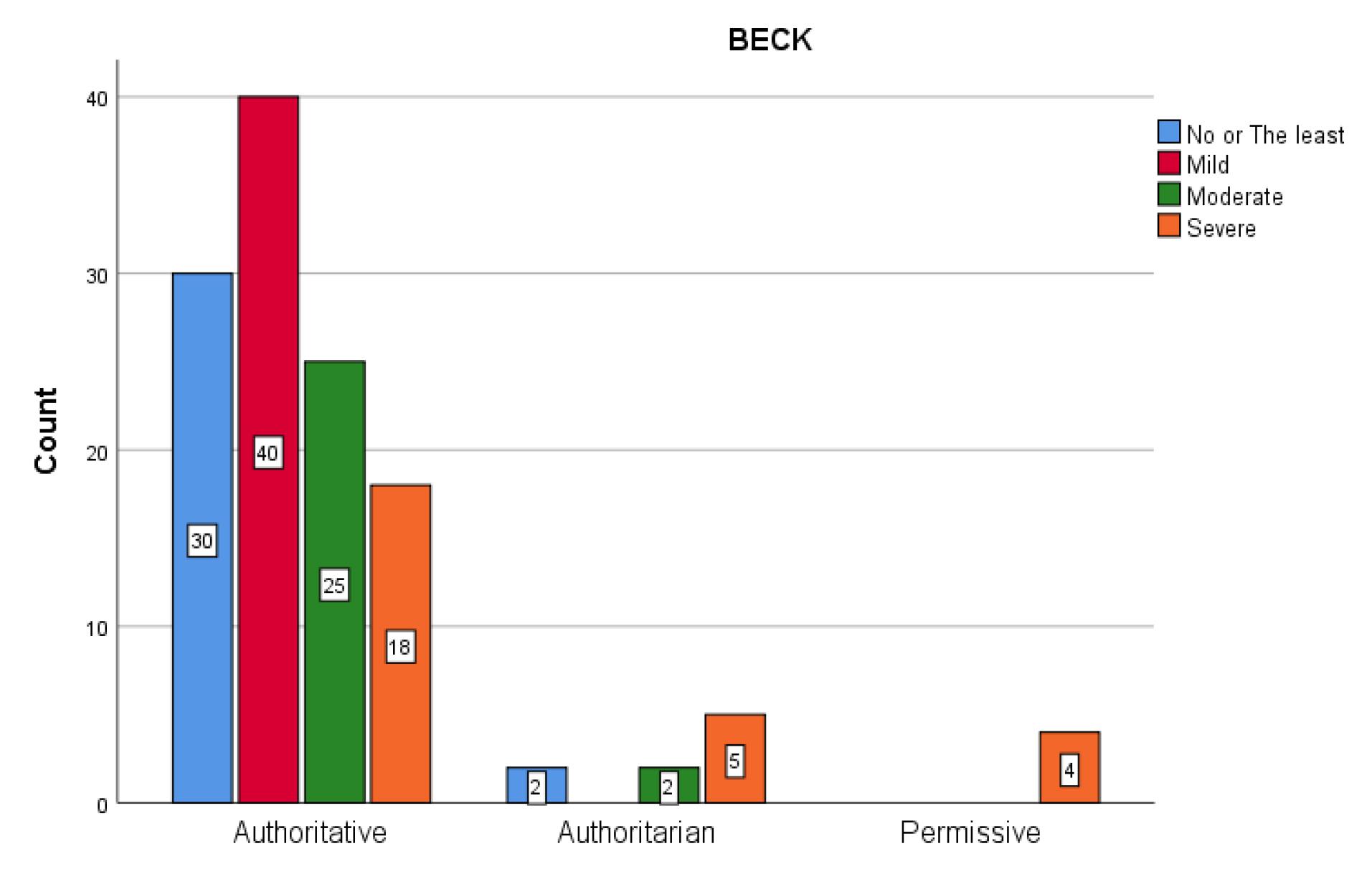
Figure 2.
Social Anxiety Levels in Relation to Maternal Parenting Style
.
Social Anxiety Levels in Relation to Maternal Parenting Style
Table 2 presents the correlation between dental anxiety and social anxiety scores and the obtained scores for each parenting style. According to the results, there was a significant positive correlation between dental anxiety and social anxiety, indicating that dental anxiety also increased by increasing social anxiety (Pearson’s correlation coefficient (r= 0.42, P = 0.0001). Furthermore, there was a significant negative correlation between the scores obtained for the authoritative style and dental anxiety (r= -0.26, P = 0.003), as well as social anxiety (r= -0.34, P = 0.0001), implying that the dental anxiety and social anxiety scores decreased by increasing the authoritative style score. The authoritarian parenting style showed a significant positive correlation only with social anxiety (r = 0.27, P = 0.002), highlighting a direct relationship between the two variables.
Table 2.
Correlation Analysis of Dental and Social Anxiety With Maternal Parenting Styles
|
Anxiety
|
Social Anxiety
|
Dental Anxiety
|
Authoritative
|
Authoritarian
|
Permissive
|
| Dental anxiety |
r*
|
0.424 |
1 |
-0.264 |
-0.029 |
-0.098 |
|
P value |
0.0001 |
|
0.003 |
0.749 |
0.274 |
| Social anxiety |
r*
|
1 |
0.424 |
-0.341 |
0.270 |
0.073 |
|
P value |
|
0.0001 |
0.0001 |
0.002 |
0.415 |
Note. r = Pearson correlation coefficient.
The final analysis using the multiple linear regression method revealed that parenting style, mothers’ age groups, and social anxiety significantly influenced dental anxiety (Table3). According to the results, in adolescents whose mothers were in the age group of 50 and above (mean ± SD of dental anxiety = 39.95 ± 27.11%), there was a significantly lower score for dental anxiety compared to those whose mothers were in the age group of 30–49 (mean ± SD of dental anxiety = 47.97 ± 26.85%) (B = -1.45, P = 0.036). Adolescents with permissive (B = -6.1, P = 0.0001) and authoritarian (B = -2.46, P = 0.017) parenting styles had significantly lower dental anxiety scores in comparison to those with an authoritative parenting style. Furthermore, similar to the univariate analysis, an increase in social anxiety was associated with an increase in dental anxiety (B = -0.16, P = 0.0001) in the multiple regression analysis.
Table 3.
Impact of Demographic Variables and Maternal Parenting Style on Dental Anxiety: Linear Regression Analysis
|
Variable
|
Regression Coefficient (B)
|
P
Value
|
| Authoritarian* |
-6.086 |
0.0001 |
| Permissive* |
-2.459 |
0.017 |
| Education |
0.225 |
0.523 |
| Age group** |
-1.454 |
0.036 |
| Job |
-0.630 |
0.533 |
| Income |
0.550 |
0.227 |
| Dental visit |
-0.537 |
0.253 |
| How many children do I have? |
-0.200 |
0.593 |
| Family size |
-0.701 |
0.403 |
| Social anxiety |
0.162 |
0.0001 |
Note. *Reference: Authoritative, **Reference: 30–49 years old.
The multiple linear regression analysis demonstrated that parenting style and dental anxiety impacted social anxiety (Table 4). According to the results, adolescents raised with permissive (B = 11.9, P = 0.001) and authoritarian (B = 6.1, P = 0.017) parenting styles had significantly higher levels of social anxiety compared to those raised with an authoritative style. Furthermore, similar to the univariate analysis, an increase in social anxiety was associated with an increase in dental anxiety (B = -0.21, P = 0.0001) in the multiple regression analysis.
Table 4.
Impact of Demographic Variables and Maternal Parenting Style on Social Anxiety: Linear Regression Analysis
|
Variable
|
Regression Coefficient (B)
|
P
Value
|
| Authoritarian* |
11.90 |
0.001 |
| Permissive* |
8.30 |
0.001 |
| Education |
0.37 |
0.70 |
| Age group** |
1.04 |
0.62 |
| Job |
1.55 |
0.57 |
| Income |
-0.23 |
0.85 |
| Dental visit |
-0.45 |
0.72 |
| Number of children |
-1.66 |
0.09 |
| Family size |
2.42 |
0.28 |
| Dental anxiety |
1.21 |
0.0001 |
Note. *Reference: Authoritative,**Reference: 30–49 years old.
Discussion
The present study aimed to evaluate the relationship between parenting styles and the levels of social anxiety and dental anxiety in adolescents. Our findings revealed that the majority of the studied population (89.7%) was raised with an authoritative parenting style, while a smaller percentage was raised with permissive (3.2%) and authoritarian (7.1%) parenting styles. These results are somewhat consistent with those of studies conducted by Mehdipor et al (16) and Shafipour et al (17), reporting a prevalence of authoritative parenting styles in their respective populations. Although the majority of the participants in our study were also raised with an authoritative parenting style, the difference in the percentage of the authoritative parenting style in the present study compared to the two previous studies could be attributed to cultural differences and social and educational development levels in the investigated communities compared to the study population of the present research.
The findings of this study indicated a relationship between maternal parenting style and dental anxiety in adolescents. It was revealed that adolescents who were raised with an authoritarian parenting style had lower levels of dental anxiety, while those raised with an authoritative parenting style had higher levels of dental anxiety. One possible interpretation is that parents with an authoritarian parenting style exert more control over their children’s behavior, which may facilitate better management of dental anxiety. Conversely, adolescents raised with an authoritative parenting style exhibited higher levels of dental anxiety, possibly due to the encouragement of independence and decision-making, leading to a greater sense of responsibility for their oral health. It is important to note that these findings may differ from those of previous studies in this field. Wood et al reported that parenting style is an important factor contributing to childhood anxiety. The findings of this study demonstrated that children who perceive their parents as warm and less controlling have better coping skills with anxiety, whereas an authoritarian parenting style is associated with higher levels of anxiety in children (18). According to the results of the study by Krikken and Veerkamp, parenting style was not related to child behavior during dental treatment (19). Viswanath et al emphasized the importance of different parenting styles for children’s cooperation and dental caries. In their study, children who were raised with an authoritarian parenting style exhibited less cooperative behavior and had higher levels of dental caries. Additionally, children raised with a permissive parenting style represented the most negative behavior and the highest levels of dental caries (20). In another study by Asl Aminabadi et al, focusing on the 4-6-year-old age group of children, those raised with an authoritative parenting style showed better behavior (21). Contrary to the findings of the present study, the results of a review study conducted by Lee et al regarding the influence of parenting styles on child behavior and dental anxiety revealed no significant relationship between dental anxiety and parenting styles in school-aged children. However, in preschool-aged children with or without a history of dental phobia, the levels of anxiety and behavior were associated with different parenting styles (22). Research results can vary due to different samples, measurement methods, and other factors. Each study has a unique sample group and method that can influence the outcomes. Therefore, it is crucial to consider these variations when interpreting the results.
Given the multidimensional nature of dental anxiety, a singular phenomenon cannot fully account for its occurrence. Research has explored the connection between dental anxiety and various personality traits, including shyness, self-consciousness, and neuroticism, revealing associations with the level of dental anxiety (23). However, limited studies have focused on the relationship between dental anxiety and social anxiety.
In the present study, a significant and positive correlation was found between dental anxiety and social anxiety, indicating an association between an increase in social anxiety and an increase in dental anxiety. Similar to dental anxiety, parenting style was another significant factor affecting social anxiety, with adolescents raised with permissive and authoritarian parenting styles exhibiting significantly higher levels of social anxiety compared to those raised with an authoritative style. Additionally, the level of social anxiety was higher in the majority of adolescents whose mothers had an authoritarian parenting style, while it was lower in those whose mothers had a permissive parenting style. In fact, severe levels of social anxiety were reported in four adolescents whose mothers had a permissive parenting style.
In a study examining the relationship between self-esteem, parenting styles, and social anxiety, Yousaf mentioned that an authoritative parenting style might predict social anxiety in individuals (23), which aligns with our study findings.
It seems that individuals raised with an authoritarian parenting style tend to be shy and fearful, experiencing difficulties in social behaviors. Among them, individuals raised with an authoritative parenting style exhibited the lowest levels of social anxiety.
Despite the findings regarding social anxiety, which indicated that adolescents raised with authoritarian and permissive parenting styles had significantly lower levels of dental anxiety compared to those raised with the authoritative parenting style, it is important to note that the number of individuals with authoritarian and permissive parenting styles was relatively small. Furthermore, the findings of the present study also demonstrated a significant relationship between the scores obtained for the authoritative style and both dental anxiety and social anxiety. As the score for the authoritative style increased, both dental anxiety and social anxiety decreased, while social anxiety increased with the higher scores of the permissive style. Therefore, considering that all mothers responded to all parenting style questions, a more precise examination of style scores (each consisting of 10 questions) could provide more accurate results, and the findings related to the association between dominant parenting styles and dental and social anxiety should be interpreted with caution.
It should be noted that, to the best of our knowledge, this is the only research conducted on adolescents in Zahedan, specifically investigating dental anxiety and social anxiety and their relationship with parenting styles. Overall, there are limited studies performed on this topic in Iran.
Limitations
In our investigated community, the predominant parenting style was the authoritative style. Our study sample consisted of individuals who sought private healthcare and had a higher social status compared to individuals who sought public healthcare or attended university. Therefore, it was expected that their parenting style would be the authoritative style. Different results would be obtained if the study were conducted on a larger scale and in diverse healthcare settings. Hence, these results cannot be generalized to a larger population or other cultures, indicating a limitation of the current study.
In the current study, only the maternal style has been addressed, while in some families, the father plays an important role in the child’s upbringing, which can be considered another limitation of the current study.
Further research is required to explore the relationship between dental anxiety and social anxiety, as well as the impact of different parenting styles on dental anxiety. Additionally, investigating the association between dental anxiety and other moral characteristics would also be beneficial.
Conclusion
The results of this study confirmed a significant relationship between the parenting style, social anxiety, and dental anxiety experienced by adolescents. The results of this study can help parents and dentists to gain a better understanding of the influence of parenting style on dental anxiety in children and adolescents. This awareness can lead parents to effective ways to reduce dental anxiety in their children. On the other hand, it was observed that social anxiety can (directly or indirectly) affect dental anxiety. In these cases, it is important that parents and dentists meet the concerns and stress of children and adolescents with social anxiety with respect and sensitivity. Creating a friendly environment, reassuring and encouraging children to experience visiting the dentist gradually, and using soothing techniques can help reduce dental anxiety. However, cooperation between parents, adolescents, and dentists is essential to determining the best strategies and methods for managing dental anxiety in any situation for any person. In addition, if the dental anxiety of a child or adolescent is so severe that it negatively impacts the quality of life and dental health, counseling from a psychological specialist can also be useful.
Acknowledgements
The authors would like to thank the Research Vice-Chancellor of Zahedan University of Medical Sciences for granting approval and providing financial support for this project. This study is based on the master’s thesis of Fatemeh Roshan, conducted at the Dental Faculty of Zahedan University of Medical Sciences, as a partial fulfillment of the requirements for the master’s degree.
Authors’ Contribution
Conceptualization: Forough Amirabadi.
Data curation: Fatemeh Roshan.
Formal analysis: Fatemeh Roshan.
Methodology: Forough Amirabadi.
Project administration: Forough Amirabadi.
Writing–original draft: Forough Amirabadi.
Writing–review & editing: Fatemeh Roshan, Fatemeh Akhavan Fard.
Competing Interests
None.
Ethical Approval
The study was approved by the Ethics Committee of Zahedan University of Medical Sciences with the ethical code IR.ZAUMS.REC.1399.426.
Funding
This study was funded by Zahedan University of Medical Sciences funded the research.
References
- Sepahvand T, Moradi J. Comparing generalized and social anxiety disorders between sinistral and dextral children with depression symptoms. J Arak Univ Med Sci 2019; 22(5):90-9. doi: 10.32598/jams.22.5.90.[Persian] [Crossref] [ Google Scholar]
- Zarafshan H, Mohammadi MR, Salmanian M. Prevalence of anxiety disorders among children and adolescents in Iran: a systematic review. Iran J Psychiatry 2015; 10(1):1-7. [ Google Scholar]
- Moharreri F, Heydari Yazdi AS. Evaluation of the effectiveness of the friends for life program on children’s anxiety and depression. Iran J Psychiatry 2017; 12(4):272-80. [ Google Scholar]
- Pop-Jordanova N, Sarakinova O, Pop-Stefanova-Trposka M, Zabokova-Bilbilova E, Kostadinovska E. Anxiety, stress and coping patterns in children in dental settings. Open Access Maced J Med Sci 2018; 6(4):692-7. doi: 10.3889/oamjms.2018.184 [Crossref] [ Google Scholar]
- Buchanan H. Assessing dental anxiety in children: the Revised Smiley Faces Program. Child Care Health Dev 2010; 36(4):534-8. doi: 10.1111/j.1365-2214.2009.01033.x [Crossref] [ Google Scholar]
- Verhoeven M, Bögels SM, van der Bruggen CC. Unique roles of mothering and fathering in child anxiety; moderation by child’s age and gender. J Child Fam Stud 2012; 21(2):331-43. doi: 10.1007/s10826-011-9483-y [Crossref] [ Google Scholar]
- Klingberg G, Broberg AG. Dental fear/anxiety and dental behaviour management problems in children and adolescents: a review of prevalence and concomitant psychological factors. Int J Paediatr Dent 2007; 17(6):391-406. doi: 10.1111/j.1365-263X.2007.00872.x [Crossref] [ Google Scholar]
- Armfield JM. How do we measure dental fear and what are we measuring anyway?. Oral Health Prev Dent 2010; 8(2):107-15. [ Google Scholar]
- Bahrami B, Dolatshahi B, Pourshahbaz A, Mohammadkhani P. Comparison of personality among mothers with different parenting styles. Iran J Psychiatry 2018; 13(3):200-6. [ Google Scholar]
- Baumrind D. Child care practices anteceding three patterns of preschool behavior. Genet Psychol Monogr 1967; 75(1):43-88. [ Google Scholar]
- Mohammadi M, Zarafshan H. Family function, parenting style and broader autism phenotype as predicting factors of psychological adjustment in typically developing siblings of children with autism spectrum disorders. Iran J Psychiatry 2014; 9(2):55-63. [ Google Scholar]
- Stouthard ME, Mellenbergh GJ, Hoogstraten J. Assessment of dental anxiety: a facet approach. Anxiety Stress Coping 1993; 6(2):89-105. doi: 10.1080/10615809308248372 [Crossref] [ Google Scholar]
- Yousefi R, Piri F. Psychometric properties of dental anxiety inventory. J Mashhad Dent Sch 2017;41(1):69-78. [Persian].
- Fallahi Khesht-Masjedi M, Shokrgozar S, Abdollahi E, Habibi B, Asghari T, Saber Ofoghi R. The relationship between gender, age, anxiety, depression, and academic achievement among teenagers. J Family Med Prim Care 2019; 8(3):799-804. doi: 10.4103/jfmpc.jfmpc_103_18 [Crossref] [ Google Scholar]
- Kaviani H, Mousavi AS. Psychometric properties of the Persian version of Beck Anxiety Inventory (BAI). Tehran Univ Med J 2008;66(2):136-40. [Persian].
- Mehdipor A, Alinejhad D, Montazeri Hedeshi R, Mohammadbeigi A. Relationship between parents’ parenting style and level of fear and cooperation of 4-8 years old children referring to dental clinics of Qom city, (Iran). Qom Univ Med Sci J 2019; 13(4):48-57. doi: 10.29252/qums.13.4.48.[Persian] [Crossref] [ Google Scholar]
- Shafipour SZ, Sheikhi A, Mirzaei M, Kazemnezhad Leyli E. Parenting styles and its relation with children behavioral problems. J Holist Nurs Midwifery 2015;25(2):49-56. [Persian].
- Wood JJ, McLeod BD, Sigman M, Hwang WC, Chu BC. Parenting and childhood anxiety: theory, empirical findings, and future directions. J Child Psychol Psychiatry 2003; 44(1):134-51. doi: 10.1111/1469-7610.00106 [Crossref] [ Google Scholar]
- Krikken JB, Veerkamp JS. Child rearing styles, dental anxiety and disruptive behaviour; an exploratory study. Eur Arch Paediatr Dent 2008; 9 Suppl 1:23-8. doi: 10.1007/bf03262652 [Crossref] [ Google Scholar]
- Viswanath S, Asokan S, Geethapriya PR, Eswara K. Parenting styles and their influence on child’s dental behavior and caries status: an analytical cross-sectional study. J Clin Pediatr Dent 2020; 44(1):8-14. doi: 10.17796/1053-4625-44.1.2 [Crossref] [ Google Scholar]
- Asl Aminabadi N, Pourkazemi M, Babapour J, Ghertasi-Oskouei S. The impact of maternal emotional intelligence and parenting style on child anxiety and behavior in the dental setting. Med Oral Patol Oral Cir Bucal 2012; 17(6):e1089-95. doi: 10.4317/medoral.17839 [Crossref] [ Google Scholar]
- Lee DW, Kim JG, Yang YM. The influence of parenting style on child behavior and dental anxiety. Pediatr Dent 2018; 40(5):327-33. [ Google Scholar]
- Yousaf S. The relation between self-esteem, parenting style and social anxiety in girls. J Educ Pract 2015; 6(1):140-2. [ Google Scholar]