Avicenna J Dent Res. 15(3):109-115.
doi: 10.34172/ajdr.1673
Original Article
Impact of COVID-19 Pandemic on the Iranian Dentists’ Practice Patterns
Bahareh Tahani 1, *  , Soroush Talakesh 2 , Ali Foroughi 2 , Mohammad Pooyan Jadidfard 3
, Soroush Talakesh 2 , Ali Foroughi 2 , Mohammad Pooyan Jadidfard 3
Author information:
1Department of Oral Public Health, Dental Research Center, Dental Research Institute, Dental School, Isfahan University of Medical Sciences, Isfahan, Iran
2Dental Students Research Committee, Dental School, Isfahan University of Medical Sciences, Isfahan, Iran
3Department of Community Oral Health, Dental School, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Abstract
Background: The practice scheme of dentists during the coronavirus disease 19 (COVID-19) pandemic changed markedly around the world. The impacts of these changes on the economic concerns of dentists and the oral health of their patients have been the focus of some recent studies. This study aimed to assess probable alterations in the practice and patient mix of general dentists (GDs) and dental specialists in Isfahan, Iran during the COVID-19 outbreak.
Methods: This analytic cross-sectional study was performed among dentists during the COVID-19 pandemic (April-June 2021). A specific self-administrated questionnaire was designed, the validity and reliability of which were verified by calculating the content validity index and intra-class coefficients (test-re-test techniques), respectively. The questionnaire had 21 items in four sections, including demographic and work characteristics, probable changes in the practice scheme, composition of patients, and the type of the provided treatments. The collected data were analyzed using the SPSS software, descriptive and analytical analysis, including t-test, Chi-square, and ANOVA (α= 0.05).
Results: Overall, 152 general (response rate= 88%) and 171 specialist dentists were recruited, of whom 206 (63.8%) were males. In addition, 74% of the dentists, especially prosthodontists and restorative specialists, reduced the number of patients per working day (P<0.001). Further, 68.5% reported a decrease in the number of their elderly patients. Based on the results, 77% of the dentists reported an increase in tooth decay and hopeless teeth. Although extraction, emergency treatments, and extensive restorations were increased, prophylactic treatments and follow-ups represented a decline. The highest concern was reported to be about family health (7 out of 10). Finally, prosthodontists, endodontists, and surgery specialists reported the least use of these facilities (P<0.001).
Conclusions: An increase in the number of hopeless and decayed teeth, as well as an increase in emergency treatments (pain and abscesses) and a decrease in preventive care, confirms an untoward change in the dental practice pattern during the pandemic.
Keywords: COVID-19, Dental care, Dentists
Copyright and License Information
© 2023 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Tahani B, Talakesh S, Foroughi A, Jadidfard MP. Impact of COVID-19 pandemic on the iranian dentists’ practice patterns. Avicenna J Dent Res. 2023; 15(3):109-115. doi:10.34172/ajdr.1673
Background
Coronavirus disease 2019 (COVID-19) was identified as a public health emergency by the World Health Organization (WHO) on January 30, 2020; it was later declared a pandemic on March 11, 2020 (1). The cumulative number of COVID-19 cases has reached up to 373 million globally in January 2022, with more than 5.6 million deaths. In Iran, based on the last updated data of the WHO, about 7 million confirmed cases and about 145000 deaths were reported in the same time period (2). COVID-19 is caused by a new coronavirus called severe acute respiratory syndrome coronavirus 2 (SARS-CoV2), which is known for causing severe acute coronavirus syndrome. The SARS-CoV-2 virus could be transmitted through the respiratory system and indirect contact. Evidence suggests that this virus is present in saliva (3), transmissible by droplets and aerosols, even through asymptomatic patients (4,5).
Among all healthcare professionals, the highest risk of cross-infection is reported for dentists, dental assistants, and dental hygienists, as they are in close contact with patients, with exposure to saliva and aerosol (6). However, healthcare policies and regulations to control the transmission of COVID-19 in dental offices around the world have been different; during the pandemic time, private dental offices were closed in many regions of the world, and dental care was limited to urgencies and emergencies (7,8). In some European countries, elective treatment was not prohibited, and dentists had to evaluate whether to close their offices; they were allowed to choose the type of personal protection equipment (PPE) to apply (9).
Several published dental healthcare protocols recommended the prioritization of emergency and urgent dental care for issues such as swelling, pain, bleeding, dental trauma, and invasive infections (10). Virtual technology screening before scheduling dental visits and comprehensive exposure history to screen asymptomatic ones from infected people were the other recommendations in this regard (11). The changes in the practice scheme of dentists during the pandemic and the impacts of these changes on the economic concerns of dentists and the oral health of their patients have been the focus of some recent studies (12-14).
In Iran, especially in the first peak of the pandemic, there were highly emphasized recommendations to postpone elective dental care. The guidelines for PPE were established soon after the pandemic as well. However, there are few comprehensive studies assessing the effects of the pandemic on dentists’ practice scheme and their patient mix. Therefore, this study sought to assess different aspects of practice changes and concerns during COVID-19 pandemic era among general dentists (GDs) and specialists in Iran.
Materials and Methods
This analytical cross-sectional study was conducted among general and specialist dentists in Isfahan, from April to June 2021.
Sample Size
Based on another similar study (12) that demonstrated a 70% decrease in the provision of dental care during the pandemic, considering a 7% minimal difference and a 95% confidence interval (CI), the sample size was calculated to be 171 GDs. According to the limited number of specialists, they were recruited as a consensus. The convenience sampling method was applied by using an electronic survey.
Data Collection Tool
To design a comprehensive questionnaire, as the first step, some individual qualitative semi-structured interviews were arranged with GDs and specialists. The interviews were based on the 6-step protocol of Morrison (15), which included determining the aim, design, and implementation. The aim included declaring the proposed changes in the pattern of care and the patient mix in dental visits during the COVID-19 pandemic. Moreover, the design encompassed considering the structure and context of the interviews, applying a purposive sampling method with 10 participants, including 8 specialists working in endodontics, Oro-facial surgery, restoration, prosthetics, pediatrics, orthodontics and periodontics departments at Isfahan Dental School and 2 GDs, and continuing the interviews until reaching the saturation. In this step, individual interviews with the participants in their private rooms were conducted after getting informed consent. Three open-ended questions were then asked, including whether the COVID-19 pandemic had changed their pattern of practice in terms of work days or work hours. The other related questions were about whether they had made any changes in the care types they used to provide and whether and how the patient mix of their visitors had changed during the pandemic.
In step 4 of the protocol, all of them were recorded to document the interviews; shortly after the interview, they were transferred to scripts. In steps 5 and 6, the scripts were analyzed by BT, AF, and ST, separately, and a consensus was gained in meetings to outline the main themes. Finally, based on the interviews with 37 participants and a complimentary literature review (16,17), some questions were designed about changes in the scheme of practice and patient mix. The scales of these questions were based on the interviews.
Study Design
The proposed questionnaire had four sections, including demographics (age and gender), work experience characteristics (type and place), probable changes in the work hours, in the practice scheme, and in patient mix. To assure the validity of the final questionnaire, it was given to 10 faculty members from different disciplines; according to the Waltz and Bausell (18) technique, the relevancy of the questions was scored from completely not relevant (1 point) to completely relevant (4 points). The content validity index (CVI) was then calculated by dividing the frequency of the scores of 3 and 4 for each question by the total number of the panel of experts. According to the Lawshe table (19), the cut-off point of 0.6 was considered the minimum acceptable CVI mean, and 3 questions were eliminated accordingly. To assess the reliability of the questionnaire, it was given to about 20 dentists; after one month, they were asked to refill the questionnaire (test-re-test), and the intra-class coefficient (20) was computed for each question. Two other questions in the patient mix gained scores lower than 0.6 and were eliminated accordingly.
The final questionnaire had 4 demographic and work experience questions, 8 main questions in the practice scheme section, 5 main questions in the patient-mix section, and 1 question to assess the degree of self-reported concerns of dentists regarding the health of themselves and their family and oral health of their patients. Additionally, it included 1 question to check the proposed changes in dental care tariffs and 2 questions about the application of tele-dentistry during the pandemic. The final electronic questionnaire was developed and distributed among general and special dentists working in Isfahan through the professional Telegram and WhatsApp channels. Reminders were sent every three days.
Statistical Analysis
The gathered data were fed into SPSS, version 26 (IBM SPSS Statistics for Windows, Version 22.0.; IBM Corp). Descriptive analysis, figures, and tables were then used to summarize the results. T-test, ANOVA, and chi-square were also applied to compare the results based on the demographic characteristics (α = .05).
Results
Overall, 152 valid and complete questionnaires of GDs (response rate = 88%) and 171 questionnaires from specialists were gained after 3 months of sampling. Totally, 63.8 participants (n = 206) were males. In addition, 30% (n = 94) and 37% were working just in clinics and private offices, respectively, and 33% (n = 106) were working in both places. The mean age of the participants and the mean work experience were 40.3 ± 10.9 (25-75 years old) and 13.5 ± 9.8 years (1-40), respectively.
The responses to the questions about the changes in the practice scheme are shown in Figure 1. Accordingly, about one-third (103) of the dentists reported to have decreased their working days per week and the hours per working day. Further, 74% (237) reported to have assigned fewer patients per working day. Prosthodontics and GDs had decreased their working days more frequently (Chi-square = 47.4, P < 0.001). The least changes were reported by orthodontics.
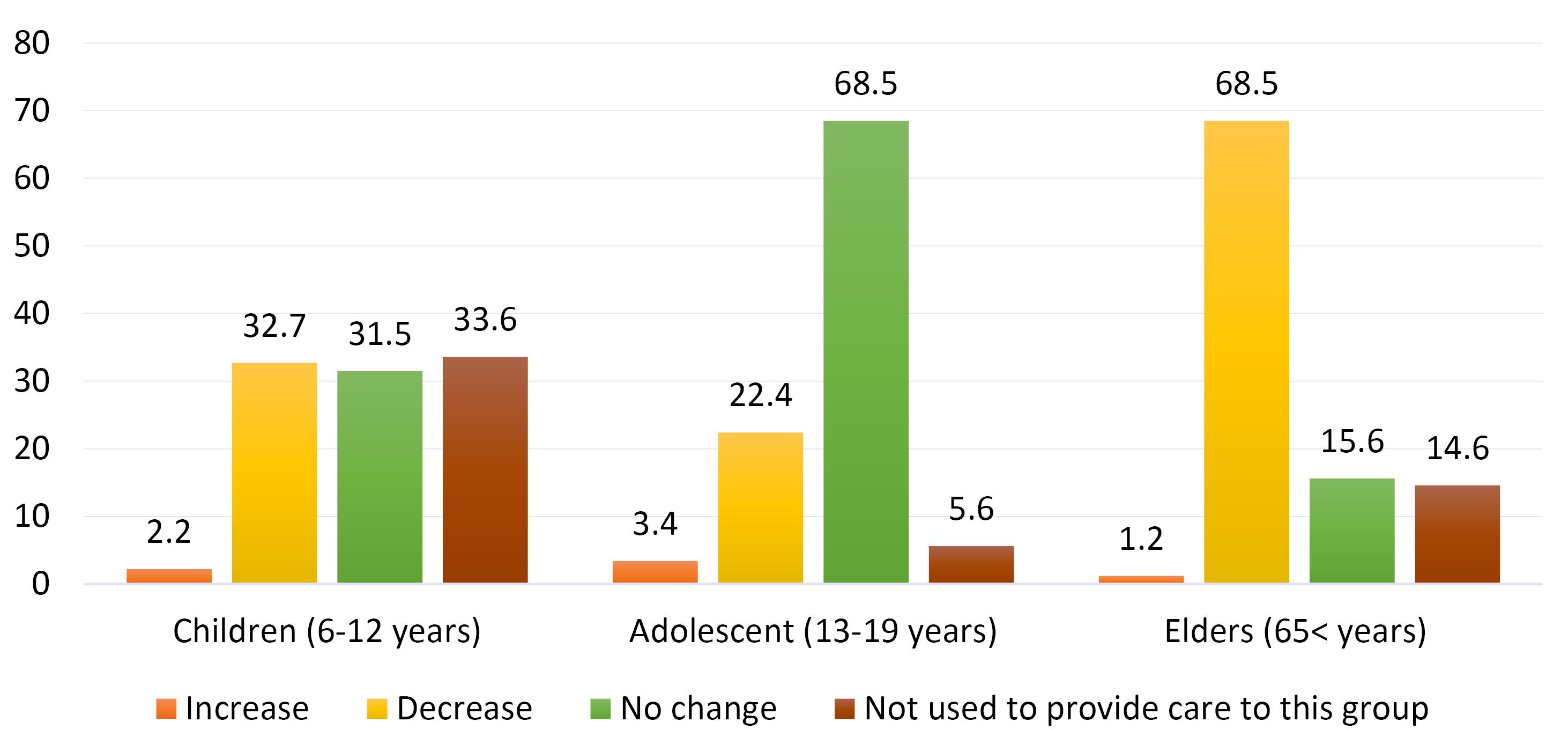
Figure 1.
The Reported Changes in the Practice Scheme by Participated Dentists.
.
The Reported Changes in the Practice Scheme by Participated Dentists.
The main reasons for the decrease in the working hours per day were the necessity of following the COVID-19 protection guidelines (82.9% = 265) and the fatigue and stress according to wearing PPEs (67.7% = 216). About 43% of the participants also mentioned the decrease in the visited patients as a reason. As regards the reasons for accepting fewer patients per working day, 58.6% ( = 188) reported the allocation of more time between patients to allow the reduction or clean up the probable air and surface contaminations more seriously.
Regarding the duration of the complete work lockdown, for the first peak (March-May, 2020), the mean weeks were 8.4 ± 7.4, and about 4% of the participants reported not to have closed their offices. The most frequent duration (in 36% of the cases) reported by dentists was 8 weeks. For the second (August-September, 2020) and third (November, 2020) peaks, the mean weeks of lockdown were similarly 1.1 ± 2.4, and about 60% reported not to have closed their offices.
As regards the patient-mix section, changes in the age group of the visiting patients are illustrated in Figure 2. The decrease in the number of visiting elders and children was reported to be about 70% and 30% of the dentists, respectively.
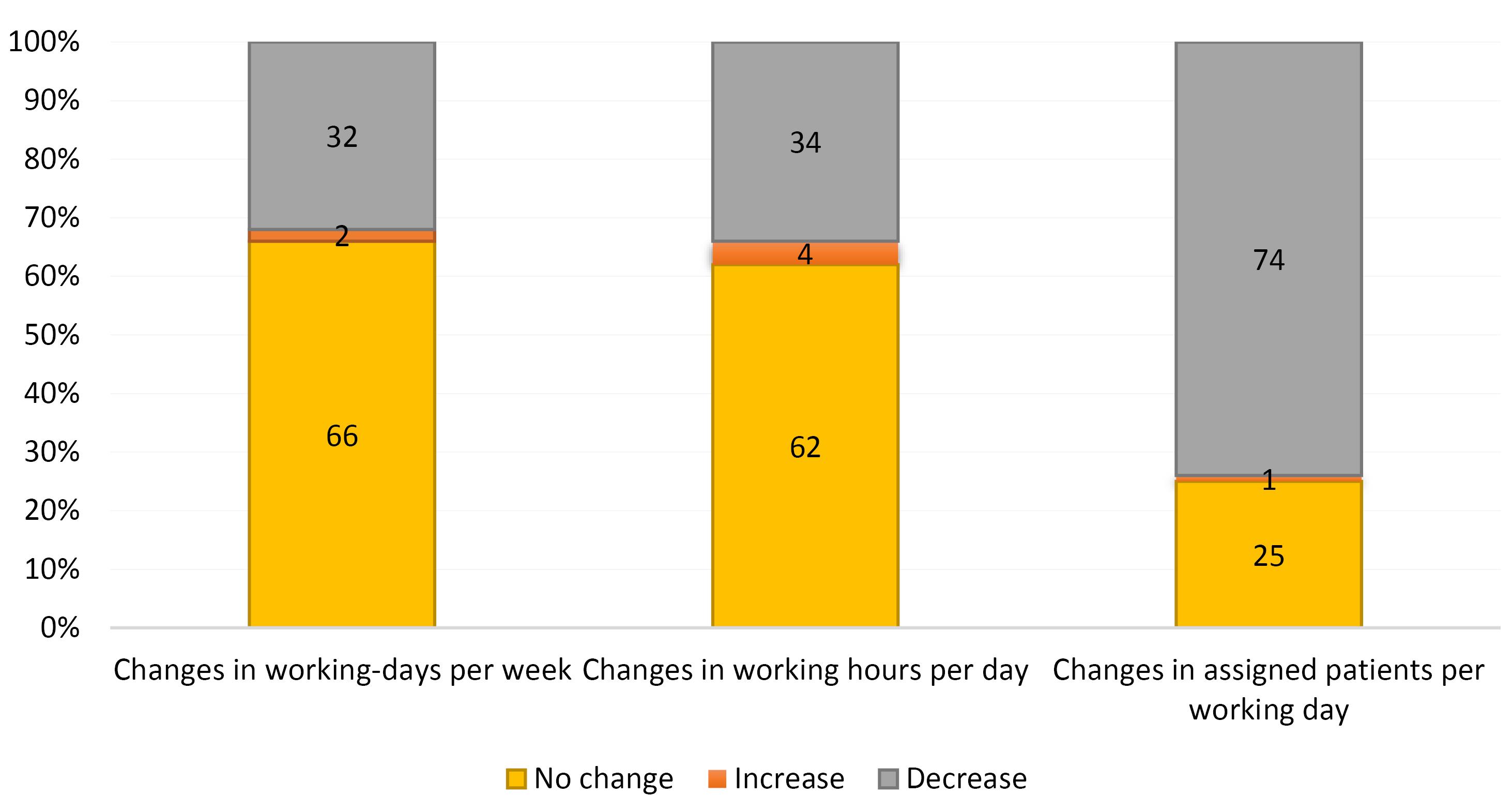
Figure 2.
Changes in the Visiting Patients Based on Their Age-group Reported by the Participated Dentists.
.
Changes in the Visiting Patients Based on Their Age-group Reported by the Participated Dentists.
With regard to the question of whether dentists believed any changes in the oral health status of their patients had occurred during the COVID pandemic, about 70% reported an increase in dental caries and the number of hopeless teeth. In addition, 46.9% of dentists believed in decreased oral hygiene behaviors among their regular patients. Although the status of parafunction behaviors (bruxism and clinching) and temporomandibular disorders was not assessed by about one-half of the participants, a 30% increase was reported by others who used to check these problems in their patients.
To find out the changes in the provided care during the pandemic, they were categorized into four groups (Figure 3), including surgical treatments (extractions, elective, and esthetic surgeries) and root canal therapies (emergency care, trauma management, pulpotomy of permanent teeth, re-treatments, and retrograde surgeries). The other groups were restorative treatments (flings, reconstructions, partial and complete prosthesis, and crowns), periodontal treatments (prophylaxis including scaling and root planning, and surgeries), and pediatric treatments.
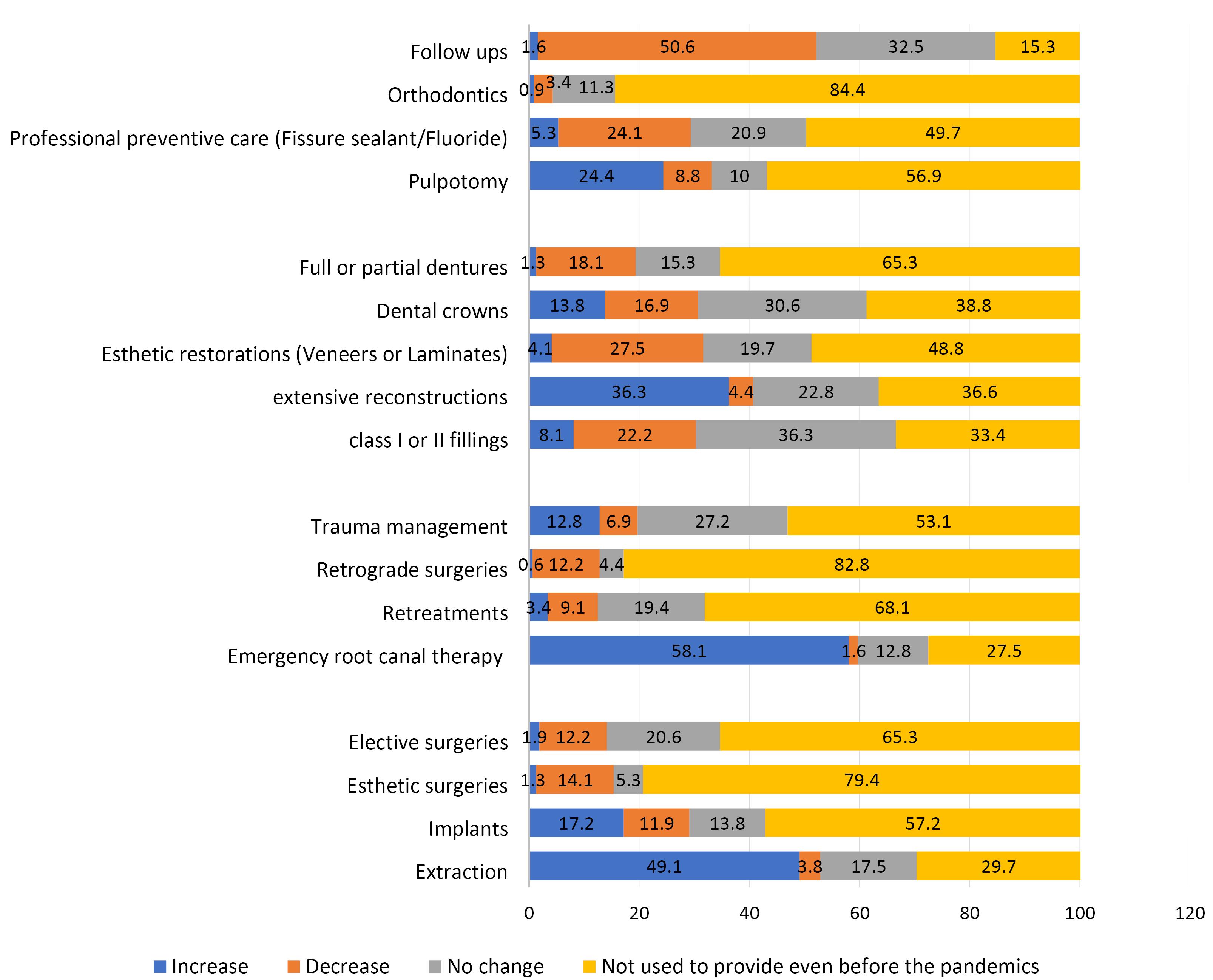
Figure 3.
Changes in the Type of Provided Care During Pandemic Reported by the Participated Dentists.
.
Changes in the Type of Provided Care During Pandemic Reported by the Participated Dentists.
Regarding surgical care, about 49% of dentists reported that the rate of extraction had increased during the pandemic (hopeless and borderline teeth). Regarding the root canal therapies, 58% of the dentists reported an increase in emergency care; moreover, of about 50% who used to manage trauma, one-third reported an increase in the rate of the visited people. As regards the restorative treatments, about one-third of the dentists reported to have increased the frequency of reconstructive restorations (extended restorations). Based on the self-report of dentists, a 47% decrease was found in scaling and root planning treatments. Concerning pediatric and orthodontic treatments, 24% of the dentists reported a decrease in professional preventive care, including fissure sealant and fluoride therapy. Among orthodontic treatments, a 50% decrease was detected in the follow-up appointments.
The changes in the provision of surgical care among GDs, Oro-maxillofacial surgeons, periodontics, and pediatrics who used to provide such care were almost similar, and the rate of the extraction of hopeless and borderline teeth increased, especially among pediatrics (87%).
As part of changes in the practice scheme regarding the PPE, it was revealed that 33% (106) of the dentists had increased their tariffs to cover the costs of PPEs, and 93.4% (295) had improved the ventilation status of their setting.
The mean self-reported concerns regarding the oral health status of patients and income are presented in Table 1. Post hoc Tukey’s analysis also demonstrated that GDs had higher income concerns as compared with endodontics (P < 0.001) and periodontics (P = 0.01). Additionally, the mean concern about the oral health of patients was significantly higher among GDs compared with others, especially endodontics (P < 0.001). The mean concern about the health status of the family was 7.7 ± 2. Regarding teledentistry facilities, while 34.2% (108) never used them, 27.5% (87) reported the application of virtual settings for the provision of tele-diagnose or tele-consultant to their patients. The most used stings were WhatsApp (91.2%) and Instagram (69.8%).
Table 1.
Mean and Standard Deviation of Dentists’ Concerns Regarding the Economic and Oral Health Effects of the Pandemic
|
|
Frequency
|
Concerns about the effect of the pandemic on dentists’ income
|
Concerns about the effect of the Pandemic on oral health status of patients
|
| General Dentists |
151 |
7.42±2.3 |
6.38±2.7 |
| Specialists |
|
|
|
| Pediatrics |
15 |
6.47±2.5 |
6±2.2 |
| Orthodontics |
27 |
6.48 ±2.2 |
5.8±1.5 |
| Maxillofacial Surgeons |
25 |
6.28±1.6 |
5.72±2.1 |
| Periodontics |
20 |
6.45±3 |
4.2±1.9 |
| Endodontics |
22 |
6.82±3.3 |
3.64±3.1 |
| Dental Restorations |
25 |
7.24±3.1 |
4.92±2.8 |
| Prosthodontics |
21 |
7.10±1.6 |
6.29±1.6 |
| Total |
306 |
5.7±2.8 |
6.01±2.3 |
Discussion
According to our study, the fear of cross-infection may have led to the increased cancellation of appointments, especially among elderly patients. In the study performed by Moharrami et al (21) in the United States, there was also a noticeable decrease in the rate of dental visits, especially among older patients. This lack of referral and postponement of necessary and timely treatments could have probably complicated the treatments, resulting in the increased number of hopeless teeth. Most dentists in our study reported that tooth extraction was extremely higher than before. The result of the study conducted by Ball et al (22) in the United Kingdom, also represented a marked increase in extraction as compared to the other dental treatments from April to May 2020. This obvious and bold change was likely to increase the burden of unnecessary edentulousness among different populations. However, to prove this claim, cohort population studies are necessary.
In addition, with regard to the results of our study, there was a marked decrease in the provision of preventive treatments such as fluoride and sealant therapy and initial non-extended restorations. Using health insurance records, Schwendicke et al (12) also concluded that preventive care had decreased by 80% during the pandemic. This reduction of conservative restorations and preventive measures, as well as the increase in the patients’ demand for extraction and endodontic treatments, might have led to pushing away from the principles of minimally invasive dentistry (23).
The findings of our study demonstrated that referring to dentists during the pandemic period was more for emergency treatments, including pain relief and dental abscess management. In a similar study conducted in Vancouver, Canada, during the COVID-19 pandemic, Tong et al (24) also found that dental infection, severe pain, and trauma were the most common reasons for patients to visit a dentist. Similarly, in the study conducted by Carter et al (25) in Britain, the most common concern presented by the patients in telephone-based consultations was receiving pain relief drugs. Ju-Hui Wu et al also reported that pulp disease had increased as compared to the time periods before the pandemic in Taiwan (26). In the study by Moharrami et al (21), the frequency of dental infection visits was also higher than before.
Most dentists in our study reported to have visited fewer patients per working day mostly due to the longer time intervals between patients to comply with PPE protocols. In a study by Ahmadi et al (27) in Iran, 95% of dentists changed their working hours. In our study, almost all dentists [95.7%] closed their offices completely upon the first peak of the disease (March 2020, to May 2020). However, this rate was decreased during the peak of the second and third waves. In a study by Faccini et al (28) in Brazil, 75% of dentists closed their offices during the first wave or limited their care only to emergency treatment. The findings of a study by Kranz et al (29) in the United States indicated that 97% of dentists closed their offices by April 6, 2020 [the first peak] or underwent emergency treatment only; however, by September 7, 2020 [second peak], 99% of the dentists did their routine work. It seems, therefore, that the fear of COVID-19 and aerosol has led to a reduction in working hours per day, the number of working days, and the number of patients per shift (the maximum decrease in the number of patients per working day was recorded by the prosthetics and restorative specialists who were involved in the exposure to aerosols at massive quantities).
Dentists’ concerns increased during the pandemic. In our study, the greatest concern was due to the impact of the pandemic on personal and family health. Women, in particular, were significantly more concerned about this issue. In the study conducted by Faccini et al (28), the average level of dentists’ concern about the impact of pandemics on their work was 9.03 out of 10, and the average level of dentists’ concern about the impact of pandemics on patients’ oral health was 8.09, while it was 6.01 in our study.
In our study, almost all dentists used PPE and followed environmental and personal protocols more rigorously. In a study performed by Ahmadi et al in Iran, 97% of dentists increased the use of PPE, but only 11% of them in government centers received subside for this overloading cost. Moreover, 97% of dentists reported a decrease in income, and 57% of them believed that they would face economic problems in the future (27). In our study, only one-third of the dentists increased the tariffs due to the use of protective items. The average level of concern about income reduction [out of 10] in our study was 6.01. Figure 4 summarizes the proposed effects of the pandemic on dentists and patients based on our findings.
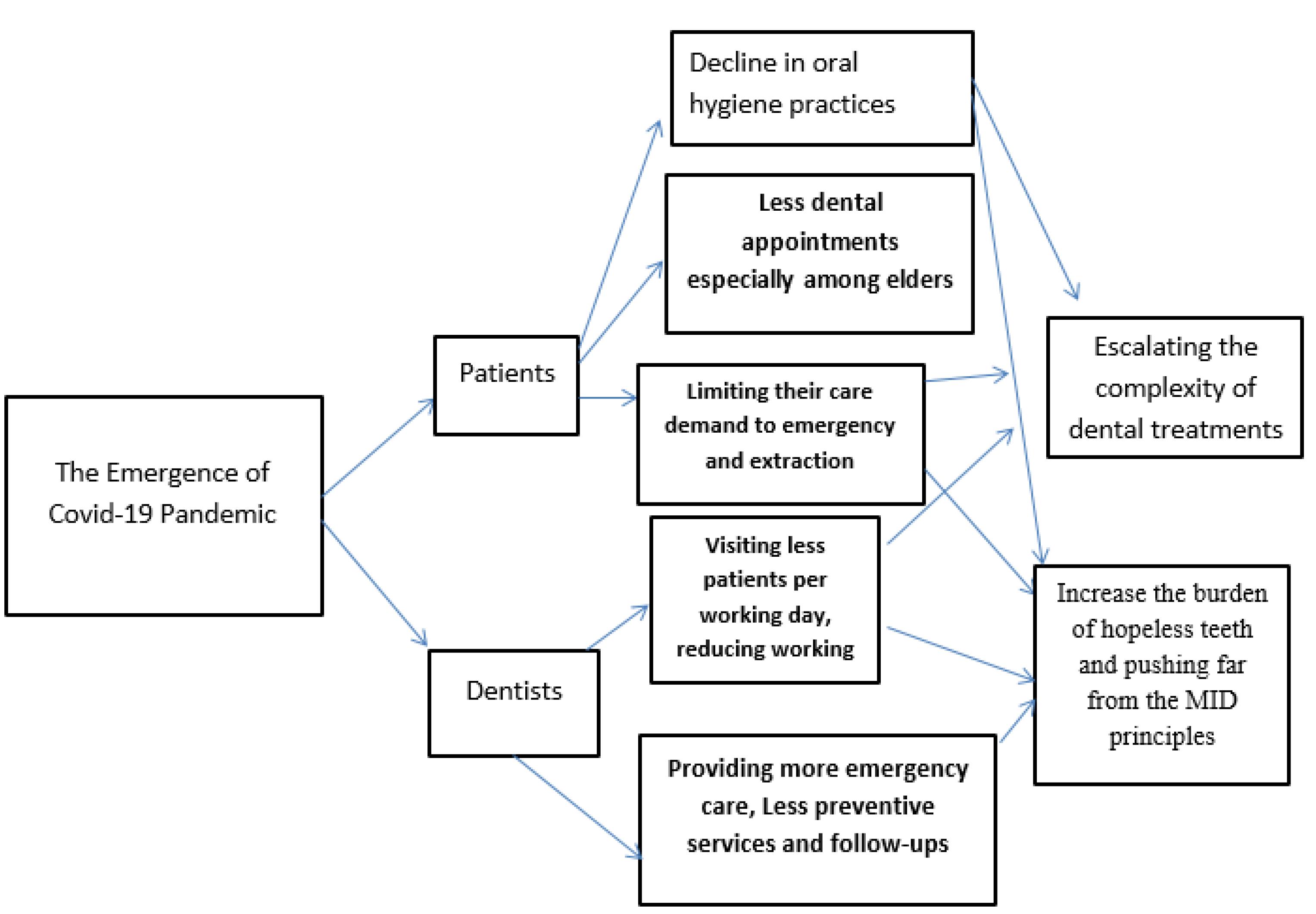
Figure 4.
The Proposed Model of Changes and Their Consequences Based on the Results of the Current Study.
.
The Proposed Model of Changes and Their Consequences Based on the Results of the Current Study.
In our study, the majority of people used teledentistry, and in 91% of cases, WhatsApp was the high-choice media. In the study by Faccini et al (28), 70% of dentists employed Teletriage using the WhatsApp software. There are, however, some challenges regarding the use of Teledentistry among dentists; the difficulty of using these facilities and the need for new skills, fear of misdiagnosis, the poor infrastructure for some people (e.g., poor Internet and lack of sufficient storage space), and inability to use the sense of touch and other complimentary tests can be noted in this regard. In addition, acceptance of this technology by patients is the key to the success of its establishment. Teledentistry cannot completely replace the patient’s presence in the dentist’s office, but it reduces unnecessary visits to the office, thus saving time and money, as well as reducing the risk of transmission of COVID-19 diseases in the dentist’s office (30).
Limitations
Although the current study was one of the most comprehensive studies assessing the different aspects of dentists’ practice schemes during the COVID pandemic in Iran, the results were limited to dentists working in Isfahan. Further, the practice was evaluated based on the dentists’ self-reports. It is recommended that changes in the working scheme of dentists in other provinces should be assessed with different mortality and incidence rates using the same questionnaire.
Conclusions
Pandemic COVID-19 has changed the pattern of dental care. According to the findings of our study, during the COVID-19 pandemic period, dentists provided care to fewer patients, performed more extraction services, emergency pain and abscess treatments, extensive restorations, and endodontic repairs, and reduced preventive treatments such as fissure sealants and fluoride therapy, scaling, and follow-up. The frequency of decayed and hopeless teeth had increased among patients, while oral hygiene behaviors had decreased among patients. Elderly people visited the dentist much less. As a result, the burden of oral disease and edentulousness in society is likely to increase after the pandemic; all these issues are likely to far us away from conservative dentistry. The outbreak of the COVID-19 infection is a warning for our future and should be considered a representative example of other similar situations in which access to dental care will become restricted dramatically. However, Teledentistry has opened a new opportunity to provide dental services.
Acknowledgements
We would like to appreciate the Vice-chancellery of Research at Isfahan University of Medical Sciences for financing support and all the dentists who participated in our study.
Authors’ Contribution
Bahareh Tahani developed the original idea and protocol and analyzed the data. Soroush Talakesh and Ali Foroughi gathered the data and cooperated in the study design. Study supervision was conducted by Pooyan Jadidfard. All the authors cooperated in the writing and final approval of the manuscript.
Competing Interests
None of the authors have any conflict of interests.
Ethical Approval
The design of the study was in accordance with the Helsinki Declaration; it has also been approved by the Ethics Committee in the Vice-chancellery of Research at Isfahan University of Medical Sciences (With the number IR. MUIREC 1400/044/3991.97). Participation in the study was voluntary, and there was no need to include the name.
Funding
This study was a research project (Grant No: 3991097) supported and funded by the Vice-chancellery of Research at Isfahan University of Medical Sciences, Isfahan, Iran.
References
- Mahase E. China coronavirus: WHO declares international emergency as death toll exceeds 200. BMJ 2020; 368:m408. doi: 10.1136/bmj.m408 [Crossref] [ Google Scholar]
- WHO Coronavirus (COVID-19) Dashboard. Available at: https://covid19.who.int/. Accessed March 2023.
- To KK, Tsang OT, Yip CC, Chan KH, Wu TC, Chan JM. Consistent detection of 2019 novel coronavirus in saliva. Clin Infect Dis 2020; 71(15):841-3. doi: 10.1093/cid/ciaa149 [Crossref] [ Google Scholar]
- van Doremalen N, Bushmaker T, Morris DH, Holbrook MG, Gamble A, Williamson BN. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N Engl J Med 2020; 382(16):1564-7. doi: 10.1056/NEJMc2004973 [Crossref] [ Google Scholar]
- Bai Y, Yao L, Wei T, Tian F, Jin DY, Chen L. Presumed asymptomatic carrier transmission of COVID-19. JAMA 2020; 323(14):1406-7. doi: 10.1001/jama.2020.2565 [Crossref] [ Google Scholar]
- Guo J, Xie H, Liang M, Wu H. COVID-19: a novel coronavirus and a novel challenge for oral healthcare. Clin Oral Investig 2020; 24(6):2137-8. doi: 10.1007/s00784-020-03291-8 [Crossref] [ Google Scholar]
- Coulthard P. Dentistry and coronavirus (COVID-19) - moral decision-making. Br Dent J 2020; 228(7):503-5. doi: 10.1038/s41415-020-1482-1 [Crossref] [ Google Scholar]
- Stangvaltaite-Mouhat L, Uhlen MM, Skudutyte-Rysstad R, Szyszko Hovden EA, Shabestari M, Ansteinsson VE. Dental health services response to COVID-19 in Norway. Int J Environ Res Public Health 2020; 17(16):5843. doi: 10.3390/ijerph17165843 [Crossref] [ Google Scholar]
- Spagnuolo G, De Vito D, Rengo S, Tatullo M. COVID-19 outbreak: an overview on dentistry. Int J Environ Res Public Health 2020; 17(6):2094. doi: 10.3390/ijerph17062094 [Crossref] [ Google Scholar]
- Goswami M, Chawla S. Time to restart: a comparative compilation of triage recommendations in dentistry during the COVID-19 pandemic. J Oral Biol Craniofac Res 2020; 10(4):374-84. doi: 10.1016/j.jobcr.2020.06.014 [Crossref] [ Google Scholar]
- Shamsoddin E, DeTora LM, Tovani-Palone MR, Bierer BE. Dental care in times of the COVID-19 pandemic: a review. Med Sci (Basel) 2021; 9(1):13. doi: 10.3390/medsci9010013 [Crossref] [ Google Scholar]
- Schwendicke F, Krois J, Gomez J. Impact of SARS-CoV2 (COVID-19) on dental practices: economic analysis. J Dent 2020; 99:103387. doi: 10.1016/j.jdent.2020.103387 [Crossref] [ Google Scholar]
- Daly J, Black EAM. The impact of COVID-19 on population oral health. Community Dent Health 2020; 37(4):236-8. doi: 10.1922/CDH_Dec20editorialDalyBlack03 [Crossref] [ Google Scholar]
- Lyu W, Wehby GL. Effects of the COVID-19 pandemic on children’s oral health and oral health care use. J Am Dent Assoc 2022;153(8):787-96.e2. 10.1016/j.adaj.2022.02.008.
- Cohen L, Manion L, Morrison K. Research Methods in Education. Routledge; 2017.
- Choi SE, Simon L, Riedy CA, Barrow JR. Modeling the impact of COVID-19 on dental insurance coverage and utilization. J Dent Res 2021; 100(1):50-7. doi: 10.1177/0022034520954126 [Crossref] [ Google Scholar]
- Davies A, Howells R, Lee SMG, Sweet CJ, Dominguez-Gonzalez S. Implementation of photographic triage in a paediatric dental, orthodontic, and maxillofacial department during COVID-19. Int J Paediatr Dent 2021; 31(4):547-53. doi: 10.1111/ipd.12773 [Crossref] [ Google Scholar]
- Waltz CF, Bausell BR. Nursing Research: Design, Statistics, and Computer Analysis. FA Davis Company; 1981.
- Ayre C, Scally AJ. Critical values for Lawshe’s content validity ratio: revisiting the original methods of calculation. Meas Eval Couns Dev 2014; 47(1):79-86. doi: 10.1177/0748175613513808 [Crossref] [ Google Scholar]
- Gambarini E, Galli M, Di Nardo D, Miccoli G, Patil S, Bhandi S. A survey on perceived COVID-19 risk in dentistry and the possible use of rapid tests. J Contemp Dent Pract 2020; 21(7):718-22. [ Google Scholar]
- Moharrami M, Bohlouli B, Amin M. Frequency and pattern of outpatient dental visits during the COVID-19 pandemic at hospital and community clinics. J Am Dent Assoc 2022;153(4):354-64.e1. 10.1016/j.adaj.2021.09.007.
- Ball M, Akintola D, Harrington Z, Djemal S. Emergency dental care triage during the COVID-19 pandemic. Br Dent J. 2021:1-5. 10.1038/s41415-021-3379-z.
- Zarif Najafi H, Oshagh M, Pakshir HR, Mohebbi M. Orthodontic treatments provided by general dentists in Shiraz, Iran. J Mashhad Dent Sch 2014; 38(4):375-86. doi: 10.22038/jmds.2014.3149.[Persian] [Crossref] [ Google Scholar]
- Tong NR, Park J, Carlisle S, Poh CF. Characteristics of emergent and essential dental services in university and hospital-based settings during COVID-19 pandemic in Vancouver, Canada. J Can Dent Assoc 2021; 87:l13. [ Google Scholar]
- Carter E, Currie CC, Asuni A, Goldsmith R, Toon G, Horridge C. The first six weeks - setting up a UK urgent dental care centre during the COVID-19 pandemic. Br Dent J 2020; 228(11):842-8. doi: 10.1038/s41415-020-1708-2 [Crossref] [ Google Scholar]
- Wu JH, Lee MK, Lee CY, Chen NH, Lin YC, Chen KK. The impact of the COVID-19 epidemic on the utilization of dental services and attitudes of dental residents at the emergency department of a medical center in Taiwan. J Dent Sci 2021; 16(3):868-76. doi: 10.1016/j.jds.2020.12.012 [Crossref] [ Google Scholar]
- Ahmadi H, Ebrahimi A, Ghorbani F. The impact of COVID-19 pandemic on dental practice in Iran: a questionnaire-based report. BMC Oral Health 2020; 20(1):354. doi: 10.1186/s12903-020-01341-x [Crossref] [ Google Scholar]
- Faccini M, Ferruzzi F, Mori AA, Santin GC, Oliveira RC, de Oliveira RCG. Dental care during COVID-19 outbreak: a web-based survey. Eur J Dent 2020; 14:S14-S9. doi: 10.1055/s-0040-1715990 [Crossref] [ Google Scholar]
- Kranz AM, Chen A, Gahlon G, Stein BD. 2020 trends in dental office visits during the COVID-19 pandemic. J Am Dent Assoc 2021;152(7):535-41.e1. 10.1016/j.adaj.2021.02.016.
- Ghai S. Teledentistry during COVID-19 pandemic. Diabetes Metab Syndr 2020; 14(5):933-5. doi: 10.1016/j.dsx.2020.06.029 [Crossref] [ Google Scholar]