Avicenna J Dent Res. 15(1):27-31.
doi: 10.34172/ajdr.2023.1589
Case Report
Customized Zirconia Crown in Pediatric Dentistry From Concept to Reality
Gaurav Gupta 1, *  , D.K Gupta 2, Priyanka Gupta 3, Parth Shah 4, Abhishek Khairwa 5
, D.K Gupta 2, Priyanka Gupta 3, Parth Shah 4, Abhishek Khairwa 5
Author information:
1Private Practice, Wisdom Dental Clinics, Jaipur, Rajasthan, India
2Senior Consultant, Wisdom Dental Clinics, Jaipur, Rajasthan, India
3Sr. Demonstrator RUHSCDS Govt Dental College, Jaipur, Rajasthan, India
4Sr. Consultant, Saanchi Pediatric Hospital Surat, Gujarat, India
5Senior Lecturer, Department of Pediatric Dentistry, Jaipur Dental College, Jaipur, Rajasthan, India
Abstract
Catering a tooth-colored restoration in a single sitting is the fundamental objective of chairside digital dentistry with computer-aided design/computer-assisted manufacturing (CAD/CAM) technology, which became a legitimate reality with the initiation of ceramic reconstruction (CEREC) workflow. CAD/CAM dentistry has evolved through an amalgamation of diverse software and hardware upgrades since its launch to a viable chairside technology that allows pediatric dentists to treat patients in a single visit. Nowadays, CAD/CAM of dental restorations has become an ingrained fabrication process, especially for zirconium restorations. In this report, we have presented three cases to exemplify the clinical use of chairside digital dentistry (i.e., CEREC workflow) for the fabrication of a customized zirconium restoration in a single sitting to restore form, function, and occlusion for grossly decayed and decalcified primary molars, as well as esthetics for primary anterior teeth with utmost comfort of child patients with single-sitting treatment modality.
Keywords: CEREC workflow, Chairside digital dentistry, Primary molars, Single sitting, Zirconium crown
Copyright and License Information
© 2023 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Gupta G, Gupta DK, Gupta P, Shah P, Khairwa A. Customized zirconia crown in pediatric dentistry from concept to reality. Avicenna J Dent Res. 2023; 15(1):27-31. doi:10.34172/ajdr.2023.1589
Background
Primary teeth necessitate crowns due to gross cavitation, developmental defects, extensive interproximal caries leading to loss of the tooth structure, as well as supporting primary teeth after pulpectomy or pulpotomy. Heretofore, prefabricated stainless-steel crowns (SSCs) and all ceramic/zirconia crowns have been available in various sizes equal to the primary first and the second molar teeth (1). Prefabricated SSCs for primary molars in pediatric dentistry have been a benchmark for the treatment of grossly decayed and deformed primary teeth (2,3).
SSCs provide a solution with higher longevity and success than conventional restoration such as silver amalgam, composites, and glass ionomer cement for primary teeth (4). However, their metallic color has been objectionable; to conquer this problem, prefabricated zirconium crowns for primary teeth were launched as an alternative and more aesthetic option for primary anterior teeth. Various zirconia crown sizes were introduced, along with a specific preparation and cementation protocol (5).
Some deficits of prefabricated zirconia crowns were that they require significantly more tooth reduction (2 mm), and bleeding from the gum due to subgingival preparation, thus prolonging the treatment time. Furthermore, anxiety or inflammation may hinder the setting of the cement used to bond the zirconia crown to the tooth, and it cannot withstand occlusal forces such as SSCs (6). One more hurdle with both prefabricated SSC and zirconium crowns was that extraction is the only possible treatment if the tooth is grossly decayed with less amount of superstructure left for retention and stability.
To overcome these stumbling blocks, computer-aided design/computer-assisted manufacturing (CAD/CAM) technology has made enormous improvements since its introduction. Ceramic reconstruction (CEREC) is a dental technique that produces an indirect ceramic dental restoration using different computer-assisted technologies, including CAD/CAM and 3-dimensional (3D) intraoral scanning. Due to the accuracy and precision of these computer-aided impressions, modified hybrid restorations can also be milled out like crownlay and overlay for grossly decayed primary teeth, where extraction was previously the only option.
Nowadays, this technology is available as the chairside in dental clinics, and CEREC software facilitates the fabrication of customized zirconium crowns for primary teeth in just a single sitting. The remarkable mechanical properties of these restorations support the use of CAD/CAM as a trustworthy method for pediatric patients because it allows the restoration fabrication with minimal tooth preparation and low fracture rates and superior comfort for patients (7).
On the same grounds, the current report presents three cases of grossly decayed primary teeth restored in single sitting with customized zirconium crowns, fabricated chairside with the help of CEREC workflow and intraoral scanning.
Case Reports
Case 1
An 8-year-old boy was referred to our clinic with multiple decayed teeth. A medical history was taken, followed by a clinical and radiographic examination which revealed deep dentinal caries with pulpal exposure and loss of tooth structure on the left side mandibular primary second molar (75) (Figure 1A).
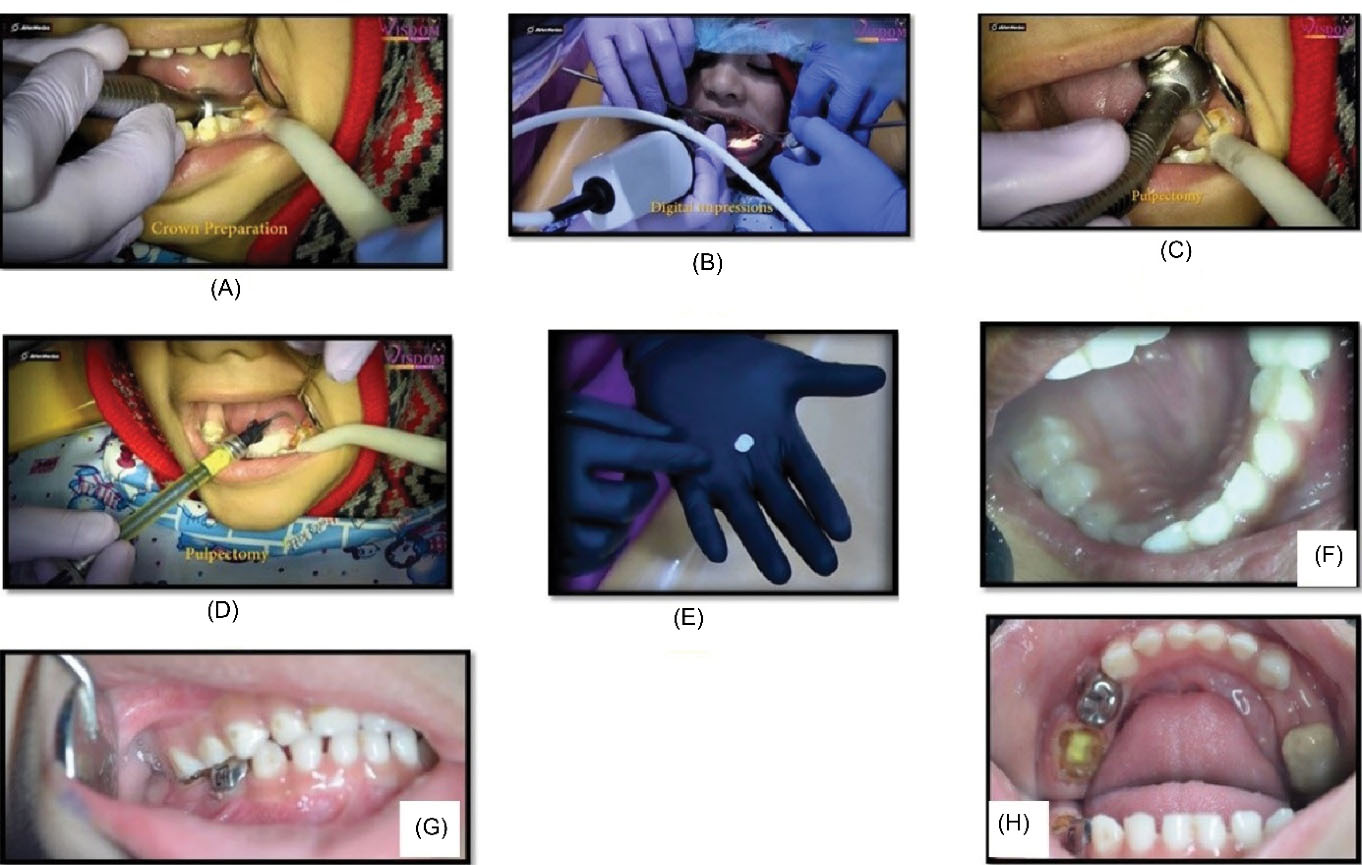
Figure 1.
(A) Crown preparation under local anaesthesia, (B) Digital impression, (C) Access cavity preparation, (D) Completed pulpectomy, (E) Customized zirconium crown fabricated chair side, (F) Post-Operative condition, and (G, H) Occlusion was checked.
.
(A) Crown preparation under local anaesthesia, (B) Digital impression, (C) Access cavity preparation, (D) Completed pulpectomy, (E) Customized zirconium crown fabricated chair side, (F) Post-Operative condition, and (G, H) Occlusion was checked.
The tooth required a full-coverage restoration, and the child and the parent were unwilling to perform conventional SSCs. Thus, we decided to restore tooth 75 with pulpectomy followed by a customized zirconium crown using intraoral scanning and chairside CEREC workflow. We exclusively altered our protocol for the procedure for single sitting chairside digital dentistry in pediatric patients.
After diagnosis and planning, we achieved local anesthesia with or without nitrous oxide inhalational sedation (NOIS) whichever was suitable as per the patient’s condition. Then, we quickly started tooth preparation (Figure 1B) followed by intraoral scanning with the help of Dentsply Sirona Omnicam to capture a digital impression for further processing in CEREC software (Figure 1C).
Scanning provides easier, more intuitive, and more precise 3D models in natural colors in less than 2 minutes. Next, we performed the pulpectomy procedure on 75 (Figures 1D, 1E, and 1F).
Simultaneously, the 3D designing and milling of the restoration were performed by another associate. As the pulpectomy was undergoing, we prepared zirconium crown chairside with CEREC prime mill in a cycle of about 11 minutes (Figure 1G).
This is India, first in-house latest generation CEREC Primemill. The milling process was extremely precise and definitive and created smooth surfaces and margins comparable to the laboratory process. A trial was conducted on the patient’s mouth to check fit and occlusion, followed by the crystallization and glazing process in CEREC speed fire.
In the meantime, a pulpectomy was completed, and once again, fitting, esthetics, and characterization were checked in the patient’s mouth. Thereafter, the tooth was cleaned, and the haemostasias of the gingiva was obtained via pressure applied with a finger. Translucent resin luting cement was used for cementation. Excess cement was removed from interdental spaces. Enjoyable and acceptable results were achieved in a matter of less than 45-minute complacent (Figures 1G and 1H).
Case 2
In our second case, a 7-year-old girl presented with a grossly decayed lower right back side tooth. She presented with a high risk of caries and already had undergone SSCs on primary molars. Clinical and radiographic examinations revealed gross decay on the primary mandibular right second molar. Interproximal caries on 85 which were crossed the line angles of the tooth, led to the loss of the primary tooth structure (Figure 2A).
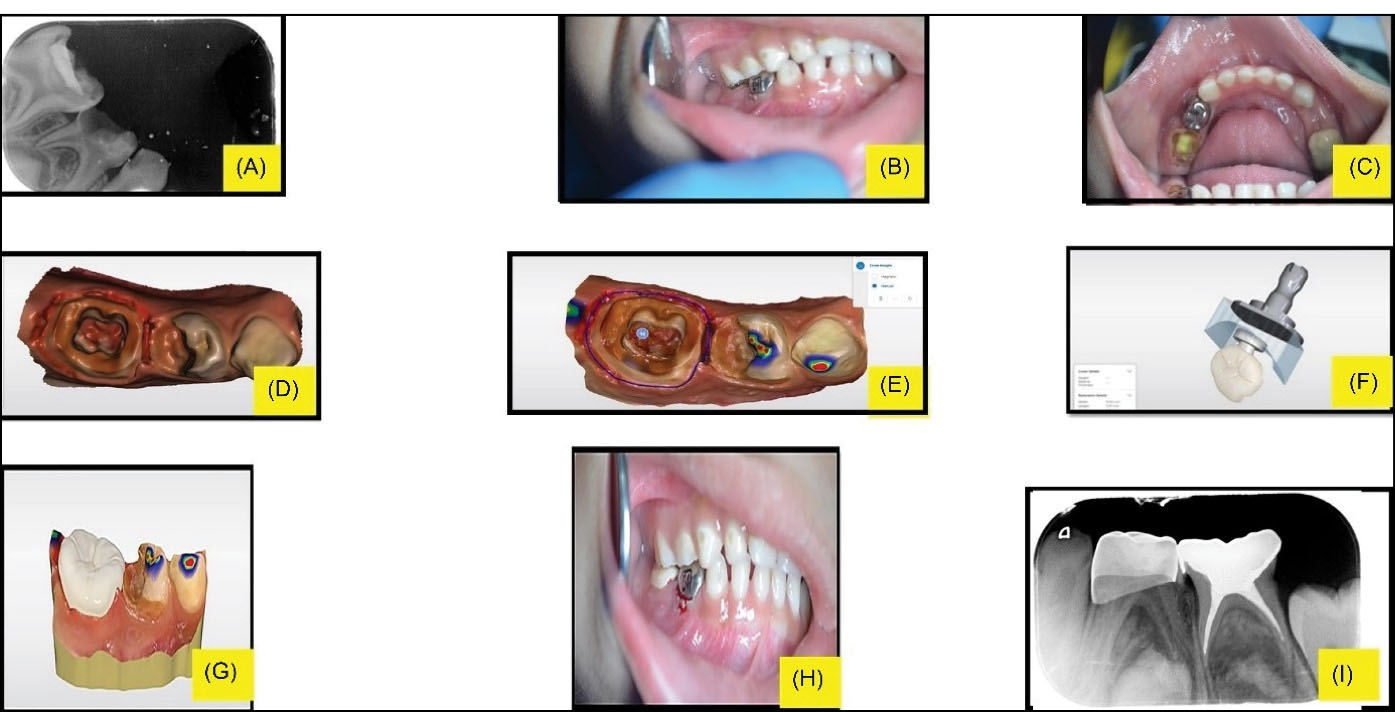
Figure 2.
(A) Pre-operative IOPA, (B) Pre-operative intraoral image, (C) Pulpectomy, (D) 3D Impression Image, (E) Drawing Margins in the 3D Model, (F) Block Manufacture, (G) 3D Digital Mockup, (H) Post Cementation, and (I) Post-operative IOPA. Abbreviation: IOPA, Intra-oral periapical.
.
(A) Pre-operative IOPA, (B) Pre-operative intraoral image, (C) Pulpectomy, (D) 3D Impression Image, (E) Drawing Margins in the 3D Model, (F) Block Manufacture, (G) 3D Digital Mockup, (H) Post Cementation, and (I) Post-operative IOPA. Abbreviation: IOPA, Intra-oral periapical.
The remaining tooth structure was not sufficient for crown preparation. We wanted to preserve 85 due to the age of the patient; otherwise, she would require a space maintainer or encounter mesial drift of permanent molars and occlusal disharmony later in life. The patient was also given silver diamine fluoride restoration followed by SSC on 84 (Patient’s 84 also had a disto-occlusal defect requiring a full coverage crown) which would further complicate the fabrication of the space maintainer on 84.
Therefore, we planned for chairside customized hybrid zirconium restoration, along with pulpectomy which provided an occlusal and functional overlay kind of permanent restoration for 85. The customized restoration on 85 was more conservative than a normal full-coverage crown. It incorporated an extension of extra restorative material on the underside of the restoration into the excavated pulp chamber following root canal therapy, taking advantage of the extra surface area afforded in this space on the interior aspect of the preparation, thereby sparing the external walls from needing as much tooth reduction.
As described in our first case, we also followed our exclusively altered plan for this case, along with NOIS for a pleasant experience to overcome her past dental experiences. The diagrammatic summary of our single-sitting treatment plan with CEREC workflow is illustrated in Figures 2B to 2H, yielding favorable results in less than one hour.
Case 3
In our third case, an 8-year-old boy came to our clinic with pus discharge and gross decay in the lower front tooth. Clinical and radiographic examinations demonstrated grossly decayed 83 with sinus formation. The decay primary structure of the tooth was lost and was insufficient for crown preparation. The preservation of the tooth was necessary considering the age of the patient.
Thus, we planned for chairside customized hybrid zirconium restoration, along with pulpectomy which provided an esthetic and functional overlay kind of permanent restoration. This restoration was more conservative than a normal full coverage crown and required minimal tooth preparation. Similar to our previous case, it incorporated an extension of extra restorative material on the underside of the restoration into the excavated pulp chamber following root canal therapy, providing anchorage to overlay without compromising the remaining tooth structure unlike conventional crown preparation for prefabricated crowns.
As described in our first case, we also followed our exclusive altered plan for this case, along with NOIS for a pleasant experience. The diagrammatic summary of our single sitting treatment plan with CEREC workflow is displayed in Figures 3A-F, providing favorable results in less than one hour similar to our previous case with happy and satisfied patients and parents.
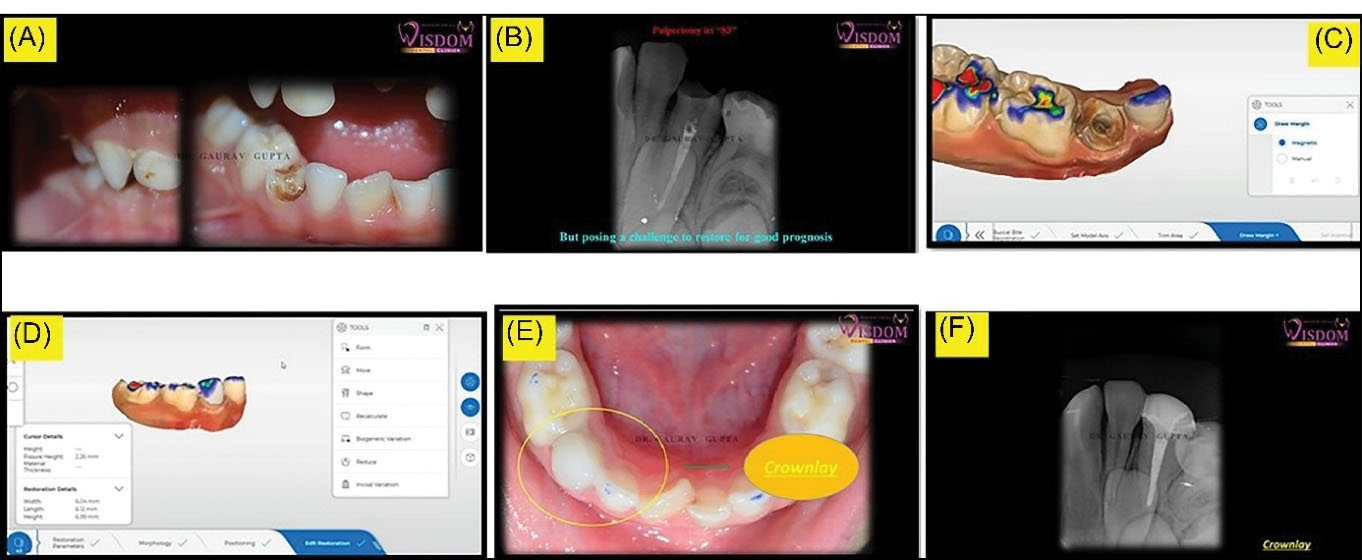
Figure 3.
(A) Grossly decayed primary mandibular canine, (B) Pre-op X-ray (C) Drawing margins, (D) 3D mock-up, (e) Post cementation, and (F) Post op X-ray.
.
(A) Grossly decayed primary mandibular canine, (B) Pre-op X-ray (C) Drawing margins, (D) 3D mock-up, (e) Post cementation, and (F) Post op X-ray.
As shown in our cases, we reconstituted not only the form, and function of primary teeth but also the esthetics with minimally invasive dentistry in single sitting with the help of CEREC workflow. The complete procedural steps are explained in form of a flowchart (Figure 4).
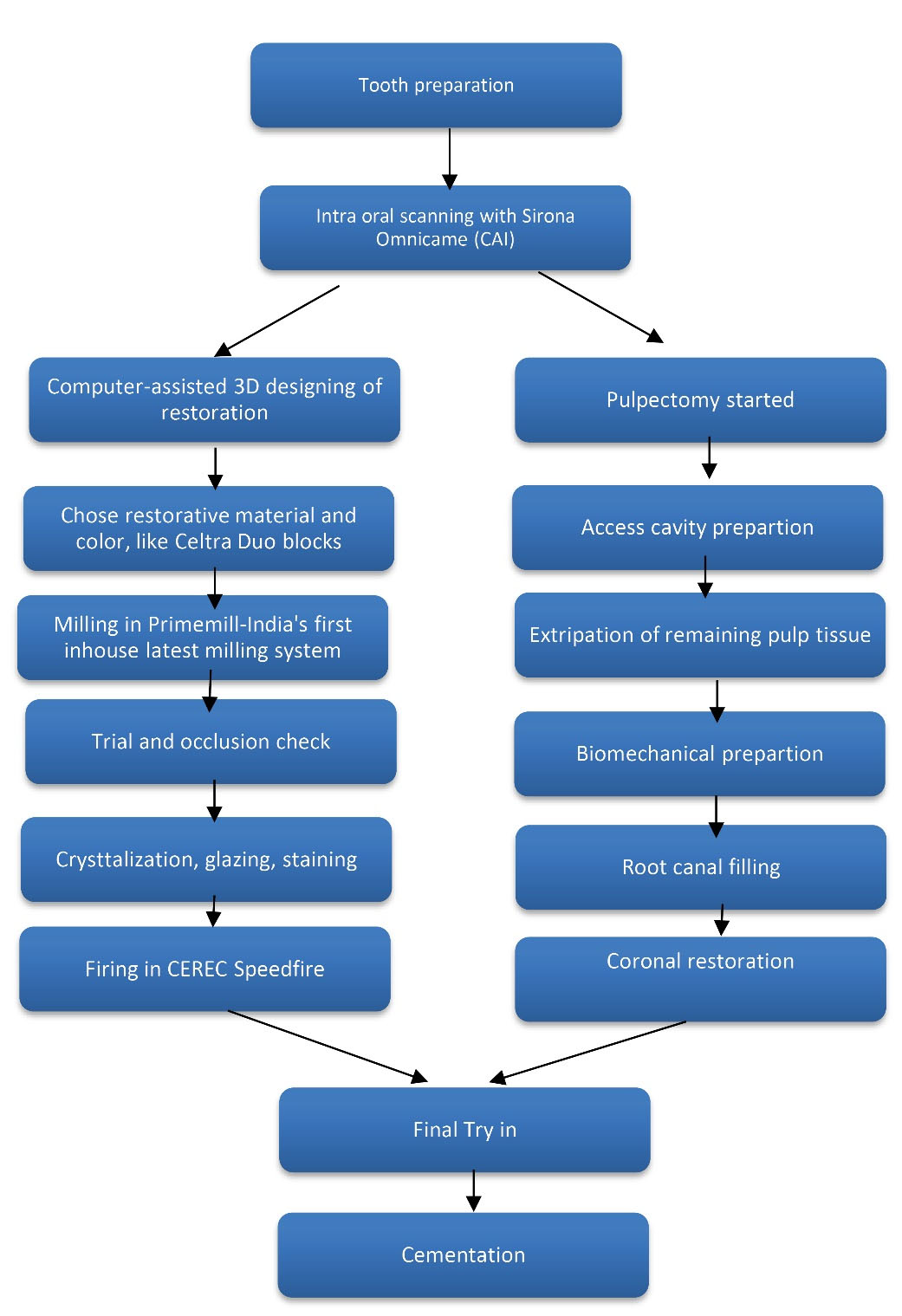
Figure 4.
Flowchart Showing Complete Procedural Steps. Note. CAI:Computer-aided impressions.
.
Flowchart Showing Complete Procedural Steps. Note. CAI:Computer-aided impressions.
Discussion
Over the past few years, the application of computer-aided impression systems in dentistry has grown tremendously and provided a substitute for traditional intraoral impression methods. 3D images obtained from intraoral scanning can be further processed and refined with the help of distinct software in almost all fields of dentistry. CAD/CAM technology facilitates the fabrication of high-quality restorations, customized as per every case’s requirement with precision, accuracy, and comfort of a single sitting. Since its evolution in the dental field in 1985 as the CEREC 1, this system has emerged through a series of software and hardware upgrades up to the CEREC 3D.
The CEREC 1 allowed for a limited 2D view of the scanned images and could fabricate only inlays for immediate cementation whereas the evolution of advanced computer technology over time has led to a 3D CEREC design program. 3D models can be prepared within minutes followed by scanning and can be evaluated immediately on the monitor screen for further treatment planning, leading to a more intuitive, convenient, and enriched quality chairside workflow in comparison to the conventional laboratory system.
CEREC workflow commenced with the digital recording and interpretation of intra-oral details. Consequently, there are two options for manufacturing restoration with CAD/CAM, either in a dental laboratory or directly chairside in clinic space (8). In the case of a dental laboratory, the dentist sends the digital record to the laboratory where the final restoration is mapped out virtually with the help of CAD software. Thereafter, the designed restoration is sent to a milling device followed by firing that produces the final prosthesis. When CEREC workflow and intra-oral scanner are installed in clinic space, the whole process of CAD/CAM will only take place in clinic space and can be accomplished in a single sitting. The dentist can execute the scanning, designing, milling, and firing process chairside (9). Simultaneously, the dentist can finish the pulpectomy procedure in pediatric cases to reduce chairside time and increase comfort for the patient.
The digital impression making technique is one of the benchmarks in this CEREC workflow since it yields good results with respect to the accuracy, precision, shade selection, and easiness to learn. It has been shown in multiple studies that digital workflow dispenses the restoration of equal fit and accuracy in a broad range of indications. Various studies have compared the time efficiency of digital 3D scanning over conventional impression methods, but only a few of them have compared the entire workflow (10). There is a requirement for new comparative studies in this field with the introduction of the latest CEREC software. The aim of our article was to portray the time efficiency and specificity of chairside workflow to fabricate hybrid restoration as per the need in comparison with a conventional treatment plan for single-unit restorations (prefabricated) in pediatric patients.
A milling machine installation in the clinic allows the insertion of customized final restoration within hours in a single sitting after a pulpectomy. CEREC Prime mill detains the next step forward and offers highly calibrated chairside dentistry. It manufactures extravagant chairside restoration easily and meticulously in a few minutes due to advanced digital technology.
There are a few stumbling blocks with this advanced technique, including the need for auxiliary training, challenges in scanning due to saliva flow and patient movement, and ultimately the high start-up cost of this system which may curb its installation in clinics.
Conclusions
The above-mentioned case and our clinical practice suggest that the CEREC chairside system is a useful tool for the clinician. The digital 3D impression, the software design, and the milling unit in the same office allow to produce highly aesthetic and reliable restorations in a single visit while improving patient acceptance and comfort with the procedures. It can be asserted that the aforementioned restorative treatment with digital CAD/CAM chairside workflow represents a valid alternative to rehabilitate this kind of pediatric patient because it is a safe, predictable, and personalized procedure; in addition, it is easier, faster, and cheaper than the traditional protocol in the long run.
Authors’ Contribution
The study was planned by Gaurav Gupta and D.K Gupta. The statistical analyses and interpretation of data were carried out by Priyanka Gupta and Parth Shah. Gaurav Gupta and Abhishek Khairwa contributed to the literature review. All the authors have read and approved the final manuscript.
Competing Interests
The authors declare that they have no conflict of interests.
Ethical Approval
Informed consent was obtained from the patients’ parents for publication of this report.
References
- Mourouzis P, Arhakis A, Tolidis K. Computer-aided design and manufacturing crown on primary molars: an innovative case report. Int J Clin Pediatr Dent 2019; 12(1):76-9. doi: 10.5005/jp-journals-10005-1591 [Crossref] [ Google Scholar]
- Kindelan SA, Day P, Nichol R, Willmott N, Fayle SA. UK National Clinical Guidelines in Paediatric Dentistry: stainless steel preformed crowns for primary molars. Int J Paediatr Dent 2008; 18 Suppl 1:20-8. doi: 10.1111/j.1365-263X.2008.00935.x [Crossref] [ Google Scholar]
- Randall RC. Preformed metal crowns for primary and permanent molar teeth: review of the literature. Pediatr Dent 2002; 24(5):489-500. [ Google Scholar]
- Seale NS. The use of stainless steel crowns. Pediatr Dent 2002; 24(5):501-5. [ Google Scholar]
- Ashima G, Sarabjot KB, Gauba K, Mittal HC. Zirconia crowns for rehabilitation of decayed primary incisors: an esthetic alternative. J Clin Pediatr Dent 2014; 39(1):18-22. doi: 10.17796/jcpd.39.1.t6725r5566u4330g [Crossref] [ Google Scholar]
- Lee JH. Guided tooth preparation for a pediatric zirconia crown. J Am Dent Assoc 2018;149(3):202-8.e2. 10.1016/j.adaj.2017.08.048.
- Collares K, Corrêa MB, Laske M, Kramer E, Reiss B, Moraes RR. A practice-based research network on the survival of ceramic inlay/onlay restorations. Dent Mater 2016; 32(5):687-94. doi: 10.1016/j.dental.2016.02.006 [Crossref] [ Google Scholar]
- Stromeyer S, Wiedemeier D, Mehl A, Ender A. Time efficiency of digitally and conventionally produced single-unit restorations. Dent J (Basel) 2021; 9(6):62. doi: 10.3390/dj9060062 [Crossref] [ Google Scholar]
- Beuer F, Schweiger J, Edelhoff D. Digital dentistry: an overview of recent developments for CAD/CAM generated restorations. Br Dent J 2008; 204(9):505-11. doi: 10.1038/sj.bdj.2008.350 [Crossref] [ Google Scholar]
- Joda T, Brägger U. Digital vs conventional implant prosthetic workflows: a cost/time analysis. Clin Oral Implants Res 2015; 26(12):1430-5. doi: 10.1111/clr.12476 [Crossref] [ Google Scholar]