Avicenna J Dent Res. 12(2):68-70.
doi: 10.34172/ajdr.2020.14
Case Report
Eagle’s Syndrome: A Case Report of a 39-Year-Old Male
Farzaneh Pakdel 1  , Maryam Hossinpour Sarmadi 2, * , Salar Payahoo 3, Golchin Jabbari 4 , Farshad Javadzadeh 2
, Maryam Hossinpour Sarmadi 2, * , Salar Payahoo 3, Golchin Jabbari 4 , Farshad Javadzadeh 2
Author information:
1Assistant Professor, Department of Oral and Maxillofacial Medicine, Faculty of Dentistry, Tabriz University of Medical Sciences, Tabriz, East Azarbaijan, Iran.
2Resident, Department of Oral and Maxillofacial Medicine, Faculty of Dentistry, Tabriz University of Medical Sciences, Tabriz, East Azarbaijan, Iran.
3Assistant of Oral and Maxillofacial Radiology, Faculty of Dentistry, Urmia University of Medical Sciences, Urmia, West Azarbaijan, Iran.
4Assistant of Endodontics, Faculty of Dentistry, Urmia University of Medical Sciences, Urmia, West Azarbaijan, Iran.
Abstract
Ossifying stylohyoid ligament can be accidentally found in panoramic images. This status is occasionally asymptomatic. However, it is called the Eagle’s syndrome in the presence of symptoms such as pain in the pharynx, a foreign body sensation, tinnitus, or otalgia. The other symptoms may be reported due to the pressure on the carotid artery including migraines, aphasia, or vertigo and syncope, especially in turning head to the suffering side. The presented case was a thirty-nine-year-old man by a thick ossified stylohyoid ligament in both sides, along with five pseudoarticles and a record of the head and neckache, especially in cold weather.
Keywords: Eagle’s syndrome, Ossifying stylohyoid ligament, Pseudoarticle
Copyright and License Information
© 2020 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Citation: Pakdel F, Hosseinpour Sarmadi M, Payahoo S, Jabbari G, Javadzadeh F, Eagle’s syndrome: A case report of a 39-yearold male. Avicenna J Dent Res. 2020;12(2):68-70. doi: 10.34172/ajdr.2020.14.
Introduction
In the 17th century, Pietro Marchettis first observed the elongated styloid process related to the ossifying stylohyoid ligament in 1937, thus Eagle named it ‘Eagle’s syndrome’ (1,2). The mean length of the styloid process differed from 20 to 30 mm (3,4). The length above 25 mm was considered as an abnormal finding and only 4% of the patients manifested its symptoms (5-7).
The fracture of the elongated ossified stylohyoid ligament causes pain because the compresses or stretches surround sympathetic nerves causing them irritation in the arterial sheath (8), which was called ‘Stalalgia’ by Eagle (9).
In addition, Langlais et al classified the elongated styloid process and mineralized the styloid complex (10) into 3 types as follows:
-
Type I: Elongated and continuous process;
-
Type II: Having a single pseudo-articulation which seems to be elongated styloid;
-
Type III: Interrupted segment (with multiple pseudo-articulations). Nodular calcification or a complete ligament is observable.
This syndrome can happen in children although it usually occurs between the age of 30 and 50, which is due to a reduction in the elasticity of the ligament or the soft tissue of the styloid process by aging (3,11,12).
Eagle classified this syndrome into classic and carotid artery types. The classic type typically occurs after tonsillectomy and the scar of tonsillar fossa press or tension cranial nerves V, X, IX, and VII. The symptoms of the carotid artery type could be characterized by a foreign body sensation, recurrent pains that radiate into the ear and dysphasia, migraines, weakness in speech and visual symptoms or dizziness or even syncope, especially in turning head to the suffering side.
Bilateral headaches can happen if the internal carotid artery is under pressure. In external carotid artery involvement, pain is reported in the temporal and maxillary branches of this artery (5,13,14). Further, the compression of the internal carotid artery and the vagus nerve could be life-threatening (15). A rare case was reported about the mechanical force of an elongated styloid process which led to carotid dissection (16). Trauma, pharyngeal infections, or aging, by causing cervical vertebrae problems and shortening the neck and changing the styloid process direction, can occasionally create symptoms in patients who were previously without problems (9).
Considering the above-mentioned explanations, the aim of this case report was to describe an uncommon syndrome in order to assess the role of cone beam computed tomography (CBCT) in the diagnosis validation of Eagle’s syndrome and the evaluation of the styloid process position and then familiarize dentists with Eagle’s syndrome and its diagnostic work-up and treatment.
Case Report
The case of our study was a thirty-nine-year-old healthy man who was admitted to Tabriz Faculty of Dentistry for routine dental examinations. Intraoral and extraoral examinations were conducted, including a review of the past medical and dental procedures, dental carries, and the panoramic radiography checkup. An ossifying stylohyoid ligament was considered given his neck examinations and the panoramic image (Figure 1). Furthermore, CBCT was taken because of his implant needs, and he allowed the researchers to further study his stylohyoid ligament. The ossifying ligament continued from the styloid process to the hyoid bone in both sides and its width in the thickest part was 11.6 mm and 17.3 mm in the left and right sides, respectively (Figure 2). Moreover, one pseudo articulation was observed on both sides (Figure 3).

Figure 1.
Panoramic Radiography.
.
Panoramic Radiography.

Figure 2.
CBCT Radiography.
Note. CBCT: Cone beam computed tomography.
.
CBCT Radiography.
Note. CBCT: Cone beam computed tomography.
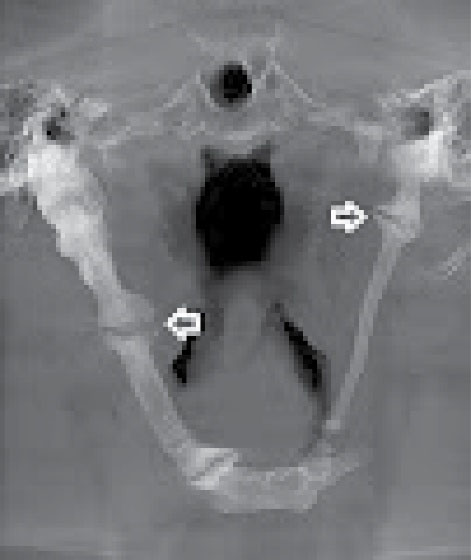
Figure 3.
Pseudoarticulation on Both Sides.
.
Pseudoarticulation on Both Sides.
The patient claimed to experience a headache and neckache which worsened in the cold weather although dental and family histories were none contributory. Based on the results, there was no associated history of fever or infection. The patient could not recollect any history of trauma. The patient had previously undergone a surgery while there was only a feeling of fullness and bilateral pain in exposure to cold weather.
Given the lack of many symptoms, the patient was in a normal physical state thus he performed no surgery. Additionally, he mentioned that he had used to that mild pain by taking pain killers such as gelofen. He was informed that he should refer to the Tabriz Faculty of Dentistry when observing an increase in the symptoms. Accordingly, we decided to follow him up.
Discussion
The palpation of palatine tonsils that causes pain is an important help for the disease diagnosis in addition to clinical history and radiographic evaluation (17).
A differential diagnosis could be temporomandibular disorders (18), glossopharyngeal and trigeminal neuralgia, temporal arteritis, salivary gland disease, chronic tonsillitis, laryngopharyngeal reflux, carotidynia, atypical migraine, otitis, and mastoiditis (5).
The temporomandibular disorder causes pain in the temporomandibular joint or the pre-auricular region, movements, joints noises and sounds, referred pain, headaches, tinnitus, earaches, vertigo or dizziness, hypoacusis, and hyperacusis (18).
This syndrome can be treated by surgical and nonsurgical procedures. There are two types of surgical methods, namely, intraoral and extraoral methods. However, the main disadvantage of intraoral method is the limited vision and the possibility of unwanted damages (19).
Conclusions
In general, patients with Eagle’s syndrome may have some symptoms that might seem confusing to physicians. On the other hand, panoramic images used in routine dental examinations can easily show the ossification of the ligament. Knowing the signs and symptoms of this syndrome and paying attention to panoramic graphy can be helpful for a quick diagnosis.
Notably, when facing symptoms such as neck pain relevant to ears or the sense of fullness in the throat, doctors and dentists should consider the probability of the above-mentioned syndrome, thus further study on graphs for routine examinations seems necessary in such cases.
Acknowledgements
We thank the patient for his cooperation in conducting this research
Ethical Statement
Consent was obtained from the patient.
Authors’ Contribution
All author’s contributed equally to this work
Funding
None.
References
- Dunn-Ryznyk LR, Kelly CW. Eagle syndrome: a rare cause of dysphagia and head and neck pain. JAAPA 2010; 23(12):28-31. [ Google Scholar]
- Eagle WW. Elongated styloid processes: report of two cases. Arch Otolaryngol 1937; 25(5):584-7. [ Google Scholar]
- Ilgüy M, Ilgüy D, Güler N, Bayirli G. Incidence of the type and calcification patterns in patients with elongated styloid process. J Int Med Res 2005; 33(1):96-102. doi: 10.1177/147323000503300110 [Crossref] [ Google Scholar]
- Lorman JG, Biggs JR. The Eagle syndrome. AJR Am J Roentgenol 1983; 140(5):881-2. doi: 10.2214/ajr.140.5.881 [Crossref] [ Google Scholar]
- Colby CC, Del Gaudio JM. Stylohyoid complex syndrome: a new diagnostic classification. Arch Otolaryngol Head Neck Surg 2011; 137(3):248-52. doi: 10.1001/archoto.2011.25 [Crossref] [ Google Scholar]
- Johnson GM, Rosdy NM, Horton SJ. Manual therapy assessment findings in patients diagnosed with Eagle’s syndrome: a case series. Man Ther 2011; 16(2):199-202. doi: 10.1016/j.math.2010.09.007 [Crossref] [ Google Scholar]
- Yavuz H, Caylakli F, Erkan AN, Ozluoglu LN. Modified intraoral approach for removal of an elongated styloid process. J Otolaryngol Head Neck Surg 2011; 40(1):86-90. [ Google Scholar]
- Ceylan A, Köybaşioğlu A, Celenk F, Yilmaz O, Uslu S. Surgical treatment of elongated styloid process: experience of 61 cases. Skull Base 2008; 18(5):289-95. doi: 10.1055/s-0028-1086057 [Crossref] [ Google Scholar]
- Yadav SP, Chanda R, Gera A, Yadav RK. Stylalgia: an Indian perspective. J Otolaryngol 2001; 30(5):304-6. doi: 10.2310/7070.2001.19604 [Crossref] [ Google Scholar]
- Langlais RP, Miles DA, Van Dis ML. Elongated and mineralized stylohyoid ligament complex: a proposed classification and report of a case of Eagle’s syndrome. Oral Surg Oral Med Oral Pathol 1986; 61(5):527-32. doi: 10.1016/0030-4220(86)90400-7 [Crossref] [ Google Scholar]
- Prasad KC, Kamath MP, Reddy KJ, Raju K, Agarwal S. Elongated styloid process (Eagle’s syndrome): a clinical study. J Oral Maxillofac Surg 2002; 60(2):171-5. doi: 10.1053/joms.2002.29814 [Crossref] [ Google Scholar]
- Quereshy FA, Gold ES, Arnold J, Powers MP. Eagle’s syndrome in an 11-year-old patient. J Oral Maxillofac Surg 2001; 59(1):94-7. doi: 10.1053/joms.2001.19302 [Crossref] [ Google Scholar]
- Costantinides F, Vidoni G, Bodin C, Di Lenarda R. Eagle’s syndrome: signs and symptoms. Cranio 2013; 31(1):56-60. doi: 10.1179/crn.2013.008 [Crossref] [ Google Scholar]
- White SC, Pharoah MJ. Oral Radiology-E-Book: Principles and Interpretation. Elsevier Health Sciences; 2014.
- Das S, Suhaimi FH, Othman F, Latiff AA. Anomalous styloid process and its clinical implications. Bratisl Lek Listy 2008; 109(1):31-3. [ Google Scholar]
- Subedi R, Dean R, Baronos S, Dhamoon A. Carotid artery dissection: a rare complication of Eagle syndrome. BMJ Case Rep 2017;2017. 10.1136/bcr-2016-218184.
- Mendelsohn AH, Berke GS, Chhetri DK. Heterogeneity in the clinical presentation of Eagle’s syndrome. Otolaryngol Head Neck Surg 2006; 134(3):389-93. doi: 10.1016/j.otohns.2005.10.046 [Crossref] [ Google Scholar]
- Thoenissen P, Bittermann G, Schmelzeisen R, Oshima T, Fretwurst T. Eagle’s syndrome - a non-perceived differential diagnosis of temporomandibular disorder. Int J Surg Case Rep 2015; 15:123-6. doi: 10.1016/j.ijscr.2015.08.036 [Crossref] [ Google Scholar]
- Németh O, Csáki G, Csadó K, Kivovics P. Case report of a 27-year-old patient suffering from Eagle’s syndrome. Oral Health Dent Manag 2010; 9(3):140-3. [ Google Scholar]