Avicenna J Dent Res. 12(2):63-67.
doi: 10.34172/ajdr.2020.13
Original Article
Iranian Dentists’ Knowledge of Post-exposure Prophylaxis Against HBV, HCV, and HIV
Maryam Amirchaghmaghi 1  , Hooman Keshavarz 2, * , Farid Haghdadi 3
, Hooman Keshavarz 2, * , Farid Haghdadi 3
Author information:
1Professor, Oral and Maxillofacial Diseases Research Center, Mashhad University of Medical Sciences, Mashhad, Iran.
2Assistant Professor, Department of Community Oral Health, School of Dentistry, Mashhad University of Medical Sciences, Mashhad, Iran.
3Student, Department of Endodontics, School of Dentistry, Mashhad University of Medical Sciences, Mashhad, Iran.
*
Correspondence to Hooman Keshavarz, Tel: +98-9153151074, Fax: +98-51-38829500, Email:
keshavarzh@mums.ac.ir
Abstract
Background: Dentists are at higher risk of exposure to blood-borne pathogens including HBV (hepatitis B virus), HCV (hepatitis C virus), and HIV (human immunodeficiency virus). The aim of this study was to evaluate the knowledge about post-exposure prophylaxis (PEP) against HBV/HCV/HIV among the general dentists working in Mashhad in 2016.
Methods: This cross-sectional study was conducted on a random sample (141 persons) of the general dentists working in Mashhad. The data gathering tool in this study was a self-administered questionnaire. The validity of the questionnaire was assessed by a group of relevant specialists. The reliability of the questionnaire was also tested by a test-retest method with a two-week interval. The agreement between the two steps (test and retest) was at least 70%, and Cronbach’s alpha was 0.74. The total score of each person’s knowledge ranged from -20 to +20. One-way analysis of variance (ANOVA) and t test were used for statistical analyses.
Results: Out of 141 dentists selected randomly, 101 subjects (69.3% male) participated in the study. The mean age of the participants was 42.3 years, And the mean duration of dental practice experience was 16.3 years. Regarding the mean age (P = 0.11), and the mean duration of dental practice experience (P = 0.12), there was no statistically significant difference between the two genders. The mean score of knowledge among the participants was -2.8, and there was no statistically significant difference between the two genders in this regard (P = 0.72).
Conclusions: This study indicated that the level of knowledge about PEP against HBV/HCV/HIV was very low among the general dentists working in Mashhad. Therefore, improving knowledge of general dentists working in Mashhad through appropriate educational interventions seems necessary.
Keywords: Dentists, HBV, HCV, HIV, Knowledge, Post exposure prophylaxis
Copyright and License Information
© 2020 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Citation: Amirchaghmaghi M, Keshavarz H, Haghdadi F. Iranian dentists’ knowledge of post-exposure prophylaxis against HBV, HCV, and HIV. Avicenna J Dent Res. 2020;12(2):63-67. doi: 10.34172/ajdr.2020.13.
Background
Highlights
-
Iranian dentists’ knowledge about post-exposure prophylaxis was very low.
-
There was no significant association between knowledge and gender.
-
There was no significant association between knowledge and practice experience.
Dentists are at risk of infection with many pathogenic microorganisms during their career (1). Oral cavity, where dental procedures take place, is an ideal environment for various infectious agents to grow, making dentists highly vulnerable to various pathogens (2). Infection transmission during dental procedures can occur through direct contact with saliva, blood, or air droplets, or indirectly via contaminated equipment such as dental surfaces or instruments (1)
Dentists are at higher risk of exposure to blood-borne pathogens including HBV (hepatitis B virus), HCV (hepatitis C virus), and HIV (human immunodeficiency virus). Regarding the dangers of these diseases for anyone, it is imperative that the standard of protection should be respected for all patients referred to dental clinics, regardless of the condition of their infection (3). The transmission of other infectious agents such as Mycobacterium spp., Pseudomonas spp., and herpes viruses is rarely reported, however there is also a higher risk of transmission through dental procedures (4).
Several centers, associations, and health care agencies such as CDC (Centers for Disease Control and Prevention), OSHA (Occupational Safety and Health Administration), and ADA (American Dental Association) have published guidelines for infection control (3,5,6). The practical implementation of these infection control strategies by dental personnel may be influenced by factors such as dentists' knowledge, socio-demographic and occupational variables, costs, and the availability of the needed equipment (7).
In Most studies in which dentists’ knowledge and attitudes toward infection control in different countries have been investigated, dentists had poor knowledge and performance regarding the standardized guidelines for infection control (7,8). Most studies on the knowledge of PEP (post-exposure prophylaxis), which is an important part of infection control, have also shown the low level of knowledge among health care workers (9-12). Unfortunately, few studies on the knowledge of PEP among Iranian dentists have been conducted (11,12).
Hence, the aim of this study was to evaluate the knowledge about PEP against HBV/HCV/HIV among the general dentists working in Mashhad city, Iran, in 2016.
Materials and Methods
This cross-sectional study was conducted on a random sample (141 persons) of the general dentists working in Mashhad (the second most populous city after Tehran in Iran). The systematic sampling method was applied for sampling using a list which was available in Mashhad Medical Council and contained information about the general dentists who had the professional permission for working in Mashhad. The list was ordered according to the dentists’ medical council codes and then, by randomly selecting a starting point, 141 persons were chosen at regular intervals (the appropriate interval was obtained by dividing the total number of dentists by 141). Having the professional permission for working in Mashhad was the only criterion for inclusion in the study. Exclusion criteria were unwillingness to participate in the study, and lack of professional activity at the time of the study. The data gathering tool in this study was a self-administered questionnaire. One of the authors (FH) had gone to the dental clinics and distributed the questionnaires among the selected dentists after providing them with the needed explanations about the study. This author had collected the completed questionnaires at the same meeting or another meeting.
The questionnaire used in this study consisted of two parts. The first part was composed of questions about demographic information (gender, age, dental practice experience, and current work place), as well as a question about the awareness of the availability of NGMOE (the National Guideline on Management of Occupational Exposure to HBV/HCV/HIV) (13). The second part of the questionnaire (20 five-choice questions) evaluated the dentists' knowledge of PEP against HBV/HCV/HIV. The source of the second part of the questionnaire was NGMOE. The validity of the questionnaire was assessed by a group of relevant specialists, and it was approved after implementation of the proposed amendments. The reliability of the questionnaire was also tested by the test-retest method with a two-week interval. Based on the results of the reliability assessment, the agreement between the answers in the two steps (test and retest) was at least 70%, and Cronbach's alpha was 0.74.
The total score of each person's knowledge (ranging from -20 to +20) was obtained by the summation of the scores assigned to his/her answers. In calculating the knowledge score, for each correct answer, a wrong answer, and the choice of "I do not know", scores +1, -1, and 0 were considered, respectively.
Statistical Analyses
Knowledge with a total score of less than 50% of the maximum score (less than 10) was considered “poor knowledge”. While individuals with the total score between 50% and 70% of the maximum score (between 10 and 14), and greater than or equal to 70% of the maximum score (greater than or equal to 14) had “medium knowledge” and “good knowledge”, respectively. The dentists were divided into three groups based on their dental practice experience: less than 10 years, 10 to 20 years, and more than or equal to 20 years. We used t test to compare the mean age and also the mean duration of dental practice experience between the two genders. T-test was also used to assess the relationship between the knowledge score and the awareness of the availability of NGMOE. One-way analysis of variance (ANOVA) and t test were used to compare the mean score of knowledge between the three groups of dental practice experience and the two genders, respectively. The data were analyzed with SPSS for Windows, version 16 (SPSS Inc., Chicago, IL, USA), and the statistical significance level was considered at P< 0.05.
Results
Out of 141 dentists selected randomly, 101 subjects (71.6%) participated in the study and completed the questionnaire. Out of the participants, 70 dentists (69.3%) were male. The mean age of the participants was 42.3 years (95% CI: 40.4, 44.1). The mean age of men was 43.3 years (95% CI: 40.9, 45.7), and the mean age of women was 40.0 years (95% CI: 37.5, 42.5). Regarding the mean age, there was no statistically significant difference between the two genders (P = 0.11).
The mean duration of dental practice experience among the participants was 16.3 years (95% CI: 14.6, 18.0). The mean duration of dental practice experience among men was 17.2 years (95% CI: 15.0, 19.3) while women had the mean duration of dental practice experience equal to 14.3 years (95% CI: 11.9, 16.8) (P = 0.12).
Moreover, majority of the participants (64.0%) were engaged in dentistry only in their offices (Figure 1). While majority of them (71.6%) were not aware of the availability of NGMOE.
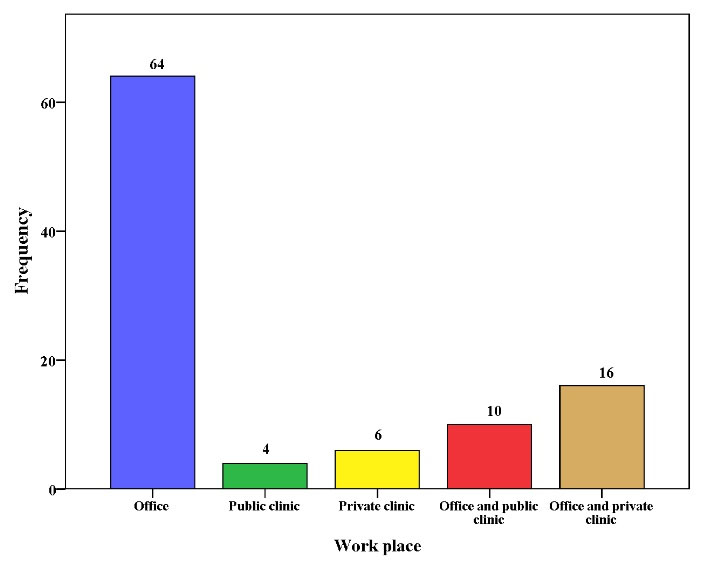
Figure 1.
Frequency of Dentists by Their Workplace (n=100 )
.
Frequency of Dentists by Their Workplace (n=100 )
The mean score of knowledge among the participants was -2.8 (95% CI: -3.5, -2.1). There was no statistically significant relationship between the mean score of knowledge and the awareness of the availability of NGMOE (P= 0.71). The lowest knowledge score was -12 while the highest was 7. Therefore, the knowledge score of all participants was considered as poor. The mean score of knowledge was -2.9 among men and -2.6 among women. There was no statistically significant difference between the two genders in this regard (P= 0.72; Figure 2).
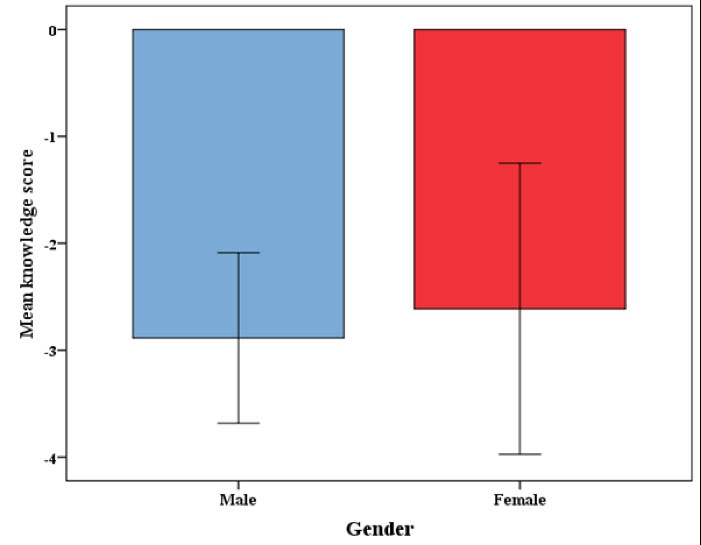
Figure 2.
Mean Knowledge Score by Gender. Error bars show 95% CI.
.
Mean Knowledge Score by Gender. Error bars show 95% CI.
The mean score of knowledge among the dentists with dental practice experience less than 10 years was -3.0, among those with dental practice experience of 10 to 20 years was -3.2, and among those with dental practice experience more than or equal to 20 years was -2.3. Regarding the mean score of knowledge, there was no statistically significant difference between the three groups of dental practice experience (P = 0.48; Figure 3).
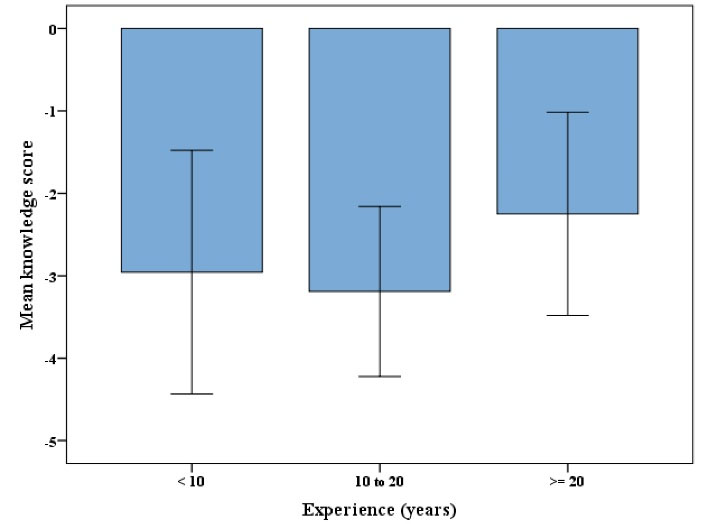
Figure 3.
Mean Knowledge Score by Experience. Error bars show 95% CI.
.
Mean Knowledge Score by Experience. Error bars show 95% CI.
Discussion
The rainbow is beautiful when the seven colors that make it up are next to each other. PEP also consists of seven steps, and its success requires careful implementation of all seven steps (Figure 4). There are very small discrepancies in different guidelines for PEP in different countries, depending on the structure of the health system and its facilities; while the general nature is almost the same. NGMOE, published by the Ministry of Health and Medical Education of the Islamic Republic of Iran, fully describes how to perform PEP against HBV/HCV/HIV (13).
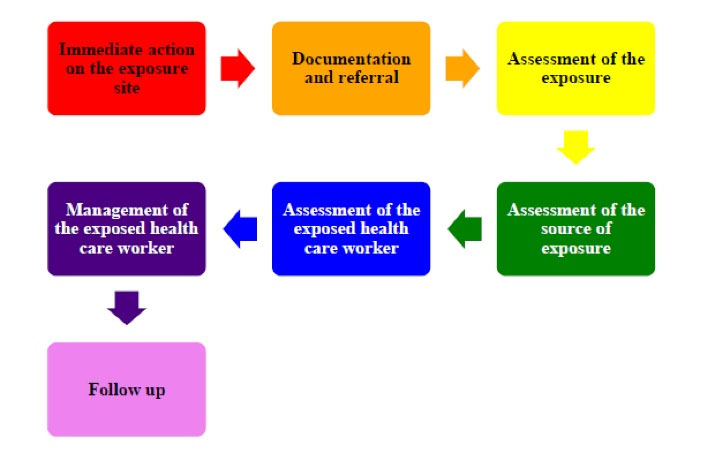
Figure 4.
The Seven Steps of Post-exposure Prophylaxis Against HBV/HCV/HIV.
.
The Seven Steps of Post-exposure Prophylaxis Against HBV/HCV/HIV.
Although previous studies have indicated that educational interventions can be effective in increasing health care workers’ knowledge about PEP (14,15), it is obvious that any planning in this field requires information on the current knowledge of the target group. The present study showed that the general dentists working in Mashhad city had very low level of knowledge about PEP against HBV/HCV/HIV.
The results of this study confirmed the results of previous studies, demonstrating poor knowledge about PEP against HBV/HCV/HIV among health care workers such as dentists (9-12,16-20). For example, Shaghaghian et al (11) in their study on dentists working in Shiraz showed that their knowledge about PEP was undesirable. They concluded that intervention to raise the dentists’ knowledge was necessary. However, contrary to the results presented in most available studies, some studies reported desirable level of knowledge about PEP among health care workers (21,22).
In this study, akin to the study of Shaghaghian et al (11), the mean score of knowledge among women was slightly higher compared to men. Indeed, this difference was not statistically significant in both studies. Conversely, in the study of Rafieian et al (12), the level of knowledge of male dentists about PEP was significantly higher than that of female dentists. Unfortunately, few studies have reported the relationship between gender and knowledge about PEP against HBV/HCV/HIV. While since knowledge about preventive efforts such as PEP may indicate the individual’s understanding of threatening risks, and this understanding may vary between genders, the study of the relationship between gender and the level of knowledge about PEP will not be useless.
In the study of Shaghaghian et al (11), the level of knowledge among dentists with dental practice experience less than 15 years was significantly higher than the level of knowledge among dentists with longer dental practice experience. In the mentioned study, authors suggested that the probable cause of this significant difference was the addition of an educational course on infection control to the curriculum of dentistry in the recent years. In contrast to that study, there was no statistically significant relationship between the level of knowledge about PEP, and dental practice experience in the present study. Perhaps the reason for the insignificant knowledge difference between the three groups of dental practice experience in the present study can be traced to various workshops on infection control which have been held specially for dentists during these years.
This study was conducted as a cross-sectional study using a questionnaire. Therefore, it had the innate limitations of cross-sectional studies, as well as the weaknesses of questionnaire studies. However, the authors attempted to minimize the impact of these limitations. For example, anonymous questionnaires and ensuring confidentiality could minimize the probability of not participating in the study and leaving questions without answers. Of course, considering the sample size and probability sampling in this study and the fact that Mashhad is the second most populous city in Iran, the results of this study can be compared to the results of a similar study at the national level.
Conclusions
This study indicated that the level of knowledge about PEP against HBV/HCV/HIV was very low among the general dentists working in Mashhad city. Considering the higher risk of occupational exposure to blood-borne pathogens including HBV, HCV, and HIV among dentists, this low level of knowledge about PEP efforts among the dentists in Mashhad may result in worrying consequences. Hence, improving knowledge of general dentists working in Mashhad city through appropriate educational interventions seems necessary.
Conflict of Interest Disclosures
The authors declare that they have no conflict of interests.
Acknowledgments
This article was originated from a graduate thesis (registered under #2846) at the Academic Affairs Office of School of Dentistry, Mashhad University of Medical Sciences.
Ethical Statement
This study was approved by the Ethics Committee of School of Dentistry, Mashhad University of Medical Sciences (Approval code: IR.MUMS.sd.REC.1394.33). Since the questionnaire used was anonymous and the selected dentists were completely free to decline participation in the study, the need for consent was waived by the Ethics Committee of School of Dentistry, Mashhad University of Medical Sciences.
Authors’ Contribution
The study was planned by MA and HK. Data collection was done by FH. Statistical analyses and interpretation of data were carried out by MA and HK. The manuscript was prepared by FH, and edited by MA and HK. All the authors have read and approved the final manuscript for submission.
Funding
This work was financially supported by Mashhad University of Medical Sciences [Grant No. 940353].
References
- Araujo MW, Andreana S. Risk and prevention of transmission of infectious diseases in dentistry. Quintessence Int 2002; 33(5):376-82. [ Google Scholar]
- Abreu MH, Lopes-Terra MC, Braz LF, Rímulo AL, Paiva SM, Pordeus IA. Attitudes and behavior of dental students concerning infection control rules: a study with a10-year interval. Braz Dent J 2009; 20(3):221-5. doi: 10.1590/s0103-64402009000300009 [Crossref] [ Google Scholar]
- Kohn WG, Collins AS, Cleveland JL, Harte JA, Eklund KJ, Malvitz DM. Guidelines for infection control in dental health-care settings--2003. MMWR Recomm Rep 2003; 52(RR-17):1-61. [ Google Scholar]
- Laheij AM, Kistler JO, Belibasakis GN, Välimaa H, de Soet JJ. Healthcare-associated viral and bacterial infections in dentistry. J Oral Microbiol 2012;4. 10.3402/jom.v4i0.17659.
- Occupational Safety and Health Administration (OSHA). Bloodborne Pathogens Exposure Control Plan and Guidance on Post-Exposure Evaluations for Federal OSHA Personnel. OSHA; 2020. [cited 25 April 2020]. Available from: https://www.osha.gov/enforcement/directives/cpl-02-02-077/.
- American Dental Association (ADA). The ADA Practical Guide to Effective Infection Control. Chicago, Ill: ADA; 2016.
- Dagher J, Sfeir C, Abdallah A, Majzoub Z. Infection control measures in private dental clinics in Lebanon. Int J Dent 2017; 2017:5057248. doi: 10.1155/2017/5057248 [Crossref] [ Google Scholar]
- Moradi Khanghahi B, Jamali Z, Pournaghi Azar F, Naghavi Behzad M, Azami-Aghdash S. Knowledge, attitude, practice, and status of infection control among Iranian dentists and dental students: a systematic review. J Dent Res Dent Clin Dent Prospects 2013; 7(2):55-60. doi: 10.5681/joddd.2013.010 [Crossref] [ Google Scholar]
- Kasat V, Saluja H, Ladda R, Sachdeva S, Somasundaram K, Gupta A. Knowledge, attitude and practices toward post exposure prophylaxis for human immunodeficiency virus among dental students in India. Ann Med Health Sci Res 2014; 4(4):543-8. doi: 10.4103/2141-9248.139308 [Crossref] [ Google Scholar]
- Owolabi RS, Alabi P, Ajayi S, Daniel O, Ogundiran A, Akande TM. Knowledge and practice of post-exposure prophylaxis (PEP) against HIV infection among health care providers in a tertiary hospital in Nigeria. J Int Assoc Physicians AIDS Care (Chic) 2012; 11(3):179-83. doi: 10.1177/1545109711401409 [Crossref] [ Google Scholar]
- Shaghaghian S, Pardis S, Mansoori Z. Knowledge, attitude and practice of dentists towards prophylaxis after exposure to blood and body fluids. Int J Occup Environ Med 2014; 5(3):146-54. [ Google Scholar]
- Rafieian N, Radi S, Hamian M, Torkaman M, Davoodi P. Post-exposure prophylaxis: knowledge and practice among general dental practitioners in Hamadan, Iran. Avicenna J Dent Res 2016; 8(4):e25963. doi: 10.17795/ajdr-25963 [Crossref] [ Google Scholar]
- Department of Health, Ministry of Health and Medical Education, Iran. National Guideline on Management of Occupational Exposure to HCV/HBV/HIV. [cited 25 April 2020] Available from: http://www.gums.ac.ir/Upload/Modules/Contents/asset77/HIV.pdf/.
- Dixit S, Khatri AK, Taneja G. Impact of educational intervention measures on knowledge regarding HIV/occupational exposure and post exposure prophylaxis among final year nursing students of a tertiary care hospital in central India. Online J Health Allied Sci 2009; 8(4):6. [ Google Scholar]
- Krishnan P, Dick F, Murphy E. The impact of educational interventions on primary health care workers’ knowledge of occupational exposure to blood or body fluids. Occup Med (Lond) 2007; 57(2):98-103. doi: 10.1093/occmed/kql126 [Crossref] [ Google Scholar]
- Kimaro L, Adinan J, Damian DJ, Njau B. Prevalence of occupational injuries and knowledge of availability and utilization of post exposure prophylaxis among health care workers in Singida District Council, Singida Region, Tanzania. PLoS One 2018; 13(10):e0201695. doi: 10.1371/journal.pone.0201695 [Crossref] [ Google Scholar]
- Mesfin YM, Kibret KT. Assessment of knowledge and practice towards hepatitis B among medical and health science students in Haramaya University, Ethiopia. PLoS One 2013; 8(11):e79642. doi: 10.1371/journal.pone.0079642 [Crossref] [ Google Scholar]
- Avachat S, Phalke DB, Dhumale GB. Awareness regarding pre-and postexposure prophylaxis for human immunodeficiency virus/acquired immunodeficiency syndrome among nursing students. Indian J Community Med 2007; 32(2):159. [ Google Scholar]
- Bilski B, Wysocki J. [The level of knowledge of post-exposure prohylaxis of blood-borne infections at the workplace observed in nurses]. Med Pr 2005; 56(5):375-8. [ Google Scholar]
- Chen MY, Fox EF, Rogers CA. Post-exposure prophylaxis for human immunodeficiency virus: knowledge and experience of junior doctors. Sex Transm Infect 2001; 77(6):444-5. doi: 10.1136/sti.77.6.444 [Crossref] [ Google Scholar]
- Bareki P, Tenego T. Assessment of knowledge, attitudes and practices of HIV post exposure prophylaxis among the doctors and nurses in Princess Marina Hospital, Gaborone: a cross-sectional study. Pan Afr Med J 2018; 30:233. doi: 10.11604/pamj.2018.30.233.10556 [Crossref] [ Google Scholar]
- Oche OM, Umar AS, Gana GJ, Okafoagu NC, Oladigbolu RA. Determinants of appropriate knowledge on human immunodeficiency virus postexposure prophylaxis among professional health-care workers in Sokoto, Nigeria. J Family Med Prim Care 2018; 7(2):340-5. doi: 10.4103/jfmpc.jfmpc_32_17 [Crossref] [ Google Scholar]