Avicenna J Dent Res. 17(2):62-69.
doi: 10.34172/ajdr.1739
Original Article
Evaluation of Oral Health Status, Including Oral Mucosal Lesion Prevalence, Dental and Gingival Health, and Developmental Anomalies, in Smokers in the West of Iran in 2018
Fatemeh Ahmadi-Motamayel 1  , Fatemeh Abbasi 2, Jalal Poorolajal 3, Negin Runasi 4, *
, Fatemeh Abbasi 2, Jalal Poorolajal 3, Negin Runasi 4, *
Author information:
1Dental Research Center and Dental Implant Research Center, Department of Oral Medicine, Hamadan University of Medical Sciences, Hamadan, Iran
2Resident of Department of Oral Medicine, Hamadan University of Medical Sciences, Hamadan, Iran
3Research Center for Health Sciences and Department of Epidemiology, School of Public Health, Hamadan University of Medical Sciences, Hamadan, Iran
4Department of oral Medicine, Dental School, Hamadan University of Medical Sciences, Hamadan, Iran
Abstract
Background: Cigarette smoke contains dozens of chemicals and free radicals that could cause significant damage to the mucous membrane and dental tissues in the mouth. Therefore, the aim of this study was to evaluate the oral health and mucosal lesions, as well as the dental and gingival status, of smokers.
Methods: In this cross-sectional study, 532 smokers, including 369 males and 169 females, were evaluated to determine the prevalence of mucosal lesions and the dental health index. A dental student examined patients under dental illumination and mirrors. All the required data were collected via a questionnaire. Oral examination was classified into four groups, including mucosal lesions, developmental oral anomalies, periodontal status, and decayed, missed, and filled teeth index. Statistical analysis was performed using Stata software.
Results: The average duration of smoking and the average number of cigarettes per day were 9.0±4.8 years and 7.7±6.49 years, respectively. Among the oral mucosal lesions, coated tongue (79.7%), pigmentation (43.4%), and halitosis (81.9%) were more prevalent, and among the developmental disorders, lip pit (45.5%), Fordyce granules (36.6%) and fissured tongue (28.8%) were more prevalent. The prevalence of filling, missing, and decayed teeth was 78.9%, 71.3%, and 92.9%, respectively. The gingivitis and periodontal lesions were 89.8% and 10.6%, respectively. A significant relationship was observed between oral-dental status and smoking duration.
Conclusion: The results of this study revealed that oral and dental lesions have a high prevalence among smokers, and the incidence of these lesions is significantly associated with the duration of smoking habits and the number of cigarettes smoked per day.
Keywords: Oral ulcer, Developmental disorders, Periodontal disease, Dental caries, Smoking
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Ahmadi Motamayel F, Abbasi F, Poorolajal J, Runasi N. Evaluation of oral health status, including oral mucosal lesion prevalence, dental and gingival health, and developmental anomalies, in smokers in the west of Iran in 2018. Avicenna J Dent Res. 2025; 17(2):62-69. doi:10.34172/ajdr.1739
Background
Cigarette smoke contains dozens of chemicals and free radicals, such as carbon monoxide, ammonia, dimethyl nitrosamine, formaldehyde, and cyanide, which can cause significant damage to the mucosal and dental tissue. Smoking is one of the main public health challenges in the world, while exposure to cigarette smoke is considered a risk factor for a variety of diseases, disorders, and malignancies (1-3).
There are more than 60 major carcinogens in the smoke. Today, it is well known that cigarette smoke is associated with a variety of human malignancies. Oral squamous cell carcinoma is the most common form of oral cancer, accounting for 90% of cancers in the mouth. This cancer includes 4% of all human cancers and can cause fatal complications in the face and mouth of the patient (4-6). Oral leukoplakia is the most common pre-cancerous lesion in the mouth, which can be highly malignant. Smoking, tobacco, and alcohol are considered the most important risk factors for these oral mucosal malignancies (4,7-9).
Dental caries is a microbial infectious disease that affects the calcified tissue of the tooth. The minerals are degraded and reduced in dental caries. Smoking increases the risk of tooth decay by reducing saliva secretion and, as a result, increasing the growth rate of microbial plaques (10,11).
Periodontal diseases are among the most commonly diagnosed diseases in humans. They involve periodontal tissues, including gingiva, and supportive structures such as periodontal fiber cement and alveolar bone. Chronic periodontitis is the host’s response to bacterial accumulation on tooth surfaces and causes irreversible damage to the connective tissue, resulting in the formation of periodontal pockets and ultimately the loss of alveolar bone. Studies showed that cigarette smoking could contribute to the progression of periodontal disease, which is due to the lack of proper oxygenation to the periodontal tissues and delays in tissue repair (12,13).
Developmental anomalies usually do not indicate a specific disease and include cleft lip and palate, lip pit, Fordyce granules, fissured tongue, leukoedema, hairy tongue, soft palate fistula, torus palatinus, and torus mandibularis. Oral developmental anomalies are formed due to various factors, including local conditions, systemic diseases, neoplasms, physical and chemical injuries, infectious diseases, and genetic factors (14). Some of these mucosal anomalies in smokers are more obvious and may be misdiagnosed as precancerous lesions.
Cigarette smoke is one of the most important risk factors associated with the progression and development of oral lesions (15,16).
As mentioned earlier, it seems that cigarette smoke has a great impact on the onset or progression of different oral diseases. Therefore, timely diagnosis of mucosal and dental lesions based on clinical signs can be of great help to patients’ health in smokers. Considering that there is a significant difference in the prevalence of these lesions in different parts of the world, this study aimed to evaluate mucosal and dental lesions among smokers in Hamadan, Iran.
Methods
This cross-sectional study was performed on 532 patients referring to private or public clinics, as well as the Oral Medicine Department of Hamadan University of Medical Sciences, in 2018.
Inclusion and Exclusion Criteria
The study population included smokers who consumed at least 2–3 cigarettes a day for at least one year. The exclusion criteria included people with a history of smoking who did not consume at the time of the study, those who used drugs or/and alcohol in addition to cigarettes, and those who consumed drugs that affect the mucosa (including hypertension and diabetes drugs and tricyclic antidepressants). The other excluded individuals were those who underwent chemotherapy and used all medications that cause dry mouth, those who had physiological pigmentation, frictional keratosis, or a systemic disease that causes mucosal pigmentation (e.g., hypo- and hyperthyroidism, Addison’s disease, Cushing’s disease, and the like), and those with complete removable prostheses.
Patients’ demographic information and status, such as consumption of cigarettes and the like, were provided in a checklist. Types of mucosal-dental lesions were recorded in four general categories, including mucosal lesions, developmental anomalies, dental health status, and periodontal diseases. Initially, a primary examination was performed under dental illumination and mirrors. In suspected cases and with the patient’s informed consent, a biopsy was taken from the affected tissue, and subsequently, a definitive diagnosis was performed by a pathologist. To evaluate dental caries, the decayed, missed, and filled teeth (DMFT) index was used based on the World Health Organization criteria. The number of permanent teeth (T = Teeth), decay (D), missing (M), or filling (F) teeth is evaluated in this index (11). Periodontal status and gingivitis were assessed based on the Silness-Löe index. Accordingly, gingivitis was categorized from 0 to 3: 0 = No inflammation, 1 = Mild inflammation; a slight change in color and a little change in texture, 2 = Moderate inflammation; moderate glazing, redness, edema, and hypertrophy; bleeding on probing, and 3 = Severe inflammation; marked redness and edema; tendency to spontaneous bleeding; ulceration (17).
Statistical analysis was performed at a 95% confidence level using Stata software, version 14. A logistic regression test was used to determine the relationship between the duration of smoking and the number of cigarettes smoked with oral and dental lesions. Furthermore, the Pearson correlation coefficient was utilized to determine the relationship between the duration of smoking and the number of smoked cigarettes with DMFT.
Results
Distribution of Age and Gender
Of the 532 patients who participated in this study, 369 (69.36%) and 169 (30.63%) cases were males and females, respectively. The mean age of males was 34.18 ± 9.85 years (the minimum and maximum age ranges were 17 and 68 years, respectively). The mean age of the females was 30.31 ± 9.39 years (minimum age 19 and maximum age of 65 years). The mean age of all patients was 32.99 ± 9.8 years.
Smoking Duration and Number of Smoke Cigarettes
The mean duration of smoking in all smokers was 9.9 ± 4.8 years, and the mean number of smoked cigarettes was 7.7 ± 6.49. The mean duration of smoking and number of cigarettes in men were 10.88 ± 8.65 years and 8.73 ± 7.12, respectively. The corresponding values for females were 4.18 ± 6.01 years and 4.14 ± 2.84, respectively.
Prevalence of Oral Mucosal Lesions in Smokers
The prevalence of mucosal lesions in smokers is provided in Table 1. Based on the results of this study, the highest prevalence was related to halitosis (436, 81.95%), coated tongue (424, 79.7%), and pigmentation (231, 43.4%). In contrast, erythroleukoplakia (1, 0.19%), squamous cell carcinoma (3, 0.66%), and giant cell granuloma (1, 0.19%) had the least prevalence. The prevalence of exophytic lesions among smokers was 39 (7.33%). All exophytic lesions were fibroma and were found in the lip buccal mucosa.
Table 1.
Prevalence of Mucosal Lesions Among Smokers Referring to the Dental Clinics
|
Mucosal Lesions
|
Yes
|
No
|
|
No.
|
%
|
No.
|
%
|
| Leukoplakia |
20 |
3.76 |
512 |
96.24 |
| Candidiasis |
84 |
15.8 |
448 |
84.21 |
| Pigmentation |
231 |
43.4 |
301 |
56.58 |
| Tooth discoloration |
92 |
17.30 |
440 |
82.70 |
| Coated tongue |
424 |
79.70 |
108 |
20.30 |
| Stomatitis nicotina of the palate |
87 |
16.35 |
445 |
83.65 |
| Erythroplakia |
25 |
7.4 |
507 |
95.3 |
| Erythroleukoplakia |
1 |
0.19 |
531 |
99.81 |
| Lichen planus |
5 |
0.94 |
527 |
99.06 |
| Oral ulceration |
50 |
9.4 |
482 |
90.6 |
| Halitosis |
436 |
81.95 |
96 |
18.05 |
| Exophytic lesions |
39 |
7.33 |
493 |
92.67 |
| Herpes |
31 |
5.83 |
501 |
94.17 |
| Squamous cell carcinoma |
3 |
0.56 |
531 |
99.43 |
| Giant cell granuloma |
1 |
0.19 |
531 |
99.81 |
The prevalence of candidiasis among smokers was 84 (15.8%). The prevalence of erythematous candidiasis, pseudomembranous, and median rhomboid glossitis was 46 (56.8%), 24 (28.6%), and 14 (16.7%), respectively. The prevalence of different types of pigmentation, including melanosis in both maxilla and mandible, localized melanosis in maxilla, localized melanosis in mandible, localized melanosis in the left buccal gingiva, and right buccal gingiva, was 165 (71.42%), 32 (13.85%), 23 (95/9%), 7 (3.03%), and 4 (1.73%), respectively.
The relationship between the duration of smoking and the number of cigarettes consumed per day with mucosal lesions was investigated using logistic regression. The results showed that in most mucosal lesions, there was a significant relationship between the incidence of mucosal lesions and the duration of smoking, or the number of cigarettes consumed per day (Table 2).
Table 2.
The Relation of Mucosal Lesions With Duration of Smoking and the Number of Cigarettes Per Day
|
Mucosal Lesions
|
Duration of Smoking
|
Number of Cigarettes (Per Day)
|
|
P
Value
|
OR (95% CI)
|
P
Value
|
OR (95% CI)
|
| Leukoplakia |
0.001 |
1.066 (1.02 – 1.1) |
0.000 |
1.09(1.04 – 1.14) |
| Candidiasis |
0.000 |
1.087 (1.06 – 1.11) |
0.000 |
1.12 (1.08 – 1.16) |
| Pigmentation |
0.012 |
1.02 (1.00 – 1.04) |
0.000 |
1.06 (1.03 – 1.09) |
| Tooth discoloration |
0.809 |
1.003 (0.976 – 1.03) |
0.280 |
1.02 (0.983 – 1.06) |
| Coated tongue |
0.001 |
1.056 (1.02 – 1.09) |
0.000 |
1.08 (1.03 – 1.14) |
| Stomatitis nicotina of the palate |
0.000 |
1.057 (1.03 – 1.08) |
0.000 |
1.11 (1.07 – 1.14) |
| Erythroplakia |
0.008 |
1.05 (1.01 – 1.09) |
0.007 |
1.06 (1.01 – 1.11) |
| Erythroleukoplakia |
0.215 |
1.099 (0.946 – 1.27) |
0.041 |
1.19 (1.00 – 1.41) |
| Lichen planus |
0.000 |
1.18 (1.08 – 1.29) |
0.000 |
1.16 (1.06 – 1.26) |
| Oral ulceration |
0.000 |
1.06 (1.03 – 1.09) |
0.000 |
1.08 (1.04 – 1.12) |
| Halitosis |
0.022 |
1.03 (1.00 – 1.07) |
0.034 |
1.04 (1.00 – 1.08) |
| Exophytic lesions |
0.073 |
0.952 (0.903 – 1.00) |
0.358 |
0.973 (0.919 – 1.03) |
| Herpes |
0.479 |
1.017 (0.969 – 1.06) |
0.580 |
0.985 (0.935 – 1.03) |
| Squamous cell carcinoma |
0.479 |
1.017 (0.969 – 1.06) |
0.580 |
0.985 (0.935 – 1.03) |
| Giant cell granuloma |
0.479 |
1.017 (0.969 – 1.06) |
0.580 |
0.985 (0.935 – 1.03) |
Note. OR: odds ratio; CI: confidence interval.
Prevalence of Developmental Disorders in Smokers
Based on the results of this study, 10 different developmental disorders were observed in the patients. The types of developmental anomalies and their prevalence are presented in Table 3. Lip pit (n = 242, 49.49%), Fordyce granules (n = 195, 36.65%), and fissured tongue (n = 153, 28.76%) were most common, while coated tongue (n = 10, 1.88%), exostosis (n = 11, 2.07%), and hairy tongue (n = 14, 2.63%) had the least prevalence.
Table 3.
Prevalence of Developmental Lesions Among Smokers
|
Developmental Lesions
|
Yes
|
No
|
|
No.
|
%
|
No.
|
%
|
| Hairy tongue |
14 |
2.63 |
518 |
97.37 |
| Coated tongue |
10 |
1.88 |
522 |
98.12 |
| Leukoedema |
30 |
5.64 |
502 |
94.36 |
| Lip pit |
242 |
45.49 |
290 |
54.51 |
| Fissured tongue |
153 |
28.76 |
379 |
71.24 |
| Torus palatinus |
23 |
4.32 |
509 |
95.68 |
| Macroglossia |
46 |
8.65 |
486 |
91.35 |
| Fordyce granules |
195 |
36.65 |
337 |
63.34 |
| Exostosis |
11 |
2.07 |
521 |
97.93 |
| Geographical tongue |
16 |
3.01 |
516 |
96.99 |
The logistic regression analysis demonstrated a significant relationship between smoking duration and developmental disorders such as lip pit, hairy tongue, fissured tongue, and exostosis in smokers (Table 4). Furthermore, a significant relationship was observed between the number of cigarettes consumed per day and developmental disorders, including a hairy tongue, coated tongue, lip pit, fissured tongue, torus mandibularis, and exostosis (Table 4).
Table 4.
Relation of Developmental Lesions With Duration of Smoking and Number of Cigarettes Per Day
|
Developmental Lesions
|
Duration of Smoking
|
Number of Cigarettes (Per Day)
|
|
P
Value
|
OR (95% CI)
|
P
Value
|
OR (95% CI)
|
| Hairy tongue |
0.035 |
1.05 (1.0 – 1.1) |
0.006 |
1.08 (1.02 – 1.14) |
| Coated tongue |
0.091 |
1.04 (1.992 – 1.1) |
0.018 |
1.08 (1.01 – 1.15) |
| Leukoedema |
0.758 |
1.006 (0.965 – 1.04) |
0.209 |
1.03 (0.982 – 1.08) |
| Lip pit |
0.002 |
1.033 (1.01 – 1.05) |
0.000 |
1.05 (1.02 – 1.08) |
| Fissured tongue |
0.000 |
1.073 (1.04 – 1.09) |
0.000 |
1.06 (1.03 – 1.09) |
| Torus palatinus |
0.12 |
0.902 (0.955 – 1.05) |
0.004 |
1.07 (1.02 – 1.12) |
| Macroglossia |
0.10 |
1.001 (0.966 – 1.03) |
0.797 |
1.00 (0.961 – 1.05) |
| Fordyce granules |
0.725 |
1.034 (0.857 – 1.24) |
0.098 |
1.15 (0.974 – 1.35) |
| Exostosis |
0.014 |
1.065 (1.01 – 1.12) |
0.000 |
1.13 (1.06 – 1.2) |
| Geographical tongue |
0.172 |
1.034 (0.985 – 1.08) |
0.510 |
0.970 (0.886 – 1.06) |
Note. OR: Odds ratio; CI: Confidence interval.
Decayed, Missed, and Filled Teeth Index in Smokers
The prevalence of dental caries (DMFT) among smokers is shown in Figure 1. Based on the results, the prevalence of filling (F), missing (M), and decayed (D) teeth was 420 (78.95%), 377 (71.27%), and 494 (92.86%), respectively. The mean of the DMFT index was 16.02 ± 6.01 (Table 5).
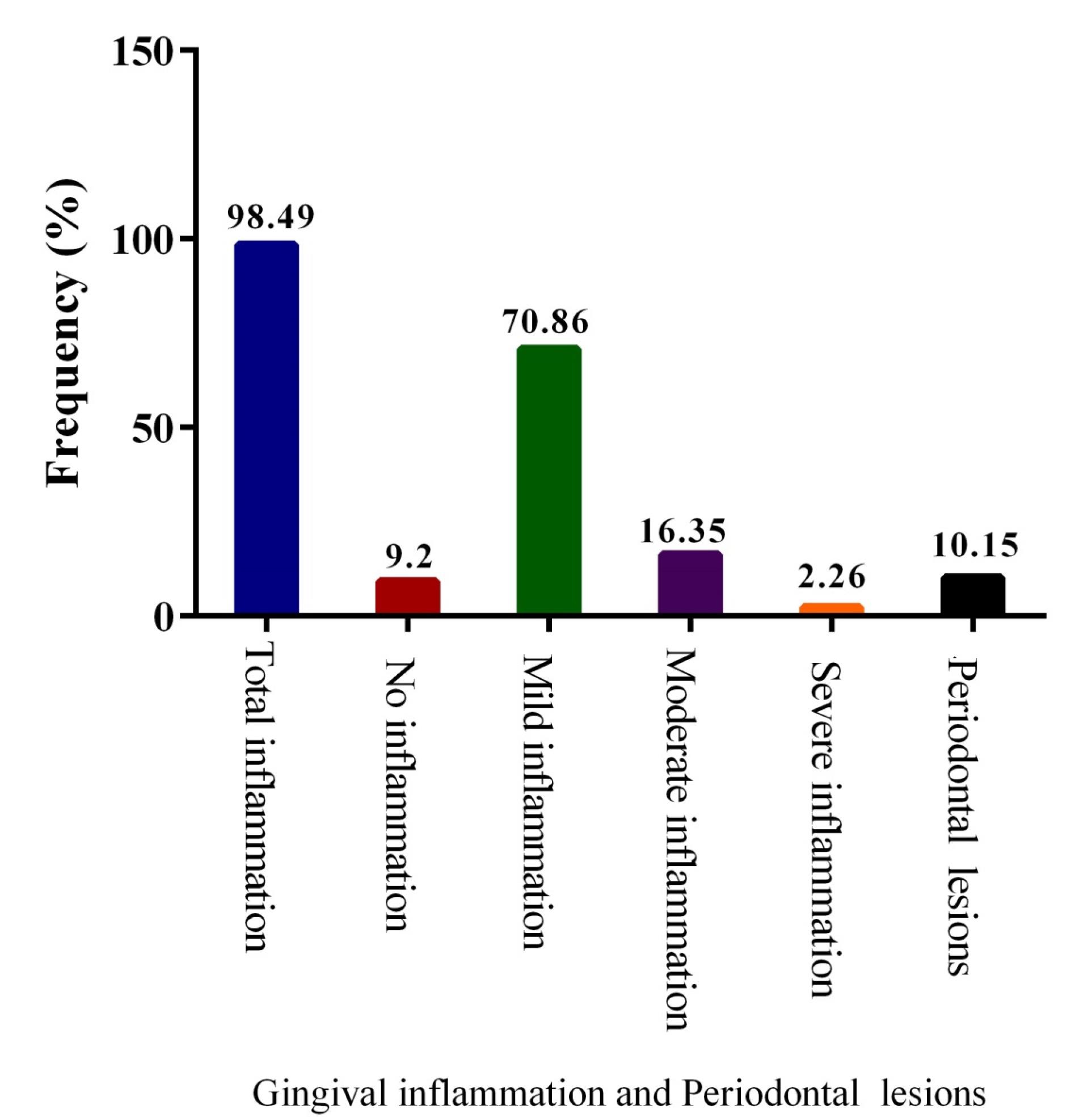
Figure 1.
The Prevalence of Gingivitis and Periodontal Lesions
.
The Prevalence of Gingivitis and Periodontal Lesions
Table 5.
Relation of Periodontal Lesions With Duration of Smoking and Number of Cigarettes Per Day
|
|
Duration of Smoking
|
Number of Cigarettes (Per Day)
|
|
P
Value
|
OR (95 % CI)
|
P
Value
|
OR (95 % CI)
|
| Periodontal lesions |
0.000 |
1.08 (1.05–1.11) |
0.000 |
1.06 (1.02–1.1) |
Note. OR: Odds ratio; CI: Confidence interval.
The Pearson correlation coefficient test was used to evaluate the relationship between the incidence of dental caries and the duration of smoking or the number of smoked cigarettes. Based on the findings, significant relationships were detected between the duration of smoking and the number of cigarettes and the incidence of dental caries.
Gingival Inflammation and Periodontal Status in Smokers
The prevalence of overall gingival inflammation among smokers was 524 (98.49%). The prevalence of gingival inflammation based on intensity was 48 (9.2%), 377 (70.86%), 87 (16.35%), and 12 (2.26%) for no inflammation, mild, moderate, and severe inflammation, respectively.
The prevalence of periodontal lesions in smokers was 54 (10.15%, Figure 1). The results of this study indicated a significant relationship between the incidence of periodontal diseases and the duration of smoking or the number of smoked cigarettes (Table 6).
Table 6.
The Prevalence of Dental Caries Among Smokers
|
|
Mean
|
SD
|
Minimum
|
Maximum
|
| Filling |
4.13 |
3.37 |
0 |
16 |
| Missing |
5.05 |
7.05 |
0 |
32 |
| Decay |
6.86 |
3.77 |
0 |
21 |
Note. SD: Standard deviation.
Discussion
The high prevalence of cigarette consumption is one of today’s problems in the human community. The smoke from cigarettes contains more than 4000 cytotoxic and mutagenic compounds that can cause significant, sometimes irreparable injuries to the oral mucosa. Smoking can change the natural and physiological oral environment and result in pathologic microorganism overgrowth, oral mucosal cell damage and pathologic changes, dental caries, gingivitis, and periodontitis (18,19).
The results of this study revealed that among mucosal lesions in smokers, coated tongue, pigmentation, and halitosis had the highest prevalence. Erythroleukoplakia, squamous cell carcinoma, and giant cell granuloma were the least common. In most mucosal lesions, including pigmentation, leukoedema, nicotine stomatitis, coated tongue, and candidiasis, there was a significant correlation between the duration of smoking and the number of cigarettes consumed per day and the incidence of mucosal lesions.
In our previous case-control study, a high prevalence of oral lesions was observed among male smokers in comparison to non-smokers. Gingival problems and coated tongues were the most prevalent (20,21).
In line with our study, Motaleb Nejad found a significant relationship between smoking and pigmentation, leukoedema, nicotine stomatitis of the palate, coated tongue, and median glossitis (22,23). Babayee et al reported that the most prevalent mucosal lesions were coated tongue (4.8%), fissured tongue (3.9%), and Lichen planus (1.8%), respectively. It was also shown that mucosal lesions were more prevalent among smokers when compared with non-smokers (24). However, the prevalence of mucosal lesions in our study was lower, which can be due to the study population. In our study, muco-dental status was only studied among smokers.
Shulman et al concluded that the prevalence of oral lesions was related to tobacco use, and this relationship was significant (25). The findings of the study by Pentenero et al revealed that smoking is associated with leukoplakia lesions, melanin pigmentation, smoker’s palate, frictional lesions, and papilloma (26). There was a significant correlation between leukoplakia and smoking in the study of Gheno et al (27). Pigmentation is mainly due to the accumulation of melanin in the oral cavity. It was demonstrated that melanin is bound to the free radicals created by cigarette smoke, nicotine, and other cigarette compounds in the oral cavity. As a result, oxidative stress is prevented in the mucosal layer, and the compounds in the cigarette are neutralized. Therefore, the increase in melanin production among tobacco users is observable. Furthermore, various studies have demonstrated that carcinogenic compounds in cigarette smoke are metabolized by the P-450 cytochromes of mucosal cells and converted into active metabolites, which can play a significant role in the development or progression of leukoplakia by attaching to DNA (28,29).
The coated tongue was reported as the most prevalent oral mucosal lesions in the study of Campisi and Margiotta (30), which conforms to our results. However, the incidence of this lesion was extremely lower than in our study (79.8% as compared with 51.4%). In the study of Axéll (31), the prevalence of coated tongue was extremely low and equal to 2.7, which was much lower than our study. It seems that the difference in the prevalence of oral lesions may be due to the racial, educational, economic, and cultural differences of different countries and populations, as well as the variety of sampling methods.
Based on the findings of this study, there was no relationship between the duration of smoking and the number of cigarettes consumed per day in the cases of exotics, erythroleukoplakia, squamous cell carcinoma, and giant cell granuloma. Although a strong correlation has been reported between some of these lesions and carcinogenic compounds present in cigarettes (4,32), it seems that a lack of relationship between these lesions and smoking duration or the number of cigarettes consumed per day is due to their pathophysiology and lower prevalence in the population.
The results of this study showed that in developmental disorders, lip pit (242.49%), Fordyce granules (195.65%), and fissured tongue (28.68%) were more common in smokers. Fordyce granules and fissured tongue in the study of Jahanbani et al (33), fissured tongue in the studies of Mansour Ghanaei et al (34) and Feng et al (35), and Fordyce granules and leukoedema in thestudy of Al-Mobeeriek and AlDosari (36) were the most common developmental abnormalities.
The results of this study demonstrated a significant correlation between the duration of smoking and the prevalence of developmental disorders, including a hairy tongue, lip pit, fissured tongue, and exostosis. There was also a significant correlation between the number of cigarettes consumed per day and developmental disorders, including a hairy tongue, coated tongue, lip pit, fissured tongue, torus palatinus, and exostosis. In this regard, the results of our study are consistent with those of Ali et al, representing the correlation between developmental disorders and smoking cigarettes (37).
However, there was no significant correlation between the duration of smoking and the number of cigarettes consumed per day with Fordyce granules and geographic tongue. In the studies of Mansour Ghanaei et al (34), and Cury et al (38), no significant difference was found in the frequency of Fordyce granules among smokers and non-smokers. In another study, Jahanbani et al (39) reported that the prevalence of Fordyce granules in non-smokers was even higher than that in smokers.
In the present study, the mean of the DMFT index was 16.02 ± 6.01. The prevalence means of filling, missing, and decayed teeth were 4.13, 5.05, and 6.86, respectively. The results of the Pearson correlation coefficient showed that there was a significant relationship between DMFT and the duration of smoking or the number of cigarettes consumed per day.
Aguilar-Zinser et al also found a significant correlation between the number of daily smoked cigarettes and DMFT (40). In a systematic review by Vellappally et al, DMFT was reported to be higher in smokers than non-smokers (11). Therefore, it seems that smoking could be an important risk factor for dental caries. However, it was observed that the frequency of DMFT in most of the studies was extremely lower than in the present study. It could be due to differences in race and culture, as well as treatment costs, among the community.
Smoking has been demonstrated to affect bone mineral content and is an important factor in alveolar bone resorption and tooth loss (41). However, the difference in DMFT between smokers and non-smokers can be attributed to a number of other factors. Smokers may have lifestyle habits that can change their oral health. In addition, smoking and dental caries are heavily dependent on educational, social, and economic factors.
In the present study, a high prevalence of gingivitis (89.47%) and periodontal lesions (10.5%) was observed in smokers. Previous studies reported contradictory results in this regard; some have shown that the progression of inflammation in response to the accumulation of microbial plaques in smokers has decreased compared to non-smokers, and therefore, gingival bleeding on probing is lower (42,43). Other studies demonstrated no difference in gingival bleeding among smokers and non-smokers (44-46).
On the other hand, the results of studies by Al-Wahadni and Linden (47) revealed that gingival bleeding in smokers was higher than in non-smokers. The findings of our study confirmed that the prevalence of gingivitis among smokers was higher than in previous studies (44,47). Smoking seems to disrupt the chemotaxis, phagocytosis, and oxidative activities of neutrophils (48,49). As a result, the response of neutrophils to plaque accumulation would be different in smokers and non-smokers.
Based on the findings of this study, there was a significant relationship between the incidence of periodontal lesions and the duration of smoking, as well as the number of smoked cigarettes. Several studies have shown a relationship between the rate of smoking and the incidence and severity of periodontitis. There was also a significant relationship between the prevalence of moderate and severe periodontal disease, and the duration of smoking (50-52) and the number of cigarettes consumed per day (51). In addition, a significant difference in probing depth, gingival recession, and clinical attachment level was observed in smokers compared to non-smokers (53).
Conclusion
The results of this study demonstrated a high prevalence of most oral-dental lesions among smokers. Mucosal lesions, including coated tongue, pigmentation, and halitosis, developmental disorders, including lip pit, Fordyce granules, and fissured tongue, as well as dental caries and gingival inflammation, were the most frequent. Furthermore, the incidence of most of these lesions in smokers was significantly related to the duration of smoking and the number of daily smoked cigarettes. Consequently, it seems that planning for the prevention, treatment, and education of these people is necessary.
Acknowledgments
The authors would like to thank the Deputy for Research of Hamadan University of Medical Sciences (Hamadan, Iran) for financial support of this research.
Competing Interests
All authors declare that they have no conflict of interest.
Ethical Approval
The study protocol was confirmed by the Ethics Committee of Hamadan University of Medical Sciences, and the approval number code was IR.UMSHA.REC.1397.28.
Funding
This study was supported by the Hamadan University of Medical Sciences.
References
- Winn DM. Tobacco use and oral disease. J Dent Educ 2001; 65(4):306-12. [ Google Scholar]
- Carter BD, Abnet CC, Feskanich D, Freedman ND, Hartge P, Lewis CE. Smoking and mortality--beyond established causes. N Engl J Med 2015; 372(7):631-40. doi: 10.1056/NEJMsa1407211 [Crossref] [ Google Scholar]
- Pinna R, Cocco F, Campus G, Conti G, Milia E, Sardella A. Genetic and developmental disorders of the oral mucosa: epidemiology; molecular mechanisms; diagnostic criteria; management. Periodontol 2000 2019; 80(1):12-27. doi: 10.1111/prd.12261 [Crossref] [ Google Scholar]
- Rivera C. Essentials of oral cancer. Int J Clin Exp Pathol 2015; 8(9):11884-94. [ Google Scholar]
- Döbrossy L. Epidemiology of head and neck cancer: magnitude of the problem. Cancer Metastasis Rev 2005; 24(1):9-17. doi: 10.1007/s10555-005-5044-4 [Crossref] [ Google Scholar]
- Warnakulasuriya S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol 2009; 45(4-5):309-16. doi: 10.1016/j.oraloncology.2008.06.002 [Crossref] [ Google Scholar]
- Neville BW, Day TA. Oral cancer and precancerous lesions. CA Cancer J Clin 2002; 52(4):195-215. doi: 10.3322/canjclin.52.4.195 [Crossref] [ Google Scholar]
- Petti S. Lifestyle risk factors for oral cancer. Oral Oncol 2009; 45(4-5):340-50. doi: 10.1016/j.oraloncology.2008.05.018 [Crossref] [ Google Scholar]
- Ford PJ, Rich AM. Tobacco use and oral health. Addiction 2021; 116(12):3531-40. doi: 10.1111/add.15513 [Crossref] [ Google Scholar]
- Roberson T, Heymann HO, Swift EJ Jr. ARABIC - Sturdevant’s Art and Science of Operative Dentistry: Arabic Bilingual Edition. Elsevier Health Sciences; 2013.
- Vellappally S, Fiala Z, Šmejkalová J, Jacob V, Shriharsha P. Influence of tobacco use in dental caries development. Cent Eur J Public Health 2007; 15(3):116-21. [ Google Scholar]
- Pejčić A, Obradović R, Kesić L, Kojović D. Smoking and periodontal disease: a review. Med Biol 2007; 14(2):53-9. [ Google Scholar]
- Sherwin GB, Nguyen D, Friedman Y, Wolff MS. The relationship between smoking and periodontal disease Review of literature and case report. N Y State Dent J 2013; 79(6):52-7. [ Google Scholar]
- Stoopler ET, Sollecito TP. Oral mucosal diseases: evaluation and management. Med Clin North Am 2014; 98(6):1323-52. doi: 10.1016/j.mcna.2014.08.006 [Crossref] [ Google Scholar]
- Behura SS, Masthan MK, Narayanasamy AB. Oral mucosal lesions associated with smokers and chewers - a case-control study in Chennai population. J Clin Diagn Res 2015; 9(7):ZC17-22. doi: 10.7860/jcdr/2015/14008.6169 [Crossref] [ Google Scholar]
- Gandini S, Botteri E, Iodice S, Boniol M, Lowenfels AB, Maisonneuve P. Tobacco smoking and cancer: a meta-analysis. Int J Cancer 2008; 122(1):155-64. doi: 10.1002/ijc.23033 [Crossref] [ Google Scholar]
- Löe H. The gingival index, the plaque index and the retention index systems. J Periodontol 1967; 38(6):610-6. doi: 10.1902/jop.1967.38.6.610 [Crossref] [ Google Scholar]
- Ahmadi-Motamayel F, Falsafi P, Hayati Z, Rezaei F, Poorolajal J. Prevalence of oral mucosal lesions in male smokers and nonsmokers. Chonnam Med J 2013; 49(2):65-68. doi: 10.4068/cmj.2013.49.2.65 [Crossref] [ Google Scholar]
- Khalili J. Oral cancer: risk factors, prevention and diagnostic. Exp Oncol 2008; 30(4):259-64. [ Google Scholar]
- Ahmadi-Motamayel F, Falsafi P, Hayati Z, Rezaei F, Poorolajal J. Prevalence of oral mucosal lesions in male smokers and nonsmokers. Chonnam Med J 2013; 49(2):65-8. doi: 10.4068/cmj.2013.49.2.65 [Crossref] [ Google Scholar]
- Chher T, Hak S, Kallarakkal TG, Durward C, Ramanathan A, Ghani WMN. Prevalence of oral cancer, oral potentially malignant disorders and other oral mucosal lesions in Cambodia. Ethn Health 2018; 23(1):1-15. doi: 10.1080/13557858.2016.1246431 [Crossref] [ Google Scholar]
- Motaleb Nejad M. The relationship between cigarette smoking and oral mucosal lesions. J Babol Univ Med Sci 1999;1(4):14-8. [Persian].
- Hernández-Morales A, González-López BS, Scougall-Vilchis RJ, Bermeo-Escalona JR, Velázquez-Enríquez U, Islas-Zarazúa R. Lip and oral cavity cancer incidence and mortality rates associated with smoking and chewing tobacco use and the human development index in 172 countries worldwide: an ecological study 2019-2020. Healthcare (Basel) 2023; 11(8):1063. doi: 10.3390/healthcare11081063 [Crossref] [ Google Scholar]
- Baabae N, Khoshsirat A, Molania T. Frequency of oral mucosal lesion in patients attending Babol Dental School, 2010. J Mazandaran Univ Med Sci 2013;23(103):114-8. [Persian].
- Shulman JD, Beach MM, Rivera-Hidalgo F. The prevalence of oral mucosal lesions in US adults: data from the Third National Health and Nutrition Examination Survey, 1988-1994. J Am Dent Assoc 2004; 135(9):1279-86. doi: 10.14219/jada.archive.2004.0403 [Crossref] [ Google Scholar]
- Pentenero M, Broccoletti R, Carbone M, Conrotto D, Gandolfo S. The prevalence of oral mucosal lesions in adults from the Turin area. Oral Dis 2008; 14(4):356-66. doi: 10.1111/j.1601-0825.2007.01391.x [Crossref] [ Google Scholar]
- Gheno JN, Martins MA, Munerato MC, Hugo FN, Sant’ana Filho M, Weissheimer C. Oral mucosal lesions and their association with sociodemographic, behavioral, and health status factors. Braz Oral Res 2015; 29:1-6. doi: 10.1590/1807-3107BOR-2015.vol29.0093 [Crossref] [ Google Scholar]
- Gümüş ZH, Du B, Kacker A, Boyle JO, Bocker JM, Mukherjee P. Effects of tobacco smoke on gene expression and cellular pathways in a cellular model of oral leukoplakia. Cancer Prev Res (Phila) 2008; 1(2):100-11. doi: 10.1158/1940-6207.capr-08-0007 [Crossref] [ Google Scholar]
- Boyle JO, Gümüş ZH, Kacker A, Choksi VL, Bocker JM, Zhou XK. Effects of cigarette smoke on the human oral mucosal transcriptome. Cancer Prev Res (Phila) 2010; 3(3):266-78. doi: 10.1158/1940-6207.capr-09-0192 [Crossref] [ Google Scholar]
- Campisi G, Margiotta V. Oral mucosal lesions and risk habits among men in an Italian study population. J Oral Pathol Med 2001; 30(1):22-8. doi: 10.1034/j.1600-0714.2001.300104.x [Crossref] [ Google Scholar]
- Axéll T. A prevalence study of oral mucosal lesions in an adult Swedish population. Odontol Revy Suppl 1976; 36:1-103. [ Google Scholar]
- Morse DE, Psoter WJ, Cleveland D, Cohen D, Mohit-Tabatabai M, Kosis DL. Smoking and drinking in relation to oral cancer and oral epithelial dysplasia. Cancer Causes Control 2007; 18(9):919-29. doi: 10.1007/s10552-007-9026-4 [Crossref] [ Google Scholar]
- Jahanbani J, Morse DE, Alinejad H. Prevalence of oral lesions and normal variants of the oral mucosa in 12 to 15-year-old students in Tehran, Iran. Arch Iran Med 2012; 15(3):142-5. [ Google Scholar]
- Mansour Ghanaei F, Joukar F, Rabiei M, Dadashzadeh A, Kord Valeshabad A. Prevalence of oral mucosal lesions in an adult Iranian population. Iran Red Crescent Med J 2013; 15(7):600-4. doi: 10.5812/ircmj.4608 [Crossref] [ Google Scholar]
- Feng J, Zhou Z, Shen X, Wang Y, Shi L, Wang Y. Prevalence and distribution of oral mucosal lesions: a cross-sectional study in Shanghai, China. J Oral Pathol Med 2015; 44(7):490-4. doi: 10.1111/jop.12264 [Crossref] [ Google Scholar]
- Al-Mobeeriek A, AlDosari AM. Prevalence of oral lesions among Saudi dental patients. Ann Saudi Med 2009; 29(5):365-8. doi: 10.4103/0256-4947.55166 [Crossref] [ Google Scholar]
- Ali M, Joseph B, Sundaram D. Prevalence of oral mucosal lesions in patients of the Kuwait University Dental Center. Saudi Dent J 2013; 25(3):111-8. doi: 10.1016/j.sdentj.2013.05.003 [Crossref] [ Google Scholar]
- Cury PR, Porto LPA, Dos Santos JN, LSF ER, de Aquino Xavier FC, Figueiredo AL. Oral mucosal lesions in Indians from Northeast Brazil: cross-sectional study of prevalence and risk indicators. Medicine (Baltimore) 2014; 93(27):e140. doi: 10.1097/md.0000000000000140 [Crossref] [ Google Scholar]
- Jahanbani J, Sandvik L, Lyberg T, Ahlfors E. Evaluation of oral mucosal lesions in 598 referred Iranian patients. Open Dent J 2009; 3:42-7. doi: 10.2174/1874210600903010042 [Crossref] [ Google Scholar]
- Aguilar-Zinser V, Irigoyen ME, Rivera G, Maupomé G, Sánchez-Pérez L, Velázquez C. Cigarette smoking and dental caries among professional truck drivers in Mexico. Caries Res 2008; 42(4):255-62. doi: 10.1159/000135670 [Crossref] [ Google Scholar]
- Hildebolt CF, Pilgram TK, Yokoyama-Crothers N, Vannier MW, Dotson M, Muckerman J. Alveolar bone height and postcranial bone mineral density: negative effects of cigarette smoking and parity. J Periodontol 2000; 71(5):683-9. doi: 10.1902/jop.2000.71.5.683 [Crossref] [ Google Scholar]
- Bergström J, Floderus-Myrhed B. Co-twin control study of the relationship between smoking and some periodontal disease factors. Community Dent Oral Epidemiol 1983; 11(2):113-6. doi: 10.1111/j.1600-0528.1983.tb01367.x [Crossref] [ Google Scholar]
- Machuca G, Rosales I, Lacalle JR, Machuca C, Bullón P. Effect of cigarette smoking on periodontal status of healthy young adults. J Periodontol 2000; 71(1):73-8. doi: 10.1902/jop.2000.71.1.73 [Crossref] [ Google Scholar]
- Bergström J, Eliasson S, Dock J. A 10-year prospective study of tobacco smoking and periodontal health. J Periodontol 2000; 71(8):1338-47. doi: 10.1902/jop.2000.71.8.1338 [Crossref] [ Google Scholar]
- Liede KE, Haukka JK, Hietanen JH, Mattila MH, Rönkä H, Sorsa T. The association between smoking cessation and periodontal status and salivary proteinase levels. J Periodontol 1999; 70(11):1361-8. doi: 10.1902/jop.1999.70.11.1361 [Crossref] [ Google Scholar]
- Gajdhar SK, Altaf K, Aljahdali RA, Gajdhar S, Wali O, Vanka S. Prevalence of oral mucosal lesions in smokers and nonsmokers: a cross-sectional study in Jeddah, Saudi Arabia. Int J Med Sci Public Health 2021; 10(2):38-42. [ Google Scholar]
- Al-Wahadni A, Linden GJ. The effects of cigarette smoking on the periodontal condition of young Jordanian adults. J Clin Periodontol 2003; 30(2):132-7. doi: 10.1034/j.1600-051x.2003.00279.x [Crossref] [ Google Scholar]
- Ryder MI, Fujitaki R, Johnson G, Hyun W. Alterations of neutrophil oxidative burst by in vitro smoke exposure: implications for oral and systemic diseases. Ann Periodontol 1998; 3(1):76-87. doi: 10.1902/annals.1998.3.1.76 [Crossref] [ Google Scholar]
- Persson L, Bergström J. Smoking and vascular density of healthy marginal gingiva. Eur J Oral Sci 1998; 106(5):953-7. doi: 10.1046/j.0909-8836.1998.eos106508.x [Crossref] [ Google Scholar]
- Alpagot T, Wolff LF, Smith QT, Tran SD. Risk indicators for periodontal disease in a racially diverse urban population. J Clin Periodontol 1996; 23(11):982-8. doi: 10.1111/j.1600-051x.1996.tb00524.x [Crossref] [ Google Scholar]
- Grossi SG, Genco RJ, Machtei EE, Ho AW, Koch G, Dunford R. Assessment of risk for periodontal disease II Risk indicators for alveolar bone loss. J Periodontol 1995; 66(1):23-9. doi: 10.1902/jop.1995.66.1.23 [Crossref] [ Google Scholar]
- Dietrich T, Walter C, Oluwagbemigun K, Bergmann M, Pischon T, Pischon N. Smoking, smoking cessation, and risk of tooth loss: the EPIC-Potsdam study. J Dent Res 2015; 94(10):1369-75. doi: 10.1177/0022034515598961 [Crossref] [ Google Scholar]
- Lafzi A, Abolfazli N, Eskandari A, Shirmohammadi A. The clinical assessment of the effects of smoking on periodontal tissues in referring patients to Tabriz dental faculty during 2005-2006. J Dent 2006;7(3-4):120-31. [Persian].