Avicenna J Dent Res. 14(2):89-91.
doi: 10.34172/ajdr.2022.15
Case Series
Giant Cell Fibroma: A Report of Seven Cases
Soussan Irani 1  , Shokoofeh Jamshidi 1, Erfaneh Amini 2, * , Samaneh Vaziriamjad 3, Parya Atapour 2
, Shokoofeh Jamshidi 1, Erfaneh Amini 2, * , Samaneh Vaziriamjad 3, Parya Atapour 2
Author information:
1Dental Research Center, Oral & Maxillofacial Pathology Department, Dental Faculty, Hamadan University of Medical Sciences, Hamadan, Iran
2Postgraduate Student of Oral & Maxillofacial Pathology, Oral & Maxillofacial Pathology Department, Dental Faculty, Hamadan University of Medical Sciences, Hamadan, Iran
3Oral Medicine Department, Dental Faculty, Hamadan University of Medical Sciences, Hamadan, Iran
*
Corresponding author: Erfaneh Amini, Oral & Maxillofacial Pathology Department, Dental Faculty, Hamadan University of Medical Sciences, Shahid Fahmideh Blvd., Hamadan, Iran. Tel:+98 9368314585, Fax:+98 8138381085, Email:
erfanamin19@yahoo.co.uk
Abstract
The giant cell fibroma is a fibrous tumor with characteristic clinicopathologic features. It accounts for approximately 2% to 5% of all oral fibrous proliferations submitted for biopsy. It does not appear to have a clear etiology. In this article, we present seven cases of giant cell fibroma retrieved from the Archive of the Department of Oral and Maxillofacial Pathology, Dental Faculty, Hamadan University of Medical Sciences.
Keywords: Connective tissue, Etiology, Mouth diseases, Soft tissue, Maxillofacial
Copyright and License Information
© 2022 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Irani S, Jamshidi S, Amini E, Vaziriamjad S, Atapour P. Giant Cell Fibroma: A Report of Seven Cases. Avicenna J Dent Res. 2022; 14(2):89-91. doi:10.34172/ajdr.2022.15
Introduction
Weathers et al described the clinical and histopathologic features of giant cell fibroma in 1947 for the first time (1). Based on gender and age distribution, location, and histologic features, they separated it from the previously known entity “irritation fibroma”. It was designated as giant cell fibroma because of the presence of stellate fibroblasts with large mononuclear and multinucleated giant cells. Giant cell fibroma accounts for approximately 2% to 5% of all oral fibrous proliferations submitted for biopsy and about 1% of total biopsies (2,3). Clinically, giant cell fibroma usually presents as a solitary asymptomatic sessile or pedunculated nodule measuring about 0.5 to 1 cm with a pebbly surface. The surface can be smooth or even ulcerated due to trauma (4). It appears to be more common on the gingiva, followed by the tongue, buccal mucosa, and palate (2,3,5).
Case Presentation
Here, we present a report of seven cases of giant cell fibromas retrieved from the Archive of Department of Oral and Maxillofacial Pathology, Dental Faculty, Hamadan University of Medical Sciences from 2009 to mid-2021. There were five males and two females. The mean age of patients at the time of diagnosis was 33.9 ± 23.7 years. In our report, the lesion was mostly found on the gingiva (n = 3). The mean duration of the disease was 42.1 ± 37.9 months. The mean size of the lesions was 0.8 ± 0.26cm. Clinical differential diagnosis included irritation fibroma, squamous papilloma, mucocele, and fibroxanthoma. All demographic and clinical data of cases are summarized in Table 1. Figure 1A, B shows the clinical features.
Table 1.
Summary of Demographic and Clinical Data
|
No.
|
Gender
|
Age (y)
|
Location
|
Clinical Feature
|
Duration (months)
|
Size (cm)
|
| 1 |
F |
4 |
Gingiva (mandible) |
Sessile, papillary surface |
7 |
0.5 |
| 2 |
F |
34 |
Gingiva (maxilla) |
Sessile, smooth surface |
24 |
1.2 |
| 3 |
M |
47 |
Labial mucosa |
Pedunculated,smooth surface |
120 |
0.8 |
| 4 |
M |
23 |
Lower lip vermilion |
Sessile, smooth surface |
36 |
0.8 |
| 5 |
M |
16 |
Dorsum of tongue |
Pedunculated, smooth surface |
12 |
0.5 |
| 6 |
M |
36 |
Gingiva (maxilla) |
Pedunculated, papillary surface |
48 |
0.6 |
| 7 |
M |
77 |
Labial mucosa |
Sessile, smooth surface |
48 |
1 |
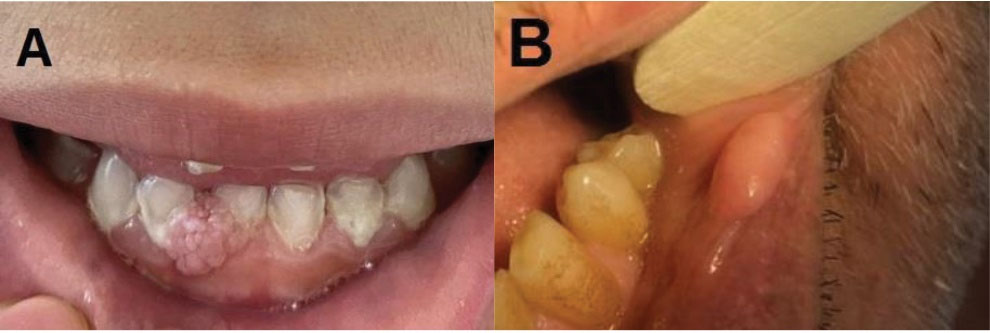
Figure 1.
Two Different Clinical Features of Giant Cell Fibroma.(A) Case No.1: The giant cell fibroma presents as a sessile nodule with a papillary surface. It was clinically diagnosed as squamous papilloma. (B) Case No. 7: The giant cell fibroma presents as a sessile nodule with a smooth surface on the labial mucosa. Clinically, it was diagnosed as irritation fibroma.
.
Two Different Clinical Features of Giant Cell Fibroma.(A) Case No.1: The giant cell fibroma presents as a sessile nodule with a papillary surface. It was clinically diagnosed as squamous papilloma. (B) Case No. 7: The giant cell fibroma presents as a sessile nodule with a smooth surface on the labial mucosa. Clinically, it was diagnosed as irritation fibroma.
Histopathologically, all cases showed a loosely arranged vascular fibrous connective tissue (Figure 2A). They were characterized by the presence of parakeratinized or orthokeratinized stratified squamous epithelium showing atrophy (number) with narrow and elongated rete ridges (number) (Figure 2B). In all cases, large stellate-shaped fibroblasts were seen in the connective tissue adjacent to the epithelium. The aforementioned cells showed distinct cell borders and a moderate amount of basophilic cytoplasm. Some of them contained 2-3 nuclei while some others had only one hyperchromatic nucleus or large vesicular nucleus with prominent nucleoli (Figure 2C). The diagnosis of giant cell fibroma was confirmed by microscopic examination. All tumors were treated by surgical excision.
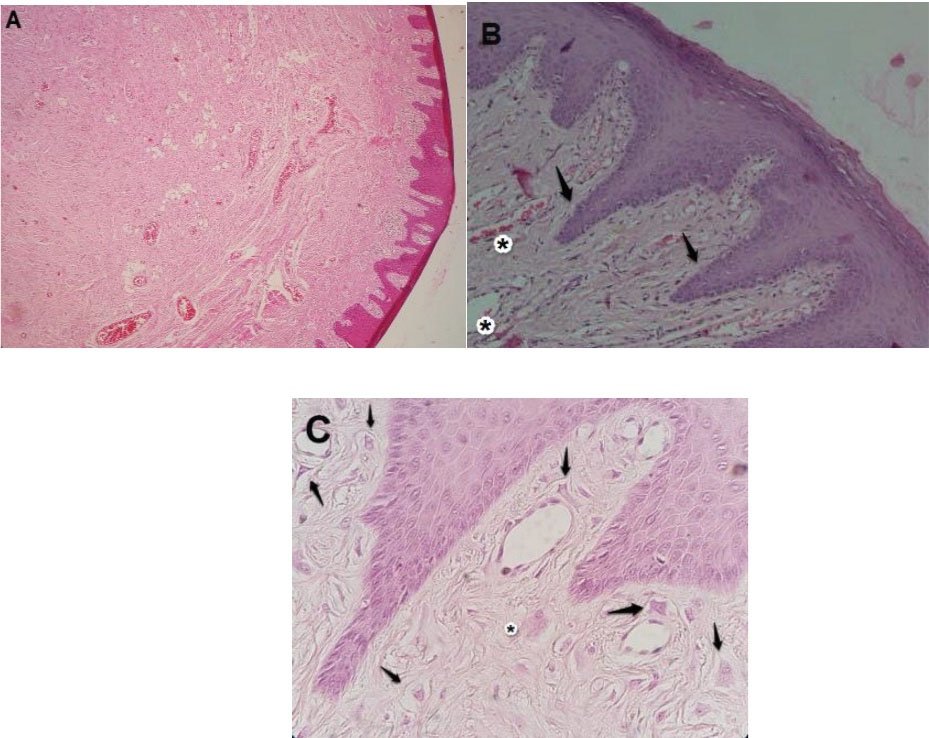
Figure 2.
Microphotographs of Giant Cell Fibroma. (A) Low power magnification shows a mass composed of loosely arranged vascular fibrous connective tissue. (B) Narrow and elongated rete ridges (→) are illustrated at medium power magnification. Underlying fibroconnective tissue demonstrates numerous blood vessels (*). (C) High power magnification indicates numerous stellate fibroblasts with large mononuclear (→) or multinuclear (*) giant cells within the superficial connective tissue.
.
Microphotographs of Giant Cell Fibroma. (A) Low power magnification shows a mass composed of loosely arranged vascular fibrous connective tissue. (B) Narrow and elongated rete ridges (→) are illustrated at medium power magnification. Underlying fibroconnective tissue demonstrates numerous blood vessels (*). (C) High power magnification indicates numerous stellate fibroblasts with large mononuclear (→) or multinuclear (*) giant cells within the superficial connective tissue.
Discussion
The giant cell fibroma is a rare non-neoplastic lesion of the oral mucosa. The etiology of this lesion remains controversial. Chronic irritation does not seem to have a role in the etiology of the lesion. Previous studies have suggested a slight female predilection. However, in this study, most of the cases were male (71%). The discrepancy may be attributed to the limited number of cases or genetic and racial differences. In the present study, the mean age of patients at the time of diagnosis was 33.9 ± 23.7 years. Previous studies have also demonstrated that the lesion usually occurs during the first three decades of life (4,6). In the current study, most of the cases were found on the gingiva (43%). Most published papers have also noticed that approximately 50% of all cases occur on the gingiva (5). Similar to the present study, several studies have indicated that the lesion is usually less than 1 cm in diameter (4,7). With regard to the origin of giant cell fibroma, immunohistochemical analysis has shown positive staining of stellate and multinucleated cells with vimentin and prolyl-4-hydrolase, suggesting that these cells might originate from fibroblasts (8,9). Ultrastructural studies have revealed numerous intracellular microfibrils supporting the fibroblastic nature of the giant cells in the lesion (10). Additionally, under light microscopy, stellate morphology, vesicular nuclei with prominent nucleoli, and basophilic cytoplasm due to high mRNA content are in favor of active fibroblast differentiation (11). Giant cell fibroma must be differentiated from irritation fibroma (cases with a smooth surface) and squamous papilloma (cases with a pebbly appearance). However, in contrast to giant cell fibroma, the extracellular matrix in irritation fibroma contains elastin (12). Clinically squamous papilloma occurs in older age and the common sites are the tongue, lip, and soft palate (10,11). There is also a tumor of the skin named fibrous papule of the nose, which shares the common histologic feature of a variable number of plump stellate or spindle-shaped multinucleated cells in the dermis. Besides, immunohistochemical staining with factor XIIIa can help to differentiate these two lesions. It has been suggested that dermal dendrocytes are the putative cells of origin (13). The treatment of choice was conservative surgery. Recurrence has rarely been reported (2).
Conclusions
Reactive fibrous hyperplastic lesions are common in the oral cavity and have some similarities in the clinical and histopathology features. Nonetheless, the giant cell fibroma is a fibrous tumor with distinctive clinicopathologic features. The etiology is not clear. Its prognosis is similar to that of irritation fibroma. The giant cell fibroma is treated by conservative surgical excision, and its recurrence is rare.
Authors’ Contribution
SI: Study conception and design, supervision, manuscript preparation and editing, SJ: data collection and interpretation of results, EA: data collection and interpretation of results, draft manuscript preparation, SV: data collection PA: data collection
Conflict of Interest Disclosures
The authors declare that they have no conflict of interests.
Ethical Statement
Demographic information, medical histories, test and laboratory results and other data were published without the release of any personal information.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Weathers DR, Callihan MD. Giant-cell fibroma. Oral Surg Oral Med Oral Pathol 1974; 37(3):374-84. doi: 10.1016/0030-4220(74)90110-8 [Crossref] [ Google Scholar]
- Magnusson BC, Rasmusson LG. The giant cell fibroma A review of 103 cases with immunohistochemical findings. Acta Odontol Scand 1995; 53(5):293-6. doi: 10.3109/00016359509005990 [Crossref] [ Google Scholar]
- Houston GD. The giant cell fibroma A review of 464 cases. Oral Surg Oral Med Oral Pathol 1982; 53(6):582-7. doi: 10.1016/0030-4220(82)90344-9 [Crossref] [ Google Scholar]
- Razi MR, Harith NS, Tahir NF, Selvaraj N. Congenital giant cell fibroma-a case report. Malays J Paediatr Child Health 2020; 26(1):21-8. [ Google Scholar]
- Reddy VK, Kumar N, Battepati P, Samyuktha L, Nanga SP. Giant cell fibroma in a paediatric patient: a rare case report. Case Rep Dent 2015; 2015:240374. doi: 10.1155/2015/240374 [Crossref] [ Google Scholar]
- Mello-Moura AC, Santos AM, Bonini GA, Del Conte Zardetto CG, Moura-Netto C, Wanderley MT. Giant cell fibroma in a two-year-old child. Case Rep Dent 2016; 2016:7058356. doi: 10.1155/2016/7058356 [Crossref] [ Google Scholar]
- Ramírez LA, Barrios BC. Giant cell fibroma Presentation of 122 cases. ADM 2021; 78(1):7-12. [ Google Scholar]
- Sanjeeta N, Nandini DB, Banerjee S, Devi PA. Giant cell fibroma: a case report with review of literature. J Med Radiol Pathol Surg 2018; 5(4):11-3. [ Google Scholar]
- Sabarinath B, Sivaramakrishnan M, Sivapathasundharam B. Giant cell fibroma: a clinicopathological study. J Oral Maxillofac Pathol 2012; 16(3):359-62. doi: 10.4103/0973-029x.102485 [Crossref] [ Google Scholar]
- Mathai M, Menaka V, Shunmugavelu K, Mugundan RN, Cynthia E, Vishnupriya V. Oral giant cell fibroma-expect the unexpected. Int J Clin Diagn Pathol 2021; 4(1):20-2. doi: 10.33545/pathol.2021.v4.i1a.318 [Crossref] [ Google Scholar]
- Sonalika WG, Sahu A, Deogade SC, Gupta P, Naitam D, Chansoria H. Giant cell fibroma of tongue: understanding the nature of an unusual histopathological entity. Case Rep Dent 2014; 2014:864512. doi: 10.1155/2014/864512 [Crossref] [ Google Scholar]
- Hegde U, Sreeshyla HS, Nitin P, Premalatatha BR, Shirona AP. Giant cell fibroma: report of two cases with histochemical nature of collagen fibers. Ann Rom Soc Cell Biol 2021; 25(4):19123-7. [ Google Scholar]
- Damman J, Biswas A. Fibrous papule: a histopathologic review. Am J Dermatopathol 2018; 40(8):551-60. doi: 10.1097/dad.0000000000001083 [Crossref] [ Google Scholar]